


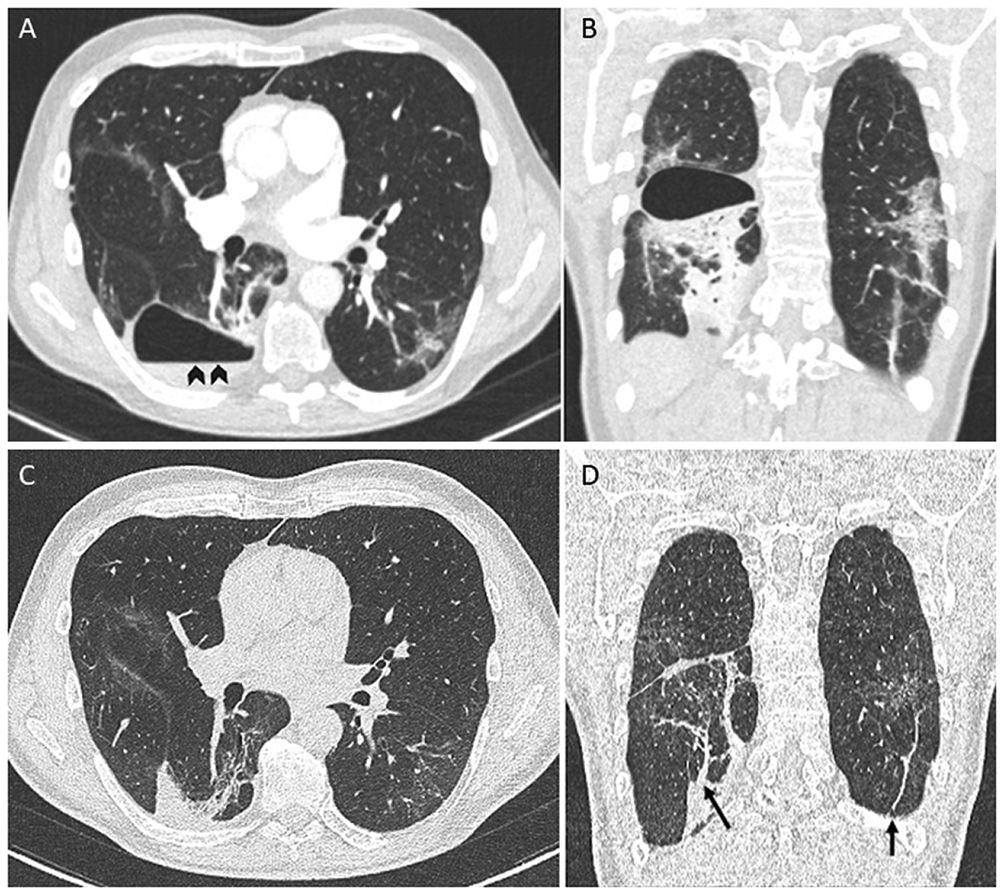
A 61-year-old man with no significant medical history presented to the emergency department with worsening dyspnea a week after close contact with someone who had COVID-19. He was unvaccinated. He was hypoxemic, and the chest radiograph showed bilateral opacities consistent with COVID-19 pneumonia and tested positive for RNA from SARS-CoV-2. Blood tests showed raised inflammatory markers. Computed tomography (CT) of the chest demonstrated bilateral ground-glass opacities. The patient was hospitalized and treated with high-flow nasal oxygen therapy, dexamethasone, and sarilumab. His clinical status improved, and he was discharged home after 1 week of hospitalization. Three weeks later, he presented again with worsening dyspnea, fever, and pleuritic chest pain. A CT pulmonary angiography ruled out pulmonary embolism (Fig. 1A, B) but demonstrated a thin-walled cystic lesion with an air–fluid level (Fig. 1A, arrowheads) that suggested an infected pneumatocele. The patient was managed conservatively with amoxicillin/clavulanic acid for 3 weeks. During the follow-up, the patient reported the disappearance of symptomatology. A subsequent CT performed 8 weeks after the diagnosis showed complete resolution of the pneumatocele (Fig. 1C, D) with persisting subpleural and parenchymal bands (Fig. 1D, arrows).
 (A) and consolidations in lower lobes (B). Chest Angio-CT performed eight weeks later showed complete resolution of the pneumatocele (C) with persisting subpleural and parenchymal bands (arrows) (D).")
None.
Potential conflicts of interestJ.P. has been a consultant for Pfizer, MSD, Gilead, and Novartis. Other authors: No reported conflicts.
None
