








La quimioterapia adyuvante reduce significativamente las recidivas en el cáncer de colon pN+ (estadio III) y en algunos pN0 (estadio II) con factores de riesgo (pT4, infiltración vascular V1, infiltración perineural Pn1, tumores complicados). Sin embargo, de manera no esperada, un 20-30% de los pN0 presentan recidivas en el seguimiento, lo que hace pensar que es posible que haya afectación ganglionar que haya quedado oculta tras el estudio convencional histológico (EC), y su identificación mediante un superestudio (SE) podría aumentar el número de pacientes que se beneficiarían de quimioterapia adyuvante. No es posible hacer este superestudio de todos los ganglios linfáticos (GL) aislados en la linfadenectomía, pero sí sería factible en un pequeño grupo de GL que fueran representativos del estatus N global (concepto de ganglio centinela [GC]). El objetivo de nuestro trabajo es determinar esa representatividad del GC y analizar el número de pacientes que se supraestadifican tras el SE del GC.
Material y métodosEstudio prospectivo en una serie de pacientes operados por cáncer de colon con intención curativa, a los que se les realiza biopsia selectiva de GC. La identificación del GC se realizó mediante la inyección in vivo del radiotrazador, con aislamiento posterior ex vivo del GC. Tras la extracción de la pieza se toman imágenes del lecho quirúrgico para descartar vías aberrantes de drenaje linfático fuera del área de resección oncológica habitual. Se realizó el EC histológico (tinción con hematoxilina-eosina con secciones convencionales) del resto de GL aislados del mesocolon. En el GC se realizó el EC y además un SE mediante hematoxilina-eosina en cortes seriados, inmunohistoquímica y estudio molecular con la técnica One Step Nucleic Acid Amplification (OSNA®). Se efectuó un estudio de validez diagnóstica de la biopsia selectiva de GC definiendo como falso negativo (FN) a la existencia de un GC negativo en presencia de otros GL afectados (N+), así como una valoración de la supraestadificación conseguida gracias al SE del GC.
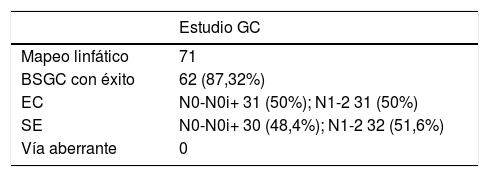
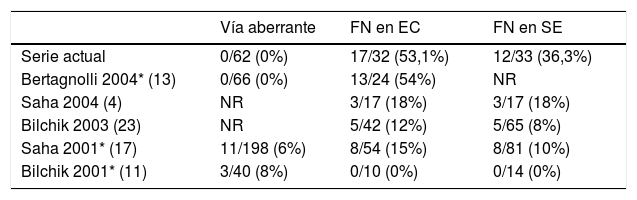
ResultadosSe realizó mapeo linfático en 71 pacientes, detectándose el GC en 62 de los 71 pacientes (87,3%). Los 9 fallos de identificación se concentran en los primeros 17 casos. No hemos encontrado pacientes con drenaje linfático aberrante.
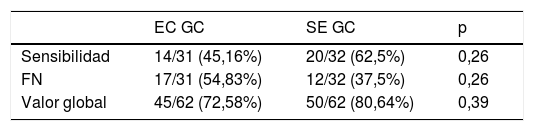
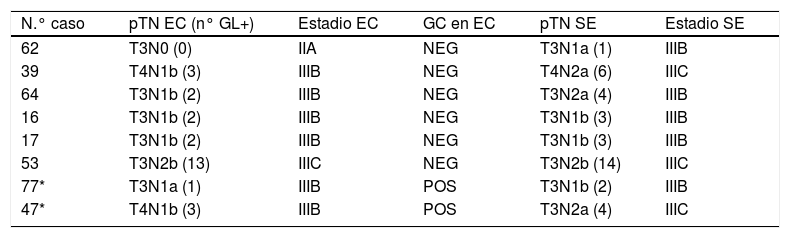
Se estudian un total 1.164 GL en los 62 pacientes (18,8 GL/paciente), de los que 145 son GC (2,34 GC/paciente), encontrándose 103 GL positivos con el EC y 112 positivos con el SE del GC (9 GL+ más en 8 pacientes que los detectados en el EC). La positividad tras el SE en el grupo GC es del 17,24% (25/145) mientras en el resto es del 8,53% (87/1.019) (p <0,001). Con el EC, el 50% de los pacientes (31/62) fueron pN+ (4 son N+ exclusivamente en el GC), y tras el SE del GC, solo uno de los 31 pacientes pN0 (3,2%) se hace pN1a, con un 51,6% definitivo de N+ en el total de pacientes (32 N+ de los 62 pacientes) (5 son N+ exclusivamente en el GC). Exclusivamente con el EC del GC, la tasa de FN («GC-, otros +», es decir, pacientes que son N+ teniendo GC negativo) es del 54,8% (17/31). Con el SE del GC, 8 de los 62 pacientes (12,9%) aumentan el número total de GL afectados: además del paciente que pasa de pN0 a pN1a supraestadificándose de IIA a IIIB (y aumentando el número total de pN+ a 32), 5 de los 17 FN del EC se hacen positivos (dos cambian de subíndice pN y uno se supraestadifica de IIIB a IIIC), reduciéndose los FN al 37,5% (12/32 casos). Además hay otros dos pacientes en los que el GC ya es positivo en el EC, que aumentan el número de GL+ tras el SE del GC, cambiando ambos su subíndice pN y supraestadificándose uno de ellos de IIIB a IIIC. En resumen, 8 pacientes aumentan el número total de GL afectados gracias al SE (8/62, 12,9%), cambiando el subíndice pN en cinco de ellos (5/62, 8%), aunque solo tres de estos se supraestadifican (3/62, 4,8%), entre los que se encuentra el que pasa de pN0 a pN1a.
ConclusiónLa técnica es válida y reproducible, con alta tasa de detección aunque con una clara curva de aprendizaje. Globalmente aumenta el número de GL afectados en un 12,9% de los pacientes, con implicaciones pronósticas en un 4,8% (tasa de supraestadificación). Solo un 3,2% de los pacientes pN0 en el EC pasan a ser pN+ tras el SE del GC, con la correspondiente consecuencia terapéutica (indicación de quimioterapia adyuvante), hallazgo que sería relevante si se extrapola a un gran número de pacientes. La alta tasa de FN (37,5%) impide asumir la representatividad de GC como índice del estatus pN global, pero esto no es trascendente en el CCR ya que su finalidad no es evitar la linfadenectomía, que sigue siendo obligatoria, (al revés que en cáncer de mama o melanoma en los que la detección del GC sí se usa para decidir sobre si se realiza o no la linfadenectomía), sino rescatar casos que pueden beneficiarse de quimioterapia adyuvante.
Adjuvant chemotherapy (CT) significally reduces the rate of relapse in +pN (stage III) colon cancer and in some pN0 (stage II) with risk factors such as pT4, vascular invasion V1, perineural invasion Pn1, and complicated tumors. However, unexpectedly, 20-30% of pN0 present a relapse in the follow-up, which may suggest that the lymph node involvement was not discovered in the conventional histological study (CS), and its finding with a superstudy (SS) could increase the number of patients who would benefit from neoadjuvant CT. It is not possible to perform this SS in every lymph node (LN) from the specimen, but it is possible in a small group of LN which are representative of the N status (definition of sentinel node SN). The aim of our work is to state the representativeness of the SN and to analyze de number of patients who are suprastaged after the SS of the SN.
Material and methodsProspective study of a series of patients who have undergone curative surgery for colon cancer, to whom we perform selective biopsy of sentinel node. Identification of SN was carried out with in vivo injection of the radiotracer, with ex vivo isolation of SN. Once the specimen is out, we take pictures of the surgical bed to rule out the presence of aberrant drainage routes, out of the routine oncological resection area. We performed the histological CS (hematoxilin-eosin stain in conventional sections) in the rest of the LN from the mesocolon. In the SN we performed the CS and a SS with hematoxilin-eosin in serial sections, immunohistochemistry (IHC) and molecular study with One Step Nucleic Acid Amplification (OSNA®). Diagnostic validity study od selective biopsy of sentinel node was carried out, defining the false negative (FN) as the negativity of the SN while other LN are positive (N+), as well as a valuation of the suprastaging due to the SS of the SN.
ResultsWe performed lymphatic map in 72 patients, finding the SN in 62 of them (87.3%). The 9 identification failures happened in the first 17 cases. We have not found aberrant drainage routes. A total of 1.164 LN were studied in the 62 patients (18.8 LN/ patient), from which 145 are SN (2,34 SN/ patient), having found 103 positive LN with the CS and 112 positive with the SS of SN (9 +LN more in 8 patients than detected with the CS). Positivity after CS in the SN group is 17.24% (25/145), while it is 8.53% in the rest (87/1.019) (p<.001). With the CS, 50% of the patients (31/62) were pN+ (4 are N+ exclusively in the SN), and after the SS of the SN, only 1 of the 31 pN0 patients (3.2%) becomes pN1a, with a definitive 51.6% of N+ in the whole series (32 N+ in the 62 patients) (5 are N+ exclusively in the SN).
Exclusively with the SS of the SN, FN rate (“-SN, +others”, meaning patients who are N+ having -SN) is 54.8% (17/31). With the SS of the SN, 8 of the 62 patients (12.9%) increase their total number of +LN: apart from the patient who turns from pN0 to pN1a, suprastaging from IIA to IIIB (and therefore increasing the total number of pN+ to 32), 5 of the 17 FN in the CS turns into positive (2 change the pN subindex and one is suprastaged from IIIB to IIIC), decreasing FN to 37.5% (12/32 cases). Besides, 2 patients whose SN is already positive in the CS increase the number of +SN after the SS of the SN, therefore both changing their pN subindex and one of them suprastaging from IIIB to IIIC. In summary, 8 patients increase the total number of positive SN after the SS (8/62, 12.9%), 5 of them changing the pN subindex (5/62, 12.9%), even if only 3 of them get suprastaged (3/62, 4.8%), among them the one who turns from pN0 to pN1a.
ConclusionTechnique is valid and reproducible, with a high detection rate even with a high learning curve. It globally increases the number of affected LN in 12.9% of patients, having prognostic implications in 4.8% (suprastaging rate). Only 3.2% of pN0 patients in the CS turn to be +pN after the SS of the SN, with its therapeutic implications (prescription of adjuvant CT), which could be relevant when extrapolated to a big number of patients. The high FN rate (37.5%) prevents us from accepting the representativeness of SN as the global N status, but it is not clinically relevant in colon cancer, as its aim is not to avoid lymphadenectomy, which remains mandatory (opposite to breast cancer or melanoma in which SN detection decides upon whether to perform or not the lymphadenectomy), but to decide which patients would benefit from adjuvant CT.
Artículo
Si tiene problemas de acceso puede contactar con la Secretaría Técnica de la SEMNIM en el correo electrónico secretaria.tecnica@semnim.es o en el teléfono: + 34 619 594 780
