






To determine the prevalence and polygraphic and clinical characteristics of patients with postural sleep apnea attended on a Colombian health institute at Bogotá, Colombia.
MethodsProspective descriptive observational study of patients older than 18 years old who underwent a polygraphic study because of a suspected OSA during a 6-month period between 2022 and 2023.
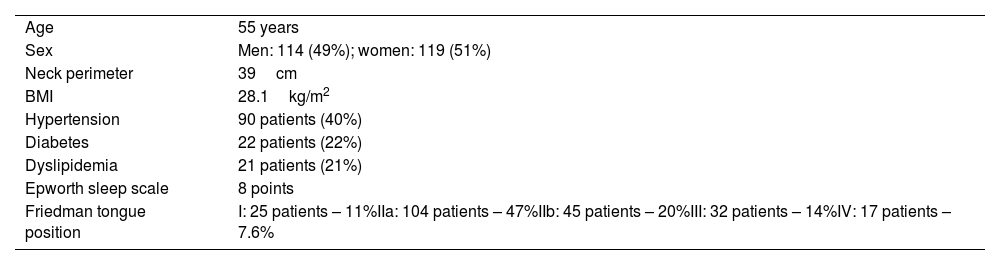
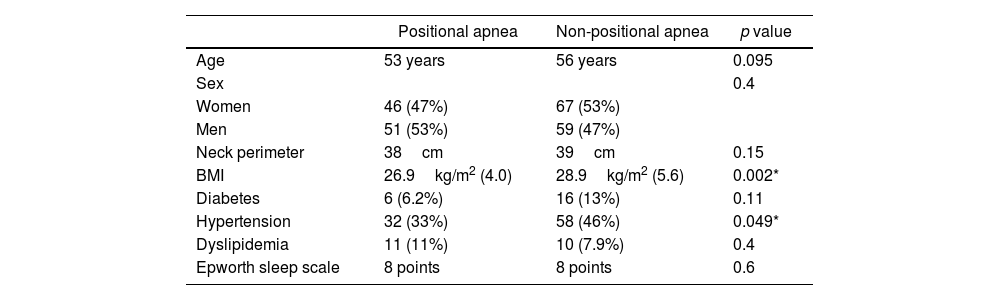
ResultsA total of 233 polygraphic recordings were done in different patients who met criteria for the study. Ninety-seven patients (43%) met criteria for positional apnea and 126 (57%) for non-positional apnea. Patients with postural apnea had lower AHI (p<0.001), lower body mass index (p=0.002) and less hypertension (p=0.002). NADIR was lower in patients with non-positional apnea, 75% vs 72% (p=0.039). No significant statistical differences were found when comparing groups by age, sex or by Epworth, STOP-BANG, FOSQ-10, or Friedman's tongue position scales.
ConclusionsPostural apnea is a prevalent condition in Colombian population. According to our results these patients tend to have a lower severity of sleep apnea measured by AHI, lower BMI and less high blood pressure.
Determinar la prevalencia y las características clínicas y poligráficas de pacientes con apnea postural atendidos en una institución de salud en Bogotá, Colombia.
MetodologíaEstudio observacional descriptivo prospectivo de pacientes mayores de 18 años a quienes se les realizó una poligrafía respiratoria por sospecha de apnea obstructiva del sueño en un periodo de 6 meses entre el 2022 y 2023.
ResultadosUn total de 255 estudios poligráficos fueron realizados en pacientes diferentes; 97 pacientes (43%) cumplieron criterios para apnea postural y 126 (57%) para apnea no postural. Los pacientes con apnea postural tuvieron niveles de IAH más bajos (p<0,001), menor índice de masa corporal (p=0,002) y menor historia de hipertensión arterial (p=0,049). La saturación mínima registrada durante el estudio fue más baja en pacientes con apnea no postural, 72% vs. 75% (p=0,039). No hubo diferencias estadísticamente significativas entre los dos grupos al compararlos por edad, sexo ni al comparar las puntuaciones en las escalas de Epworth, STOP-BANG, FOSQ-10 o Friedman.
ConclusionesLa apnea postural es una condición prevalente en la población colombiana. De acuerdo a nuestros resultados, estos pacientes tienden a tener menor severidad de la apnea, menor índice de masa corporal y menor historia de hipertensión arterial.

