












In recent decades, vitamin D has been extensively researched in relation to several autoimmune diseases, including Rheumatoid Arthritis (RA).
ObjectiveThe primary objective of this study is to investigate the relationship between RA and polymorphism in vitamin D receptor gene Cdx2 in a sample of women.
MethodsEighty females (60 with RA and 20 controls) participated in this case–control investigation. The Cdx2 single nucleotide polymorphism (SNP) of the VDR gene was genotyped using the tetra-primer amplification refractory mutation system-polymerase chain reaction technique (ARMS-PCR).
ResultsThe current study found that 51 RA patients have the heterozygous GA genotype of the Cdx2 polymorphism despite non-significant values. Although the present findings showed no significant association between Cdx2 gene polymorphism and the risk of RA, this genotype still represents the majority among the study's RA patients. Moreover, vitamin D3 serum was significantly lower in RA with the GA genotype compared to healthy controls (HC) with a similar genotype (p=.0002). Also, RA patients with heterozygote GA genotype for Cdx2 had a relatively lower mean VD3 serum level than those with homozygote GG genotype.
ConclusionThe novelty of this study is to discover the probable association of Vitamin D receptor, caudal-related homeobox 2 (VDR-Cdx2) polymorphism with RA in the given study group for the first time in our society using a tetra primer ARMS-PCR. Additionally, the tetra-primer ARMS-PCR technique is simple, reliable, and cost-effective, making it a potentially valuable alternative to Restriction Fragment Length Polymorphism-Polymerase Chain Reaction (RFLP-PCR) for (SNP) genotyping.
En las últimas décadas, la vitamina D ha sido ampliamente investigada en relación con varias enfermedades autoinmunes, incluida la artritis reumatoide (AR).
ObjetivoEl objetivo principal de este estudio es investigar la relación entre la AR y el polimorfismo en el gen Cdx2 del receptor de vitamina D en una muestra de mujeres.
MétodosOchenta mujeres (60 con AR y 20 controles) participaron en esta investigación de casos y controles. Se genotipificó el polimorfismo de un solo nucleótido (SNP) Cdx2 del gen VDR, utilizando la técnica de reacción en cadena de polimerasa del sistema de mutación refractaria de amplificación de tetra-cebador (ARMS-PCR).
ResultadosEl estudio actual encontró que 51 pacientes con AR tienen el genotipo GA heterocigoto del polimorfismo Cdx2, a pesar de los valores no significativos. Aunque los hallazgos actuales no mostraron una asociación significativa entre el polimorfismo del gen Cdx2 y el riesgo de AR, este genotipo aún representa la mayoría entre los pacientes con AR del estudio. Además, el VD3 sérico fue significativamente menor en AR con el genotipo GA, en comparación con los controles sanos con un genotipo similar (p=0,0002). Además, los pacientes con AR con genotipo GA heterocigoto para Cdx2 tuvieron una media relativamente menor para el nivel sérico de vitamina D3 que aquellos con genotipo GG homocigoto.
ConclusiónLa novedad de este estudio es descubrir la probable asociación del polimorfismo del receptor de vitamina D, homeobox 2 relacionado con el caudal (VDR-Cdx2) con AR en el grupo de estudio, por primera vez en nuestra sociedad, utilizando un tetraprimer ARMS-PCR. Además, la técnica ARMS-PCR de tetra-cebador es simple, confiable y rentable, lo que la convierte en una alternativa potencialmente valiosa a la reacción en cadena de la polimerasa por polimorfismo de longitud de fragmentos de restricción (RFLP-PCR) para la genotipificación (SNP).
Due to the increased risk of developing RA in individuals with inherited genetic risk factors exposed to environmental triggers, environmental and genetic factors interact to cause RA. The likelihood of developing RA is affected by various environmental factors, including tobacco smoke, occupational exposure, infectious diseases, hormones, and diet [1,2]. According to Jiang and Alfredsson [3], one of the environmental elements contributing to the development of RA may be VD3. Recent research indicates that low serum levels of Calcidiol (25OHD) play a role in RA's pathogenesis and affect its clinical manifestations [4]. Additionally, in their research, Lee and Bae [5] discovered an inverse connection between the severity of RA disease and VD3 levels.
Due to osteoporosis symptoms in RA patients, physicians recommended VD3 supplements as a treatment [6]. VD3 is a significant endocrine mediator with immunomodulatory characteristics. Over the last 20 years, it has been found to have a close relationship with immune responses. It is understood that VD3 has pleiotropic anti-inflammatory effects and directly contributes to the expression of VD receptors on various immune cells, including macrophages, dendritic cells, and lymphocytes [7]. Coupled with the discovery that low VD3 levels and VD deficiency are standard in RA patients, VD may act as a preventative factor against the disease [8,9]. VD possess anti-inflammatory and immunomodulatory roles, and its deficiency has been correlated with many autoimmune syndromes, including RA; its deficiency is more prevalent in RA patients and may be one of the reasons for the disease's development [10].
The RA disease lacks a pathognomonic laboratory test, making early diagnosis challenging. A comprehensive clinical approach is crucial for accurate diagnosis and to prevent debilitating joint impairment. Furthermore, RA requires various combined diagnostic techniques, including patient history, physical examination, blood tests, and imaging analysis [11,12].
The frequencies of the GG, GA, and AA genotypes for specific polymorphisms in the Iraqi population can vary depending on the specific gene being studied. For example, one study on prothrombin gene polymorphism (G20210A) found the following frequencies among Iraqi patients: GG (88%), GA (10.66%), and AA (1.333%) [13]. For the VKORC1 (−1639G>A) rs9923231 polymorphism, the frequencies were GG (83.33%), GA (14.86%), and AA (1.8%) [14].
Recently, Polymorphic variants of the VD Receptor Gene (VDR) such as (FokI), (TaqI), (ApalI), and (BsmI) have been investigated in RA patients. According to earlier studies, these polymorphisms increase the likelihood of developing RA [15,16].
Another VDR gene polymorphism that may influence the susceptibility of inflammatory diseases like RA is Caudal-type Homeobox Protein 2 (Cdx2) [17]. The most extensively studied VDR polymorphisms in this region include TaqI, FokI, ApaI and BsmI [18–20]. Moreover, there is a notable lack of research on the polymorphism of VDR genes among RA patients in the provinces of Kurdistan, Iraq. Recognizing this gap in the existing literature, the present study was designed to highlight the prevalence and significance of this polymorphism, particularly among women affected by RA in the region.
MethodsStudy participantsInclusion criteriaFemale patients aged 22–60 years. Diagnosed with rheumatoid arthritis (RA). Attended the Department of Rheumatology and the Medical Rehabilitation Centre of Biological Therapy for Rheumatic Disease at Rzgary Teaching Hospital, Erbil—comparison with an age- and sex-matched control group of healthy subjects. Peripheral blood samples were collected from all participants.
Exclusion criteriaIncluded women with other autoimmune diseases, such as diabetes mellitus type 1, osteoporosis, and multiple sclerosis, as well as patients older than 60 years and pregnant females.
Ethical considerationsBefore collecting the samples, ethical approval was obtained in accordance with the Helsinki Agreement from the ethical committee of the Science Faculty at Soran University, reference number 1/1/178 on 15/11/2021. Patients were informed that blood samples would be collected solely for research purposes, with assurances of anonymity. Informed consent was obtained from each patient, who willingly signed a consent form demonstrating their voluntary participation in the study.
Sample collectionPeripheral blood samples were collected from patients and HC. Blood samples were obtained from sixty women in the patient group and twenty age- and sex-matched healthy women in the control group. For each participant, 5ml of peripheral blood was collected:
- •
3ml of blood was placed in a serum separation tube (gel tube).
- •
For molecular work, 2ml of blood was placed in an Ethylenediaminetetraacetic acid (EDTA) tube.
The samples were centrifuged for 15min at 3000rpm to separate the serum and then stored at −20°C pending further analysis.
ELISA analysisAnti-CCP and VD3 levels in the sera of RA patients and HC were assessed using enzyme-linked immunosorbent assays (ELISA).
An ELISA kit (DIAGNOSTIC AESKULIZA CCP, REF 3166, Wendelsheim, Germany) was used to determine the serum level of IgG antibodies to specific cyclic citrullinated peptides, following the manufacturer's instructions.
The serum level of human VD3 was measured using a Human Direct AccuBind ELISA kit (Monobind Inc, Lake Forest, CA, USA, product code: 9425-300) based on the competitive ELISA method, adhering to the manufacturer's instructions. Based on the sandwich method, the serum level of interleukin 17 (IL-17) in the study subjects was estimated using Human (IL-17) ELISA Kit, Sun Long Biotech, China.
DNA extractionDNA was extracted from the whole blood samples using the ReliaPrep™ Blood gDNA Miniprep System (Promega) DNA Extraction kit, following the manufacturer's protocol. The quality and concentration of the extracted DNA were evaluated using a Nanodrop spectrophotometer and by measuring the 260/280 and 260/230 ratios.
Health status questionnaireAll participants completed a health status questionnaire to confirm their diagnosis, which included information on age, BMI, drug type, time since disease diagnosis, and family history.
Cdx2 gene polymorphism detection by tetra-ARMS PCRThe detection of Cdx2 (rs11568820) gene polymorphism in all samples was carried out using two pairs of primers: outer primers (outer forward and outer reverse) and inner primers (inner forward and inner reverse). The primers were specifically designed for this study using a design tool https://primer1.soton.ac.uk/primer1.html. The primer sequences used in VDR rs11568820 analysis by tetra primer ARMS-PCR are shown in Table 1. The primers were synthesized by Macrogen and shipped in a lyophilized state, with the quantity provided in picomoles. The primer sequences utilized in the VDR rs11568820 analysis by tetra primer ARMS-PCR are detailed in Table 1. Before opening the cap, the tube was spun down. Then, 250μL of Nuclease-Free Water was added to each lyophilized primer to achieve a concentration of 100μM. After preparation with Nuclease-Free Water (NFW), the mixture was thoroughly mixed using a microcentrifuge for 2min to obtain a master stock from each primer. The primers were then diluted at a 1:10 ratio using Nuclease-Free Water to create a working stock for PCR product preparation. The master stock was stored at −20°C, and the working stock was stored at −8°C. Primers were distributed into single-use aliquots to limit freezing-thawing cycles, thus extending their shelf life.
The primer sequence of the Cdx2 gene used in the tetra-primer ARMS-PCR method.
| Gene | Primer sequence | Reference |
|---|---|---|
| Inner forward | GCAACCCATAATAAGAAATAAGTTTTGAC | Specifically designed for this study. Cdx2 rs11568820 |
| Inner reverse | ATATTCCTGAGTAAACTAGGTCAAAA | |
| Outer forward | AAACACACGTTAAGTTCAGAAAGATT | |
| Outer reverse | AAAGAAAGAGAGAAAGGAAGAAAAAG |
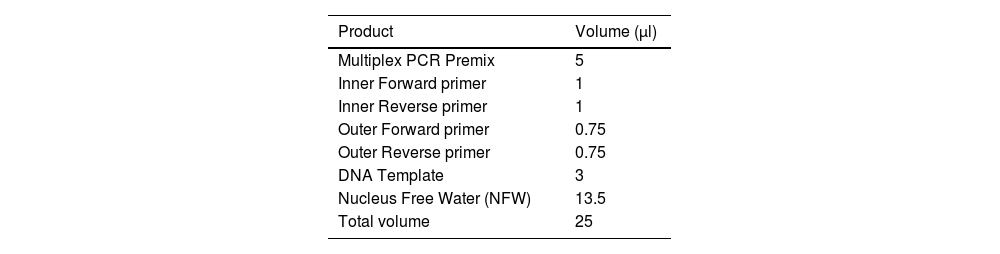
The ingredients and volumes for a single tetra-primer ARMS PCR reaction are illustrated in Table 2.
Ingredients and the reference volume of a single reaction of tetra-ARMS PCR used to detect Cdx2 gene polymorphism.
| Product | Volume (μl) |
|---|---|
| Multiplex PCR Premix | 5 |
| Inner Forward primer | 1 |
| Inner Reverse primer | 1 |
| Outer Forward primer | 0.75 |
| Outer Reverse primer | 0.75 |
| DNA Template | 3 |
| Nucleus Free Water (NFW) | 13.5 |
| Total volume | 25 |
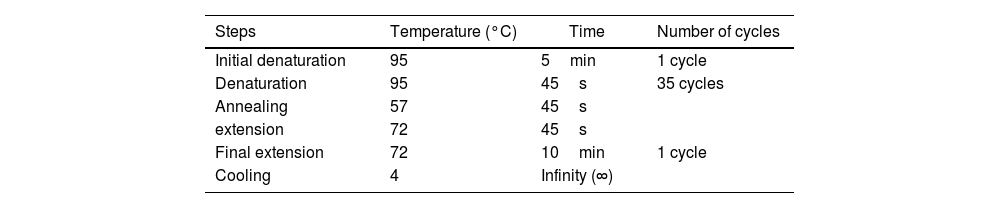
The thermal cycler condition used to detect Cdx2 gene polymorphism can be found in Table 3.
Thermal cycler conditions for Cdx2 gene polymorphism detection, using applied biosystems gene amp PCR system 9700.
| Steps | Temperature (°C) | Time | Number of cycles |
|---|---|---|---|
| Initial denaturation | 95 | 5min | 1 cycle |
| Denaturation | 95 | 45s | 35 cycles |
| Annealing | 57 | 45s | |
| extension | 72 | 45s | |
| Final extension | 72 | 10min | 1 cycle |
| Cooling | 4 | Infinity (∞) |
First, a normality test was used to statistically analyze the data, followed by a non-parametric test (Mann–Whitney Confidence Interval). The mean and standard error were determined, and frequencies were estimated using gene counting. The odds ratio (OR) and the 95% confidence interval (CI) for the detected genotypes were calculated using online tools. https://www.medcalc.org/odd_ratio.php.
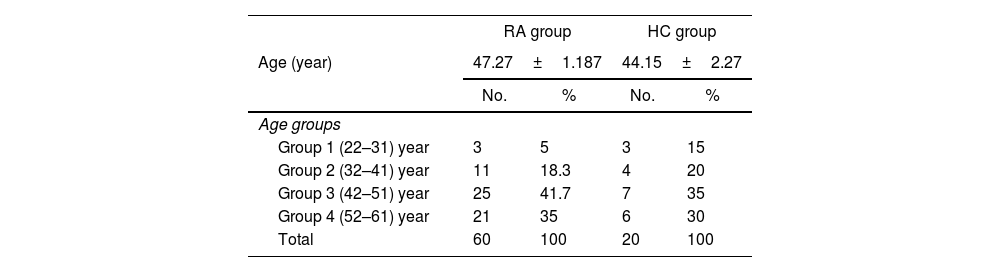
ResultsDemographic and clinical dataThe study revealed that the mean age for the RA group was 47.27±1.187 years, while the HC group had a mean age of 44.15±2.27 years. Among RA patients, 41.7% were in the 42–51 age group, which was the largest, comprising 25 women. The next largest group was the 52–61 age group, with 21 patients, and the smallest was the 22–31 age group, with only three patients (5%). Additionally, 60% (36) of RA patients were post-menopausal, 28.3% were premenopausal, and 11.7% (7) had their ovaries removed.
Regarding body mass index (BMI), 45% (27) of women with RA were in the normal weight category (18.5–24.9). Out of the total patients, 36% (22 women) were found to be overweight. In contrast, the remaining patients fell into the following categories: underweight (<18.5) with 7 cases, obese (30–34.9) with 3 cases, and severely obese (35–39.9) with 1 case. In contrast, the HC group generally weighed a normal amount. The average duration of illness among RA patients was 12±2.16 years, ranging from 1 to 39 years. Furthermore, 51.7% (31) of RA patients had a familial history of the illness, while 48.3% (29) did not.
As per the doctor's diagnosis and questionnaires, 45% (27 out of 60) of the women with RA were prescribed VD3 to address VD deficiency, while 55% (33) did not receive VD3. The study also indicated that 68.3% (41) of women with RA received biological therapy, whereas 31.7% (19) were not. Most RA patients, 86.7% (52), were administered anti-rheumatoid drugs, while the remaining 13.3% (8) were not. Enbrel injection was a commonly used form of biological therapy. Physicians also recommended antirheumatic medications such as methotrexate and hydroxychloroquine as Disease-Modifying Antirheumatic Drugs (DMARDs) for treating RA. Detailed information on the demographic data of participants in both groups (patients and controls) is shown in Table 4.
Detailed information on the demographic data of participants in both groups (patients and controls).
| RA group | HC group | |||
|---|---|---|---|---|
| Age (year) | 47.27±1.187 | 44.15±2.27 | ||
| No. | % | No. | % | |
| Age groups | ||||
| Group 1 (22–31) year | 3 | 5 | 3 | 15 |
| Group 2 (32–41) year | 11 | 18.3 | 4 | 20 |
| Group 3 (42–51) year | 25 | 41.7 | 7 | 35 |
| Group 4 (52–61) year | 21 | 35 | 6 | 30 |
| Total | 60 | 100 | 20 | 100 |
| No. | % | No. | % | |
|---|---|---|---|---|
| BMI (kg/m2) | ||||
| Underweight<18.5 | 7 | 11.7 | 5 | 25 |
| Standard weight, 18.5–24.9 | 27 | 45 | 13 | 65 |
| Overweight 25–29.9 | 22 | 36.7 | 2 | 10 |
| Obese 30–34.9 | 3 | 5 | 0 | 0 |
| Severe obese 35–39.9 | 1 | 1.7 | 0 | 0 |
| Total | 60 | 100 | 20 | 100 |
| Menopausal period | ||||
| Premenopausal | 17 | 28.3 | 16 | 80 |
| Postmenopausal | 36 | 60.0 | 4 | 20 |
| Ovary removed | 7 | 11.7 | – | – |
| Total | 60 | 100 | 20 | 100 |
| Patients and RA family history | ||||
| 1st-degree relatives | 28 | 46.7 | – | – |
| 2nd-degree relatives | 3 | 5 | – | – |
| No family history | 29 | 48.3 | – | – |
| Total | 60 | 100 | – | – |
| Type of drugs | ||||
| Biological therapy | 41 | 68.3 | – | – |
| Anti-rheumatoid drugs | 52 | 86.7 | – | – |
| Vitamin D3 supplement | 27 | 45 | – | – |
| Duration of disease(Years) | 12±216 | – | – | |
| Comorbidities | ||||
| Type 1 diabetes | 11 | 18.3 | – | – |
| Type 2 diabetes | 1 | 1.7 | – | – |
| Hypothyroidism | 4 | 6.7 | – | – |
| Asthma | 4 | 6.7 | – | – |
| Allergy | 2 | 3.3 | – | – |
| Psoriasis | 3 | 5.0 | – | – |
| No comorbidity | 35 | 58.3 | – | – |
| Total | 60 | 100 | ||
Regarding the DNA quality assessment by NanoDrop, our results included both concentration(ng/ml) and the ratio of 260/280nm for the purity of samples. The resulting DNA concentration ranged between (16.13ng/μl and 151.89ng/μl), all falling within the range of good purity for 260/280nm as (1.8–1.82).
The VD3 Genotyping in RA was accomplished using Tetra-ARMS PCR, and the Cdx2 gene polymorphism was amplified. Subsequently, 2% agarose gel electrophoresis was used to visualize the PCR products.
The Cdx2 gene polymorphism genotype was associated with both RA patients and the HC group. The VD Cdx2 polymorphism results showed that the GG genotype was detected in 7 (12.07%) of RA samples, while in the HC groups, the GG genotype was found in only 3 (15%) samples. The GA genotype was detected in 51 (87.93%) (RA) patients and 17 (85%) in the HC. In contrast, the AA genotype was undetected in any patient or control. The G (size=180bp) and A allele (size=245bp), along with the internal control (size=370bp), were visualized in 2% agarose gel, as shown in Fig. 1.
 Electrophoresis of Cdx2 rs11568820 vitamin D3 receptor gene polymorphism by (Tetra-primer ARMS–PCR) on 2% agarose gel. The size of the G allele=180bp, the A allele=245bp, and the internal control=370bp.")
No significant association was found between the Cdx2 VDR rs11568820 analysis by tetra primer ARMS-PCR (G/A) polymorphism and the risk of developing RA in the present study, with the probability of p<0.05. Two DNA samples did not yield readable results during electrophoresis. The odd ratio, 95% CI intervals, and p-value are presented in Table 5.
Statistical analyses of VD Cdx2 rs11568820 genotype in RA patients and HC.
| Genotypes | RA n=58 (%) | HC n=20 (%) | Odd ratio (OR) | 95% CI | p-Value |
|---|---|---|---|---|---|
| GG | 7 (12.07) | 3 (15) | 1 | 0.14–6.77 | 1 |
| GA | 51(87.93) | 17 (85) | 0.77 | 0.18–3.34 | 0.73 |
| AA | 0 (0) | 0 (0) | – | – | – |
| G allele | 65 (76.5) | 20 (23.5) | 1 | 0.49–2.03 | 1 |
| A allele | 51 (75) | 17 (25) | 1.08 | 0.51–2.2 | 0.83 |
In terms of serum VD3 level based on Cdx2 genotypes, both the HC and RA groups (GA genotype), the outcomes of the present study revealed that 17 women in the HC group and 51 women with RA possessed the GA genotype. Additionally, as presented in Fig. 2, the current results showed a significant decrease in serum VD3 levels in the RA group with the GA genotype compared to the HC group with a similar genotype (p=0.0002). The mean and standard error for the RA and HC groups were (18.89±1.563SE and 28.30±1.960SEng/ml), respectively.

Fig. 3 illustrates the results of the GG genotype and serum VD3 levels, which revealed a non-significant decrease in serum VD3 levels in RA patients with the genotype GG compared to HC of a similar genotype (24.91±4.48SE and 31.92±6.82SEng/ml, p=0.4833).

When we compared serum VD3 levels according to GA and GG genotypes, the present results revealed that RA patients with heterozygote GA genotype for Cdx2 had a relatively lower mean for serum VD3 level than those with homozygotes GG genotype. The means for RA patients were 18.89 and 24.91 for both GA and GG genotypes, respectively, as shown in Fig. 4. The current findings displayed that the level of serum IL-17 was significantly (p<0.0003) increased in RA with GA genotype compared to HC with a similar genotype (108.5±5.731) and 61.56±3.768ng/ml) respectively, as in Fig. 5. Whereas there was a non-significant difference (p=0.1833) in the level of serum IL-17 in RA with GA genotype compared to HC of the same genotype (98.23±16.28 and 65.57±9.476ng/ml), respectively, as illustrated in Fig. 6.



According to genotypes of Cdx2 VDR polymorphism, the current data showed serum levels of VD3, IL-17, and anti-CCP in RA patients. Serum VD3 levels in women with RA who had the heterozygote GA genotype for Cdx2 were found to be, on average, lower than those in homozygotes (p=0.1098). The mean serum anti-CCP levels were higher in homozygotes compared to heterozygotes. However, the difference in VD3 levels between GA and GG genotypes was not statistically significant. Also, GA and GG genotypes did not differ significantly (p=0.3261) in their levels of IL-17. Similarly, the difference in anti-CCP levels between GA and GG genotypes was not statistically significant (p=0.5121), as shown in Table 5.
Our results for assessing DNA quality indicated that the purity of the extracted DNA fell within the acceptable range of good quality. According to an earlier publication, the typical 260/280 ratios for DNA and RNA generated by pure nucleic acids are 1.8 and 2.0, respectively. This ratio is affected by the buffer's pH, and ionic potency was used to measure the blank and the sample [21]. Furthermore, Surzycki concluded that DNA samples with an OD260/OD280 ratio between 1.6 and 2 were considered pure, while samples above or below this range were deemed protein or RNA contamination, respectively (Table 6) [22].
The mean (± SE) values of VD3, IL-17, and Anti-CCP across the different Cdx2 rs11568820 VDR polymorphism genotypes in women with RA.
| Cdx2 VDR polymorphism | Serum VD3 level (ng/ml) | Serum IL-17 level (pg/ml) | Serum anti-CCP level (U/ml) |
|---|---|---|---|
| GA genotype | 18.89±1.563 | 108.5±5.731 | 67.40±14.55 |
| GG genotype | 24.91±4.484 | 98.23±16.28 | 123.1±57.50 |
| p value | 0.1098 | 0.3261 | 0.5121 |
One immunomodulatory agent that shows promise is vitamin D. Vitamin D is known for its immune-stimulating properties, as it enhances the performance of the innate immune system and may contribute to immune tolerance. Vitamin D deficiency has been linked to autoimmune diseases [23,24].
The VDR is abundantly present in immune system cells such as dendritic cells, macrophages, and activated T and B lymphocytes. This distribution suggests that VD's regulatory role in the immune system operates through multiple mechanisms. Additionally, vitamin D inhibits proinflammatory processes by binding to VDR and preventing immune cells from becoming overly active during an adaptive autoimmune response. It seems to regulate immune homeostasis by enhancing innate immunity while suppressing adaptive immunity. Moreover, VD can alter the ratio of Th1 to Th2 and T regulatory cells [25,26].
The last few decades have witnessed increased speculation about the potential role of hypovitaminosis D as a risk factor for multiple sclerosis (MS), based on research findings linking MS and VD status. There is a connection between MS susceptibility and specific gene variants that encode proteins involved in VD metabolism, transport, and function [27]. VD3 inhibits the proliferation of cancer cells by binding to its nuclear receptors leading to apoptosis. As the VDR gene lacks consensus TATA and CAAT boxes, the VDR-Cdx2 polymorphism, found in the promoter region of exon 1e, affects the functional activity of the receptor [26]. The same author and his colleagues also studied the link between VDR-Cdx2 polymorphism and breast cancer in premenopausal Pakistani women. They hypothesized that young female patients with the GG genotype of the Cdx2-VDR gene polymorphism might have a raised risk for breast cancer. Although breast cancer and the VDR Cdx2 polymorphism were not significantly associated, women with the GG genotype were at an increased risk of breast cancer [28].
Due to its anti-inflammatory properties, VD helps prevent the onset of arthritis. The biologically active form of vitamin D, 1,25(OH)2D3, can exert its effect only after binding to its specific VD receptor, encoded by the VDR gene. Several human autoimmune diseases, mostly TH1- or TH17-intermediated, such as RA, have been linked to the pathogenic impact of TH17 lymphocytes [29,30].
Our result showed that the most common Cdx2 genotype in the Kurdish population of Iraq was GA, followed by the GG genotype. Additionally, no AA genotype was detected. Moreover, no significant associations were found among the genotypes; thus, the Cdx2 hasn’t influenced the risk of RA susceptibility among the Kurdish population. A study among the Turkish people investigated, VDR BsmI, TaqI and FokI gene polymorphisms, concluding that in the Turkish population, VDR polymorphism does not affect rheumatoid factor positivity, susceptibility to RA, or erosive disease of RA [31]. It is well-known that G>A sequence variation in the 1a promoter region, known as the Cdx2 polymorphism, is linked to the transcriptional activity of the VDR gene [32]. In 2020, Saleh recorded in Iraq that the genotypes and alleles that were more associated with RA were ApaI (TT) and the T allele, TaqI (CC) and the T allele, BsmI (GG) and the A allele, and FokI (TT) and the C allele. In contrast, this study didn’t include the CDx2 [33].
The association between VDR gene polymorphism and the risk of RA has been assessed, reporting conflicting results [15]. In the same aspect, a recent investigation indicated that several genetic loci contribute to the increased risk of RA in the British White sample. The polygenic risk score (PRS) is significantly higher in those with RA and can be used for clinical applications and personalized disease prevention [34]. In their research on susceptibility to RA, Marquez Pete et al. found that the VDR FokI gene polymorphism suggested a potential increased risk for developing RA. Conversely, they observed no effect from the VDR BsmI, TaqI, ApaI, and Cdx2 polymorphisms on RA risk. Nevertheless, haplotype analysis revealed that the haplotypes ACGAG and GTGCA were linked to a greater risk of RA [35]. Another study has suggested that polymorphism is closely associated with an increased risk of RA, particularly the polymorphisms in Tumor necrosis factor receptor-associated factor 1-complement 5 (TRAF1-C5). This polymorphism causes a change in the amino acid within TRAF1. As a result, it boosts the TNF-α signaling, which leads to an increase in pro-inflammatory response [36].
The GG genotype of Cdx2-VDR gene polymorphism may increase the risk of developing breast cancer in young female patients in South Pakistan [28].
Additionally, Pinho et al [37]. investigated the distribution of VDR gene polymorphism in people with type 2 diabetes mellitus (DM2) and chronic periodontitis (CP), including FOKI, CDX2, and GATA. According to the findings, having these variants may result in less susceptibility to DM2 and CP. No significant differences between groups were found in the analysis of other SNPs.
A study conducted on the relation of Cdx2 VDR gene polymorphism with susceptibility to autoimmune thyroiditis in the Caucasian Polish population revealed that the Cdx2 VDR gene does not play a significant role in the development of autoimmune thyroiditis [38]. A recent study indicated that RA patients frequently have VD deficiency, and their 25(OH)D levels are significantly lower than those of HC. Higher disease activity and disability scores were associated with lower VD levels. Four VDR polymorphisms identified through genetic analysis did not increase the susceptibility to RA in the Lithuanian population [14].
Various vitamin D-related gene polymorphisms, including those in the VDR, may increase the risk of developing autoimmune diseases. To investigate the relationship between the VDR Cdx2 (rs11568820) polymorphism and autoimmune thyroid disease (AITD) in the Caucasian-Polish population, genotyping of the CDX2 polymorphism was carried out. There is no statistically significant difference between the genotype or allele distribution of the VDR Cdx2 polymorphism in the Caucasian-Polish population between AITD, AIT, or TAO, and the control group [30]. However, Maciejewsk et al [39]. investigated that TAO patients’ VDR Cdx2 genotype distribution was significantly different from that of the AIT group.
Except for Cdx2, the VDR genetic variants were linked to the severity of Polycystic Ovary Syndrome (PCOS) symptoms but not the disease itself. These variants are not directly associated with PCOS risk factors or causes.; however, they could indirectly affect the development of PCOS at the biochemical level by regulating calcium or VD levels [30]. In this aspect, a study was performed in Iraq regarding the genotypic frequencies distribution of Cdx2 polymorphism of the VDR gene between women with PCOS and controls. They concluded that the odds ratio for GG carriers was 1.93, for AA carriers it was 0.95, while for GA carriers it was 0.52 [40].
Additionally, Ling et al. [41] showed that the serum 25(OH)D levels of Chinese women and the risk of osteoporosis and fracture in middle-aged and elderly individuals might be impacted by the Cdx-2 polymorphism in the VDR gene and compared to GG genotype carriers, carriers of the AA and AG genotypes had higher odds of fracture. This study also found that women who were GG carriers had the highest 25(OH)D levels, AA carriers had the lowest, and AG carriers fell in the middle.
A subsequent study by Rehman et al. [42] on cancer patients found a significant association between the SNP of the VDR-Cdx2 gene polymorphism and the development of several diseases. According to the study's results, there is a strong link between the genotypes AG (32%), and GG (66.8%), and several cancer types, including multiple myeloma (MM), rectal cancer, colon cancer, and gastric cancer (GC) (P 0.05). The genotype AA (1.2%) was less standard in this study.
In a research study involving Pakistani patients with RA and osteoarthritis (OA), it was observed that serum vitamin D levels were not significantly low in the study groups. Still, that polymorphism on the VDR gene limits vitamin D's ability to act as an anti-inflammatory by changing the 1, 25(OH)2 D3 binding sites. As a result, 25(OH)2D3 dysfunction ultimately causes disease onset. They showed a significant correlation between the beginning of RA and OA in the population under study and the VDR gene polymorphisms (rs10735810, rs7975232, rs731236, and rs1544410). They proved that tryptophan is replaced with arginine when there is a polymorphism on rs10735810. Vitamin D could not convert into the active form and prevent disease onset because of polymorphism in the VDR gene. Consequently, in the Pakistani population, VDR gene polymorphism is a significant risk factor for the development of RA and OA [27].
Polymorphisms in the VDR are linked to many diseases, potentially impacting mortality. A prospective cohort study established a connection between the VDR gene polymorphisms (FokI, three haplotypes of the Cdx2 and GATA polymorphisms, and three haplotypes of the BsmI, ApaI, and TaqI polymorphisms) and mortality in older people. They found that osteoporotic fractures may contribute to the increased mortality risk associated with the Cdx2-GATA haplotype 1 allele [43]. In contrast, a separate genomic study identified that the HLA-DRB1*04 genotype was associated with RA susceptibility in most Iraqi patients, indicating that the HLA-DRB1*04 allele significantly contributed to the onset of RA [44]. Various vitamin D-related gene polymorphisms, including those in the VDR gene, may elevate the risk of emerging autoimmune diseases. Among RA patients, 41.7% suffered from co-existing autoimmune and non-autoimmune diseases, such as type 1 and 2 diabetes mellitus, hypothyroidism, asthma, psoriasis, and allergy. This result suggests RA patients’ vulnerability and may indicate a connection between RA and other autoimmune diseases [45], and 78.3% of women have a family history of RA disorder [46].
ConclusionBased on our experimental findings, the following conclusion can be drawn. This study represents the first attempt to detect Cdx2 vitamin D receptor genotyping of RA patients in Iraq by Tetra-primer ARMS PCR technique with specifically designed primers. Our study successfully developed the tetra-primer ARMS PCR protocol for Cdx2 genotyping. The genotypes and alleles more associated with RA were Cdx2 (GA), with the GG genotype detected in 12.07% of RA samples, and in HC groups, the GG genotype was found in 15%. The GA genotype was found in 87.93% of RA patients and 85% of HC. Despite non-significant values, the current work found that 51 RA patients have the GA genotype of the Cdx2 polymorphism. Although the current findings showed no significant association between Cdx2 gene polymorphisms and the risk of RA, this genotype still represents the most common or dominant among the study's RA patients.
Author's contributionBS and MA designed the study. RQ performed the research method. RQ and BS analyzed the data. BS and MA wrote the paper. All authors discussed the results and contributed to the final manuscript.
Consent for publicationWe hereby consent to the publication of identifiable details in the journal mentioned above.
Ethics approval and consent to participateThis study was conducted under the Helsinki agreement and received ethical approval from Soran University Hospital, referenced 1/1/178, on November 15,2021. Before participation, patients were informed about the study, and all participants voluntarily signed consent forms. To ensure confidentiality, no personal names or identities were disclosed in this study; all participants were referenced using anonymous numbers.
FundingThe authors received no specific funding for this manuscript.
Conflicts of interestThe authors have no conflict of interest to declare.
Data availabilityNot applicable.
Code availabilityNot applicable.
The authors thank SiSaf drug delivery nanotechnology and Soran University for cooperating.
