






The increase in the incidence of hip fractures in elderly patients is associated with higher mortality, with rates as high as 30% per year. The aim of this study was to identify the factors associated with in-hospital and 12-month mortality in patients undergoing hip arthroplasty for femoral neck fracture. While the type of procedure (HA vs. THA) was analysed, the primary focus was on clinical and perioperative variables influencing mortality.
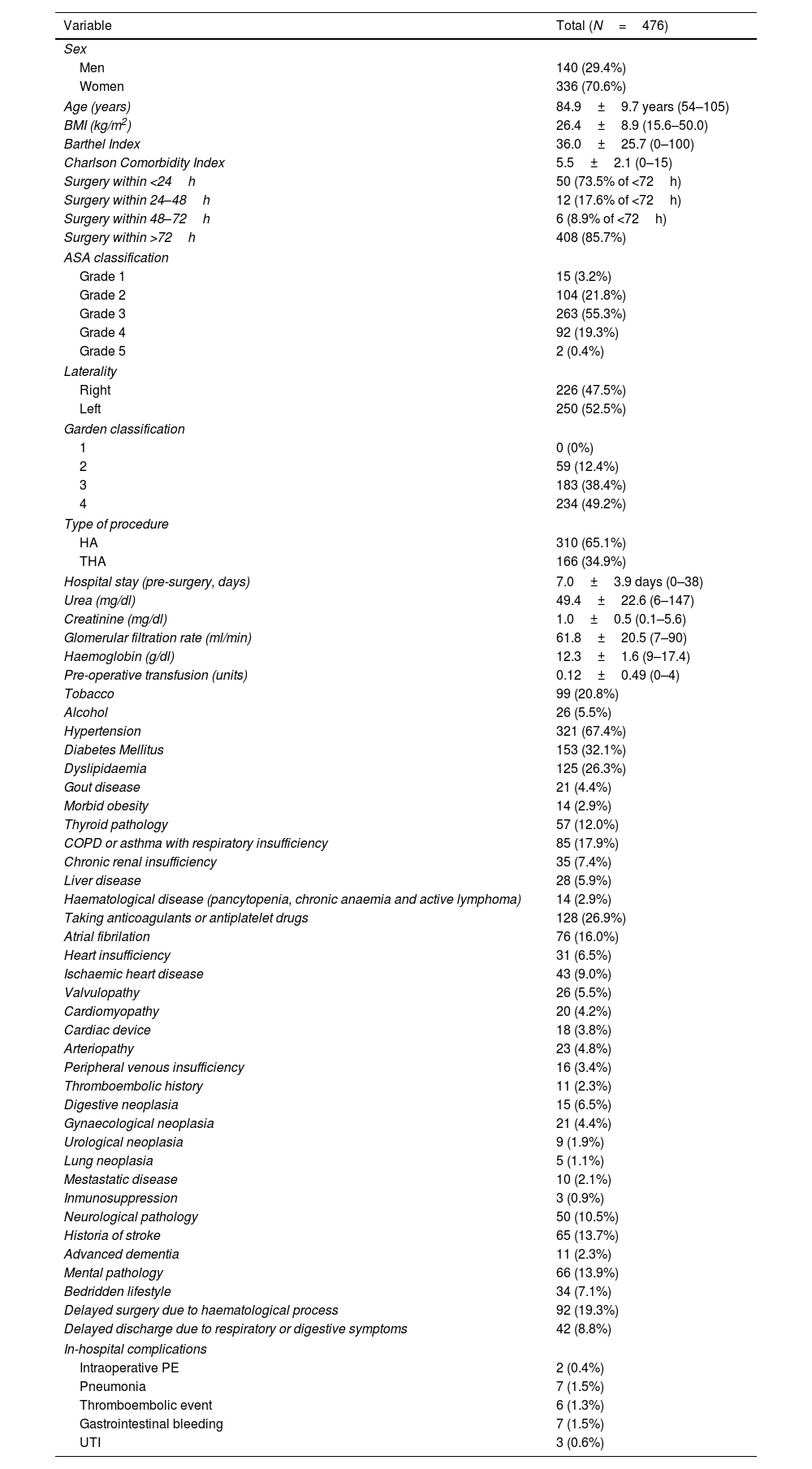
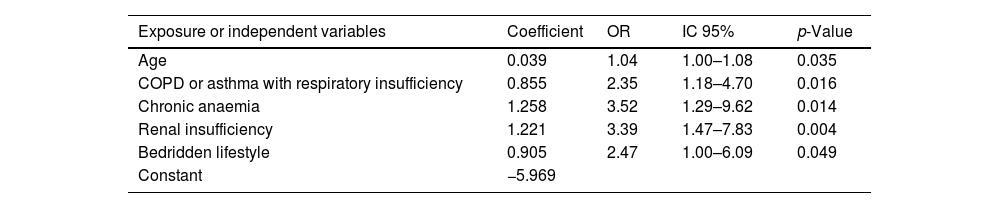
Material and methodsA retrospective case–control study was conducted with a sample of 476 patients treated with THA or HA between 2016 and 2018. A multivariate analysis was performed, to identify the variables with the most significant impact on in-hospital mortality and mortality within the first year of follow-up.
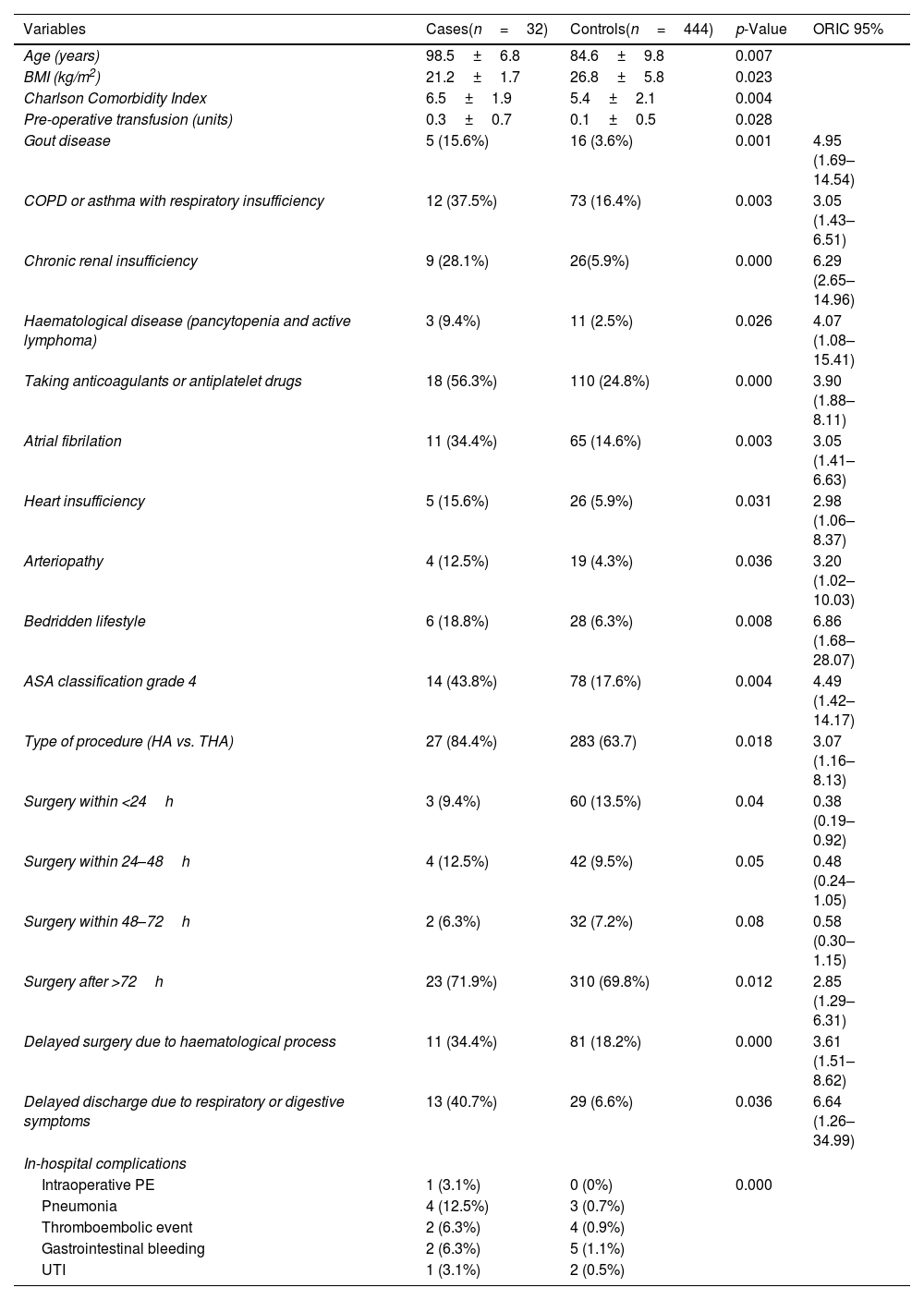
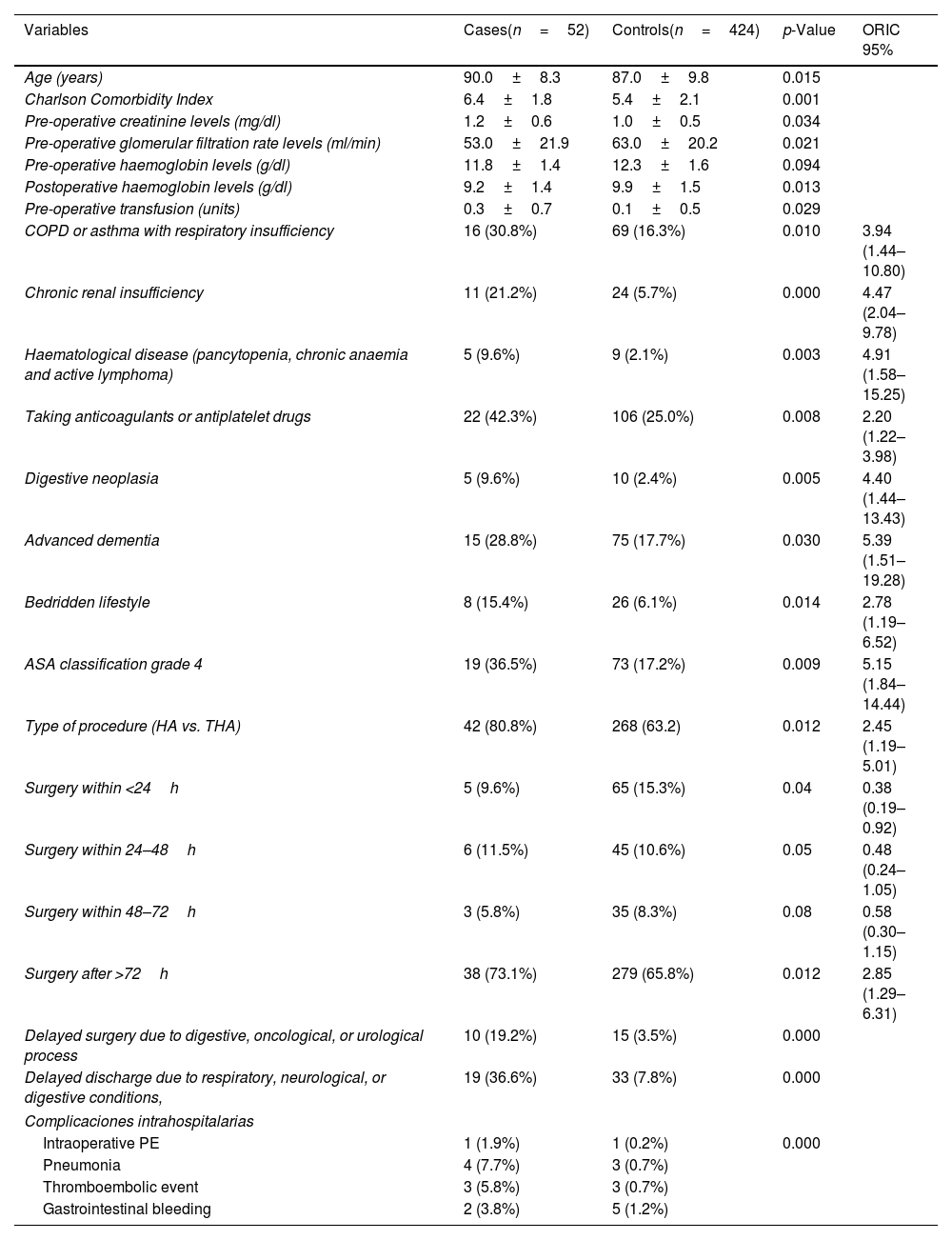
ResultsIn-hospital mortality was 6.8%, while 12-month mortality reached 10.9%. The variables associated with higher mortality were age, respiratory disease, renal insufficiency, chronic anaemia, use of antiplatelet or anticoagulant medications, and being bedridden or chair-bound. No statistically significant differences were observed regarding the type of procedure (THA or HA).
ConclusionsThe use of antiplatelet or anticoagulant medications, chronic renal insufficiency, and being bedridden or chair-bound were associated with higher in-hospital mortality. Chronic anaemia, respiratory disease, chronic renal insufficiency, and being bedridden or chair-bound correlated with an increase in mortality during the first year.
El aumento en la incidencia de fracturas de cadera en pacientes ancianos se asocia a una mayor mortalidad, con tasas que pueden alcanzar hasta el 30% anual. El objetivo de este estudio fue identificar los factores asociados con la mortalidad intrahospitalaria y a 12 meses en pacientes que reciben artroplastia de cadera por fractura de cuello femoral. Aunque se analizó el tipo de procedimiento (HA vs. ATC), el enfoque principal se centró en las variables clínicas y perioperatorias que influyen en la mortalidad.
Material y métodosSe realizó un estudio retrospectivo de casos y controles con una muestra de 476 pacientes tratados con ATC o HA entre 2016 y 2018. Se llevó a cabo un análisis multivariante, para identificar las variables con mayor influencia en la mortalidad intrahospitalaria y en la mortalidad dentro del primer año de seguimiento.
ResultadosLa mortalidad intrahospitalaria fue del 6,8%, mientras que a los 12 meses alcanzó el 10,9%. Las variables que se asociaron con mayor mortalidad fueron la edad, la enfermedad respiratoria, la insuficiencia renal, la anemia crónica, la toma de antiagregantes o anticoagulantes y la vida cama-sillón. No se apreciaron diferencias estadísticamente significativas en relación con el tipo de procedimiento (ATC o HA).
ConclusionesLa toma de antiagregantes o anticoagulantes, la insuficiencia renal crónica y la vida cama-sillón se asociaron con una mayor mortalidad intrahospitalaria. La anemia crónica, la enfermedad respiratoria, la insuficiencia renal crónica y la vida cama-sillón se correlacionaron con un aumento en la mortalidad durante el primer año.

