







Aunque el carcinoma oncocítico (de células de Hürthle) (COT) se parece al carcinoma folicular de tiroides (CFT), son tumores diferentes derivados de las células foliculares tiroideas. El COT comprende el 3-5% de todos los carcinomas tiroideos diferenciados y tiene un comportamiento más agresivo que el CFT. Los médicos debaten sobre el tratamiento y el pronóstico del COT. Evaluamos sus características clínico-histopatológicas y su evolución clínica.
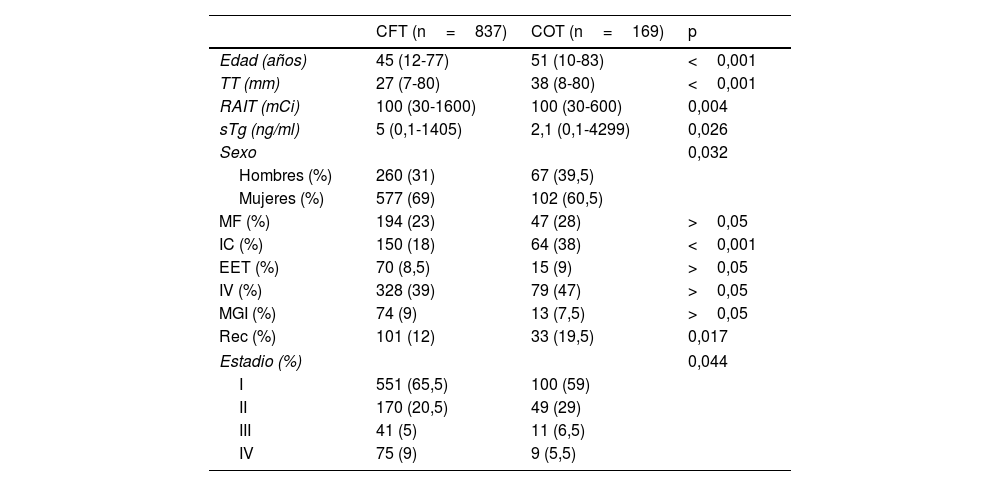
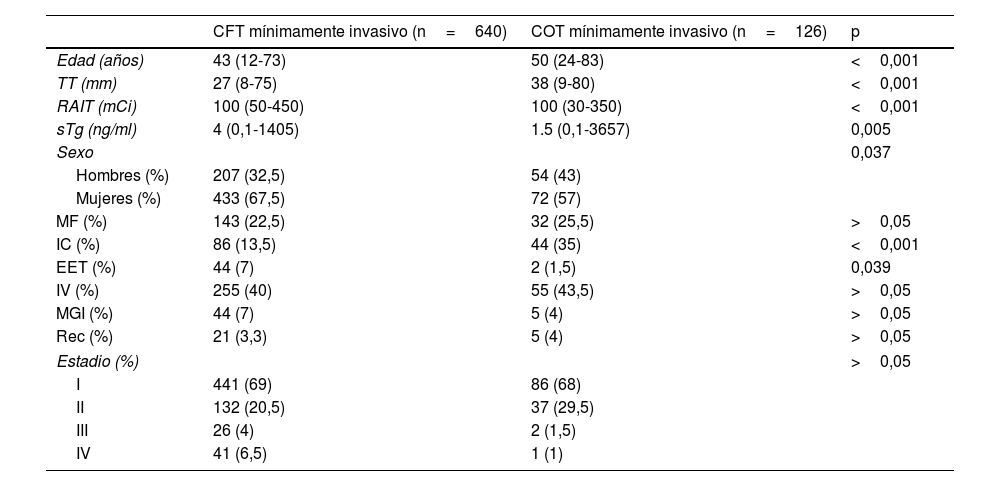
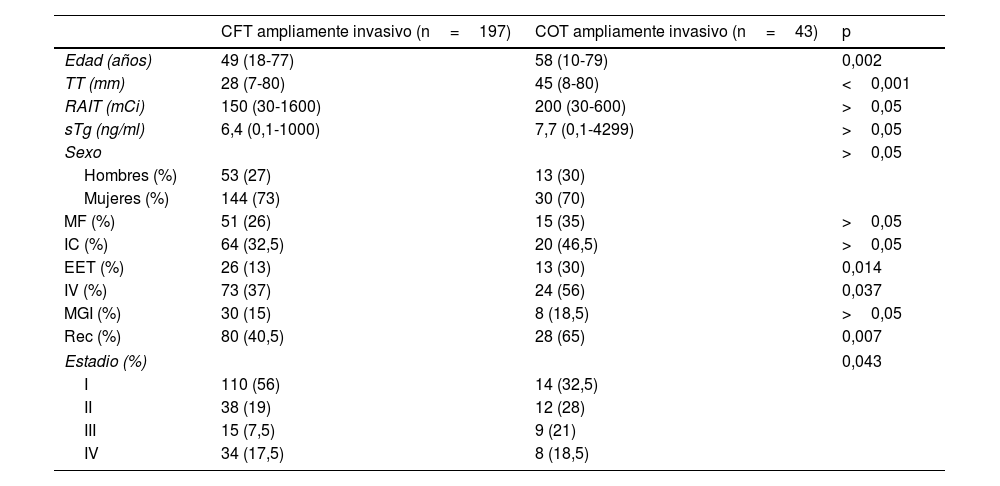
Materiales y métodosExaminamos y realizamos un seguimiento en 169 pacientes con COT (126 mínimamente invasivos, 43 ampliamente invasivos) y 837 pacientes con CFT (640 mínimamente invasivos, 197 ampliamente invasivos). Se compararon COT y CFT según las variables pronósticas, la tasa de recurrencia (Rec) y el resultado. También se determinaron los factores predictores que influyen en la aparición de recurrencia en el COT.
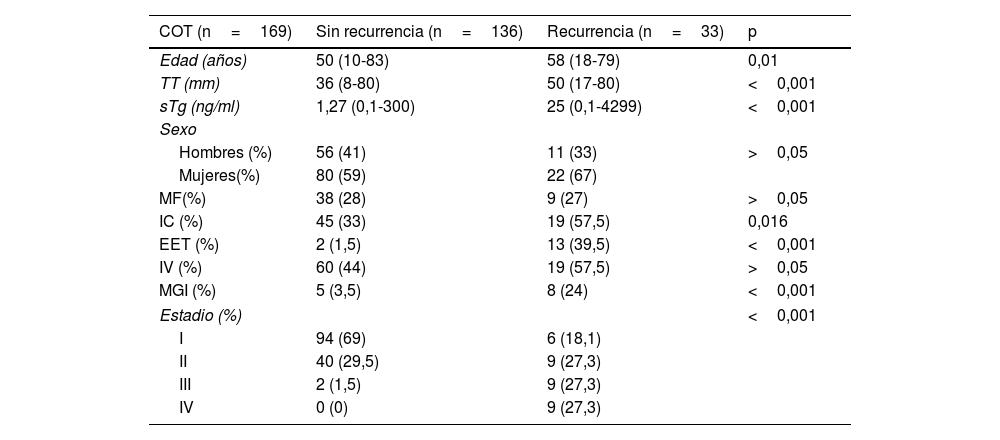
ResultadosHubo diferencias estadísticamente significativas entre COT y CFT en edad, sexo, invasión de cápsula (IC), tamaño tumoral (TT), dosis total administrada de [131I]NaI (RAIT), tiroglobulina estimulada (sTg), Rec y estadio (p<0,001, p=0,032, p<0,001, p<0,001, p=0,004, p=0,026, p=0,017, p=0,044, respectivamente). Edad, IC, extensión extratiroidea (EET), TT, metástasis ganglionar inicial (MGI), sTg y estadio (p=0,01, p=0,016, p<0,001, p<0,001, p<0,001, p<0,001, p<0,001, respectivamente) fueron los predictores de recurrencia en el COT. La incidencia de metástasis fue del 19,5% para COT y del 12% para CFT. En 25 pacientes con CFT (2,8%) y en 11 pacientes con COT (6,5%) la causa de muerte fue oncológica.
ConclusiónEl pronóstico de los tumores COT mínimamente invasivos es bastante favorable, mientras que el de los tumores COT ampliamente invasivos es desfavorable. Se puede administrar radioyodo (RAI) a estos tumores, pero es inútil insistir en dicho tratamiento si no hay respuesta después de la primera terapia adyuvante.
Although oncocytic (Hurthle cell) carcinoma (OTC) resembles to follicular thyroid carcinoma (FTC), they are different tumours derived from thyroid follicular cells. OTC comprises 3-5% of all differentiated thyroid carcinomas and has more aggressive behaviour than FTC. Clinicians discuss about the treatment and prognosis of OTC. We evaluated its clinicopathological features and clinical course.
Material and methodsWe examined and followed up 169 patients with OTC (126 minimally invasive, 43 widely invasive) and 837 patients with FTC (640 minimally invasive, 197 widely invasive). OTC and FTC were compared according to prognostic variables, recurrence rate (Rec) and outcome. The predictor factors impacting on recurrence in OTC were also determined.
ResultsThere were statistically significant differences between OTC and FTC in age, sex, capsule invasion (CI), tumor size (TS), total administered [131I]NaI dose (TID), stimulated thyroglobulin (sTg), Rec and stage (P<.001, P=.032, P<.001, P<.001, P=.004, P=.026, P=.017, P=.044, respectively). Age, CI, extrathyroidal extension (ETE), TS, initial lymph node metastasis (ILNM), sTg and stage (P=.01, P=.016, P<.001, P<.001, P<.001, P<.001, P<.001, respectively) were the predictors for recurrence in OTC. Metastasis incidence was 19.5% for OTC and 12% for FTC. The cause of death was cancer in 25 patients with FTC (2.8%) and 11 patients with OTC (6.5%).
ConclusionThe prognosis of minimally invasive OTC is quite favorable. However the prognosis of widely invasive OTC is unfavorable. RAI may be administered to these tumors, but it is in vain to insist on RAI after the first adjuvant therapy if it does not respond.
Artículo
Si tiene problemas de acceso puede contactar con la Secretaría Técnica de la SEMNIM en el correo electrónico secretaria.tecnica@semnim.es o en el teléfono: + 34 619 594 780
