




Court claims against gynaecologists in the Spanish criminal court system are a rare occurrence (less than 3%). These can lead to financial penalties, imprisonment and disqualification. Our aim is to study the court sentences issued in such cases, as these involve the most serious convictions, and to obtain a profile of those convicted.
Material and methodsA retrospective analysis of the sentences against gynaecologists during the period from 1987 to 2013. We used F-distribution tables, normal distribution tables and Student's t-test to compare differences between groups, and the Mann–Whitney nonparametric test for comparison of independent samples. In order to define two broad groups, those of “convicted” and “not convicted,” we performed a multivariate study analysis followed by cluster analysis to determine similar sentences.
ResultsOf the 85 cases, 56.4% of complaints came from procedures in the public sector, but the highest rate of convictions (59.3%) was based on complaints originating in the private healthcare sector. The likelihood of conviction in events related to childbirth was 36.6% (20 out of 55) versus 16.6% (5 out of 30) in incidents of another origin. 69.2% of cases of criminal proceedings for permanent neurological damage (neonatal encephalopathy) concluded in a criminal conviction and had the highest financial compensation. The average time elapsed between the incident and the sentence was 5.7 years. With a prior conviction, the possibility of confirmation at higher levels was 71.9%. An acquittal was confirmed in 96.2% of cases.
ConclusionsOf the court claims filed against gynaecologists based on their professional activity, very few are decided upon in the criminal courts. Most are due to complications during childbirth, and one-third ends with a conviction. A judgement of acquittal is most likely to be confirmed when this was the case with the previous one.
En España las reclamaciones judiciales contra ginecólogos resueltas por vía penal son escasas, menos del 3%. Esta vía conlleva sanción económica y penas de cárcel y de inhabilitación. El objetivo es estudiar las sentencias resueltas por vía penal, por ser de consecuencias más graves y obtener un perfil del condenado.
Material y métodosAnálisis retrospectivo de las sentencias judiciales penales contra ginecólogos desde 1987 hasta 2013. Hemos utilizado tablas de distribución de Fisher, de normalidad y el t-Test para comparación de diferencias entre grupos y la prueba no paramétrica de Mann-Withney para comparación de muestras independientes. Para la caracterización de dos grandes grupos, el de «condenado» y «no condenado», realizamos estudio multivariante mediante análisis de correspondencias múltiples seguidas de análisis de conglomerados para agrupar.
ResultadosDe 85 casos el 54,6% de las reclamaciones judiciales procedían de actos médicos del sector público, aunque el mayor número de condenas, el 59,3%, lo fue por demandas sobre hechos ocurridos en el ámbito de la sanidad privada. La probabilidad de condena en sucesos relacionados con el parto fue del 36,6% (20 de 55) frente al 16,6% (5 de 30) de episodios de otro origen. En el 69,2% de los casos de procedimientos penales por daño neurológico (encefalopatía neonatal) la sentencia fue condenatoria y con las indemnizaciones más elevadas. El tiempo medio trascurrido entre el incidente y la condena fue de 5,7 años. Con una condena previa, la posibilidad de confirmación en instancias superiores fue del 71,9%. Una absolución se confirmó en el 96,2% de las ocasiones.
ConclusionesAunque es elegida para iniciar el procedimiento pocas reclamaciones se resuelven en vía penal. La mayoría se deben a complicaciones durante el parto y en un tercio se condena. Lo más probable es que se confirme la sentencia previa cuando esta fue absolutoria.
Amongst legal claims against doctors, some specialties, such as obstetrics and gynaecology, stand out because of the large number of doctors involved in them, based on the number of specialists reported, and the high rate of compensation for convictions.
In some countries this increase in claims against gynaecologists is seen as a “crisis” in this specialty.1 In our country there are few scientific publications that cast light on the scope of the problem: one by a group in Catalonia, the insurance brokerage “Uniteco” as well as one by our group,2–4 are the most detailed in this regard. Most of the publications that we consulted and used as references originate from the “American scenario”,5 which is far removed from ours in terms of customs and the health and judicial systems, and which these publications recognise as more expensive and less effective.6
In Spain many claims are initiated in criminal court, because it is a more cost-effective procedure. Also, civil liability, i.e., the amount of financial compensation, is determined in criminal court.7 Here, obstetrics and gynaecology are the medical specialties involved in the most lawsuits, with 15.53% of all claims, below only traumatology and orthopaedic surgery (15.69%). Considered overall, and for cases that go to a court of second instance or supreme court (in all courts), convictions and acquittals represent the same percentage, 50%, in the specialty. Specifically, and again considering all courts, convictions in obstetrics are more likely (57.6%) than they are in gynaecology (42.31%).4
Although criminal court is the route chosen to initiate a legal claim against doctors, it is the most difficult one in which to win a case. Doctors may be unaware of this fact.
In all areas the number of legal claims against doctors is increasing, and this has more relevance in some medical specialties, such as obstetrics and gynaecology, which are always ranked in the top spots (3), as they have the largest number of claims compensated and a higher rate of damages.8
Often the data come from the insurance companies, which use them to conduct risk assessments and thus adjust premiums. This is the case in our country and also in others with more experience in analysing such data.8
Few studies have tackled this subject with a scientific interest. The information that professionals receive may therefore be incomplete, but it is considered sufficient to lead to care-related changes9,10 such as increasing the number of deliveries by caesarean section.11,12
It is also true that these “litigation crises” have been used, together with the lasting interest of medical science, to improve patient safety, help to develop clinical guidelines,13 and implement action protocols.
In our study, we reviewed the judgements in cases related to gynaecology and obstetrics from 1987 to 2013, prosecuted in criminal court. As far as we know, there are no references in the medical literature for this aspect. We believe that convictions in criminal court may have the most influence on any changes in attitude on the part of professionals.
The jurisprudence shows that it is difficult for criminal charges to succeed,14 but, as we mentioned, this causes the professional involved to suffer the most, because with compensation comes the possibility of penalties of disqualification and custodial sentences, along with media coverage.
In principle, criminal court is chosen owing to the economic (almost gratis) and procedural advantages that are aimed at avoiding longer and more expensive proceedings,14 and seeking civil liability derived from criminal conviction. Recourse to criminal court in our specialty is becoming a pressing problem,15 which is why the aim of our study is to define a “convicted-party profile” for cases in criminal court during the study period, trying to differentiate this from civil court, inclined to the legal fact that there should be no prejudice without reparation,15 and the real cause of the increase in decisions regarding civil liability cases against doctors.
We need our own data to compare with those from other countries, mainly the United States, whose health and judicial systems are very different from European standards and, more specifically, those of our country.
Material and methodsWe mainly used the Westlaw Aranzadi database of decisions, accessing it from the School of Legal Medicine at the Complutense University of Madrid. We collected all decisions in medical malpractice cases against gynaecologists, for medical procedures that occurred after 1987 with a decision published before May 2013, made in criminal court and which reached at least a court of second instance or supreme court, i.e., Provincial Court, Superior Court of Justice, or Supreme Court. This database contains the full decisions. The variables of our study were: adverse effect; the party affected by the damage claimed: mother, foetus or newborn, or patient in the case of gynaecological surgery; type of surgery; and other data such as the year of the event, the time elapsed between the event and the publication of the final decision, and the scope of the medical activity, whether public or private.
We also assessed whether the final decision was upheld or went against that of the previous instance court and, in case of conviction, the amount of compensation.
Our main goal was to determine the “convicted-party profile”. We divided the total number of cases into two large groups, those related to childbirth and those related to other procedures particular to obstetrics and gynaecology, and then sub-classified them by most common adverse events, as reported in previous publications.
For the amounts awarded for compensation, we only performed a descriptive analysis.
We used SPSS 19.0, Fisher's exact test, normal tables and a t-test to compare the differences between groups. We also used the non-parametric Mann–Whitney U test to compare independent samples.
The multivariate analysis was performed using SPAD 7.0. and the analysis of multiple correspondences was followed by a cluster analysis to obtain decisions that were similar in terms of conviction, childbirth and others, and scope. The characterisation of these homogeneous groups for these and other variables was also performed to characterise two large groups: “conviction” and “no conviction”.
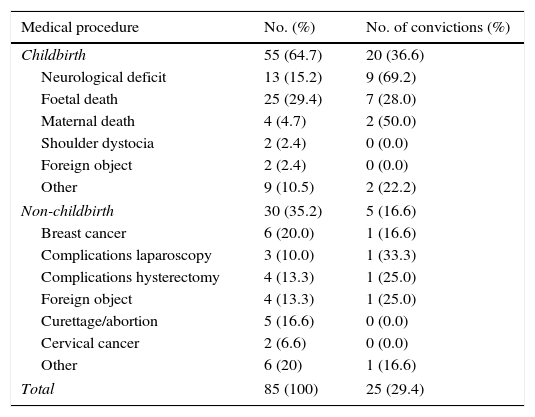
ResultsOf the total of 85 decisions, Table 1 summarises the origin of the claim, its relationship or not with childbirth, and the outcome. Most of the claims concerned complications arising from childbirth—related to foetal harm (55), death of the newborn (25), or due to residual neurological damage (13). In the latter case, 69.2% of the claims ended in conviction, with the same result obtained in 28% of the cases of foetal death. Claims not related to complications during childbirth and heard in criminal court accounted for 30 in total. Of these, 6 (7%) were related to diagnostic delays of breast cancer, 3 (3.5%) to complications during laparoscopic surgery, and 4 (4.7%) to hysterectomy. As regards another surgical complication, we found 6 cases (7%) where a foreign object had been left inside the patient's body: 2 related to childbirth, and 4 to other surgical procedures, with only one case being a conviction.
Source of lawsuit and outcome.
| Medical procedure | No. (%) | No. of convictions (%) |
|---|---|---|
| Childbirth | 55 (64.7) | 20 (36.6) |
| Neurological deficit | 13 (15.2) | 9 (69.2) |
| Foetal death | 25 (29.4) | 7 (28.0) |
| Maternal death | 4 (4.7) | 2 (50.0) |
| Shoulder dystocia | 2 (2.4) | 0 (0.0) |
| Foreign object | 2 (2.4) | 0 (0.0) |
| Other | 9 (10.5) | 2 (22.2) |
| Non-childbirth | 30 (35.2) | 5 (16.6) |
| Breast cancer | 6 (20.0) | 1 (16.6) |
| Complications laparoscopy | 3 (10.0) | 1 (33.3) |
| Complications hysterectomy | 4 (13.3) | 1 (25.0) |
| Foreign object | 4 (13.3) | 1 (25.0) |
| Curettage/abortion | 5 (16.6) | 0 (0.0) |
| Cervical cancer | 2 (6.6) | 0 (0.0) |
| Other | 6 (20) | 1 (16.6) |
| Total | 85 (100) | 25 (29.4) |
In all, 36.6% of the legal claims related to childbirth ended in a conviction, compared with 16.6% of the rest.
When the original decision was a conviction, the most probable outcome was that the decision would be affirmed by the supreme court (72% of cases); however, the likelihood of an acquittal being affirmed was higher (96.2%).
Obstetrics requires close collaboration between doctor and midwife, which is a significant responsibility. We therefore studied the professional against whom the claim was made: against only the doctor in 60 cases (70%), the doctor and midwife in 15 cases (17%), and only the midwife on 8 occasions (9.6%). In the last two situations, the likelihood of conviction was slightly higher (37.5%) compared with 28.3% in the first situation.
Public healthcare accounted for 56.4% of the claims, but only 48% of convictions, vs 38.8% and 59.3%, respectively, in the private sector.
Regarding the temporal distribution, we found a cluster of cases between 1995 and 2004, with a “peak” in 2002, and what seems to be a rebound in 2009 (Fig. 1).

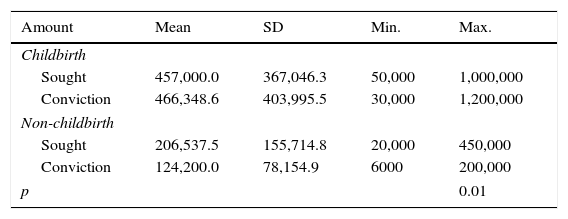
In the 25 convictions we analysed the amounts sought and the compensation awarded. The highest amounts were due to reports of complications during childbirth, with an average of €457,000, compared with the rest, i.e., an average of €124,200 (Table 2).
Amounts awarded in compensation.
| Amount | Mean | SD | Min. | Max. |
|---|---|---|---|---|
| Childbirth | ||||
| Sought | 457,000.0 | 367,046.3 | 50,000 | 1,000,000 |
| Conviction | 466,348.6 | 403,995.5 | 30,000 | 1,200,000 |
| Non-childbirth | ||||
| Sought | 206,537.5 | 155,714.8 | 20,000 | 450,000 |
| Conviction | 124,200.0 | 78,154.9 | 6000 | 200,000 |
| p | 0.01 | |||
Amounts in euros. We have given raw amounts in today's currency, but no correcting factor has been applied to older rates.
The time elapsed from the year of the event to the issuance of the decision was 5.7 years on average, although there was a very wide range of 2–15 years due to a few outliers, regardless of whether the decision was to convict or not.
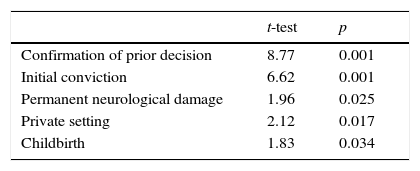
The multivariate analysis (Table 3) shows that the following factors greatly influence the likelihood of conviction: prior conviction; permanent neurological damage in a newborn or related to childbirth in general as a reason for the claim; and whether the event occurred in a private setting.
DiscussionIn our study, the events occurring during childbirth—compared with those occurring outside it—, events occurring in a private setting, events related to permanent neurological damage, and events in which the prior decision was to convict were the factors that mainly contributed to the “convicted-party profile”.
The more specific analysis of criminal proceedings (court of second instance or supreme court) shows that the percentage of convictions is 29.4%.
More specifically, in the same level of criminal courts the percentage of convictions was 36.6% in obstetrics and 16.6% in gynaecology. Considering proceedings overall, the percentage of convictions would be 57.69% and 42.31%, respectively.
Research in our setting and in others that refer to decisions published from criminal proceedings is rare, which makes comparisons difficult. One publication by a French insurer16 distinguishes “criminal and civil jurisdiction”, and the legal system there is comparable. In cases related to obstetrics regarding decisions in 2006, the percentage of convictions was 75% (8 claims) in criminal court and 49% (39 claims) in civil court.
Our study, which includes 85 decisions issued in criminal court over a 25-year period (we do not know the total number of lawsuits), shows that although this is the most common route (i.e., criminal court), cases are rarely concluded in it, and if professionals knew this fact, they might view their “presence” before the judge with less anxiety.
Regarding the “convicted-party profile” in criminal court, the likelihood of being convicted is greater when: the legal claim concerns medical procedures carried out in private centres (59.3% of convictions in 33 cases) than in public centres (48% in 48 cases); the claim involves adverse events during childbirth (36.6% convictions in 55 cases); and the cause is due to neurological damage in a newborn (69.9% convictions in 13 suits). This fact seems to be revealing because it often happens that the relationship between encephalopathy or neonatal asphyxia and obstetric malpractice is questioned. Although the reasons may be multifactorial,17 there is a significant number of such events that can be attributed to or develop during childbirth,18 and claims have a higher chance of conviction in criminal court.
The 20 convictions for events related to childbirth and the 5 for other causes over the 25-year period covered by our study (1987–2013) do not allow for an analysis of the amounts awarded in evolutionary or comparative terms. But from the maximum and minimum amounts from the compensations awarded, we can conclude with other authors working in Spain19 that practically all catastrophic compensation—defined in Spain as amounts over €200,000—is due to events during childbirth. Although in their case series these events represent 5.8% of the total, in our series it was 80% of convictions (20 of 25). This study and other articles16,20 support the fact that obstetrics features the highest amounts of compensation, and therefore those that exceed €1,000,000, which also happened in our case. The range in our sample was between €6000 and €1,200,000, compared with €200,775 and €74,331,098 in the above-cited research.19 These differences are justified by the temporal range: 25 years vs 6 years. This is not comparable; nor is the number of convictions (25 vs 550) or the legal route studied.
The amount awarded and the severity of the injury are related, but we believe it more likely that convictions in criminal court have a greater influence on changes in care than do those that are only financial, however high they may be. In addition, only 5% of criminal claims made against doctors reach the stage of prosecution,21 and in this specialty they are due mainly to adverse events during childbirth and end in acquittal, especially if the original ruling was one of acquittal. This information could help to influence this type of medicine “to prevent lawsuits” or for “defensive medicine”, though this is not known. This was another goal of our study, i.e., to cast light on how difficult it is for a lawsuit started in criminal court to end with a decision in that sphere.
The differences found between the public and private settings in our study should be interpreted by taking into account the important changes that have occurred in recent years in the standards of care of private medicine in certain areas of Spain.
ConclusionsCases of residual neurological damage in a newborn have the highest probability of seeing a conviction, and the conviction is harsher. The percentage of criminal claims that reach a court of second instance or supreme court is low, and here the likelihood of conviction is lower than in civil court, regardless of whether it involves a doctor or a midwife.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: García-Ruiz N, Santiago-Sáez A, Albarrán-Juan ME, Labajo-González E, Perea-Pérez B. Análisis de reclamaciones judiciales contra obstetras y ginecólogos en España. Estudio específico de la vía penal (1987-2013). Rev Esp Med Legal. 2016;42:136–141.