





To characterize meningococcal strains isolated from five cases of meningococcal disease (MD) associated with an outbreak in Trancoso – BA, occurred in October 2009. All cases, with the exception of a 39-year-old male, attended a dance party with approximately 1000 youngsters in a rural site.
Materials and methodsThe epidemiological investigation was conducted by the Epidemiological Surveillance Service of Bahia State. Meningococcal strains were characterized at Adolfo Lutz Institute, the Brazilian National Reference Laboratory for Bacterial Meningitis by conventional techniques (serotype, serosubtype and antimicrobial susceptibility test) and by molecular methods (Pulsed-field gel electrophoresis – PFGE and Multilocus Sequence Typing – MLST).
ResultsThe PFGE showed 2 closely related restriction profiles, designated as PFGE types A and A1, having 92% relatedness to each other. MLST characterization showed both A and A1 clones were ST-3780, which belongs to the ST-103 complex. All isolates displayed the phenotype C:23:P1.5 and were susceptible to all antibiotics tested.
ConclusionsThis is the first reported MD outbreak associated with serogroup C ST-103 complex in Brazil, as well as the party and illicit drug-use associated outbreak.
Caracterizar las cepas de Neisseria meningitidis (Nm) aisladas de cinco pacientes con Enfermedad Meningocócica (EM) asociada a un brote epidémico en Trancoso - BA, que ocurrió en octubre del 2009, luego de una fiesta en zona rural y en la que participaron 1000 jóvenes .Todos los casos fueron secundarios al caso primario a excepción de un paciente varón de 39 años.
Materiales y métodosEl Servicio de Vigilancia Epidemiológica del Estado de Bahia realizó la investigación epidemiológica y las cepas de Nm se caracterizaron en el Laboratorio Nacional de Referencia para Meningitis, Instituto Adolfo Lutz - São Paulo mediante métodos convencionales (sero - subtipificación y prueba de sensibilidad a los antimicrobianos) y métodos moleculares (electroforesis en gel de campo pulsado- PFGE y Multilocus Sequence Typing - MLST).
ResultadosLa PFGE mostró dos perfiles de restricción estrechamente relacionados designados como PFGE tipos A y A1 con 92% de relación entre sí. Ambos tipos fueron clasificados como ST-3780 mediante MLST, y pertenecientes al complejo clonal ST-103. Todos los aislados mostraron el fenotipo C: 23: P1.5 y eran susceptibles a todos los antibióticos testados.
ConclusionesEste es el primer brote de EM reportado asociado a cepas de Nm serogrupo C del complejo clonal ST-103 y relacionado con el consumo de drogas en Brasil.
Meningococcal disease (MD) remains a major worldwide health problem, with most disease globally being caused by serogroups A, B, C, W135 and Y.1 In recent years, MD in Brazil has been caused primarily by serogroup B and C strains. During the past decade, the proportion of cases caused by serogroup B strains declined from 74.5% in 2000 to 25.7% in 2008, corresponding to a decline from 0.6 to 0.1 per 100,000 inhabitants in the average annual incidence of serogroup B MD. At the same time, serogroup C MD has been steadily increasing in several Brazilian states, from 22.4% to 67.7%. The annual incidence of serogroup C MD increased from 0.2 cases in 2000 to 0.41 cases per 100,000 habitants in 2008.2N. meningitidis serogroup C:23:P1.14-6, belonging to the ST-103 complex, was first described in São Paulo State in 19893 and by 2009 accounted for 75.4% of MD cases. In addition, since 2004 serogroup C ST-103 complex strains have also emerged as the main cause of MD outbreaks in Brazil.
In October 2009, the local authorities of Porto Seguro, a coastal town in Bahia State reported a cluster of meningococcal serogroup C cases associated with a party (http://www.saude.ba.gov.br/arquivos/Nota%20Meningite%20em%20Porto%20Seguro%20(04-11-2009.pdf). To further investigate the outbreak, we characterized the outbreak-associated isolates using molecular methods such as pulsed-field gel electrophoresis (PFGE) and multilocus sequence typing (MLST).
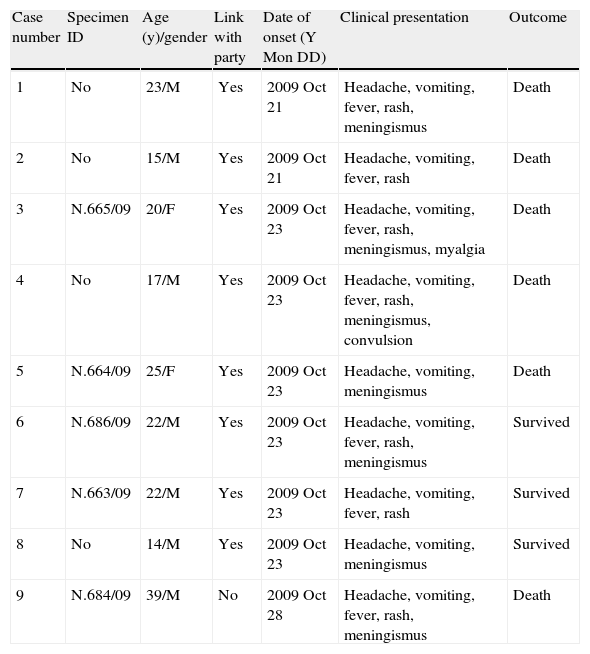
Material and methodsEpidemiological data and bacterial isolatesThe epidemiological investigation was conducted by the Epidemiological Surveillance Service of Bahia, State and the data are presented in Table 1. Nine cases, 6 (67%) of which were fatal, were reported to public health authorities in Porto Seguro, Bahia between October 21 and 26, 2009. The outbreak occurred in Trancoso, a small coastal town of 4538 inhabitants. There were 7 male and 2 female patients, and all were between the ages of 14 and 39 years. All cases, with the exception of a 39-year-old male, attended a dance party with approximately 1000 youngsters on October 18 in a rural site in Trancoso. Alcohol consumption, cigarette smoking and illicit drug use were reported during the outbreak investigation. People who had close contact with patients, such as a family and classroom colleagues received rifampin chemoprophylaxis. The MD cases were laboratory confirmed, either by isolation of N. meningitidis serogroup C in blood or cerebrospinal fluid (5/9, 55.5%), or by the detection of serogroup C meningococcal polysaccharide in cerebrospinal fluid by latex agglutination (4/9; 44.5%). All meningococcal isolates were confirmed and serogrouped at Adolfo Lutz Institute, the Brazilian National Reference Laboratory for Bacterial Meningitis, using conventional microbiologic methods.4–6
Summary of cases, meningococcal disease outbreak, Trancoso, Brazil.
| Case number | Specimen ID | Age (y)/gender | Link with party | Date of onset (Y Mon DD) | Clinical presentation | Outcome |
| 1 | No | 23/M | Yes | 2009 Oct 21 | Headache, vomiting, fever, rash, meningismus | Death |
| 2 | No | 15/M | Yes | 2009 Oct 21 | Headache, vomiting, fever, rash | Death |
| 3 | N.665/09 | 20/F | Yes | 2009 Oct 23 | Headache, vomiting, fever, rash, meningismus, myalgia | Death |
| 4 | No | 17/M | Yes | 2009 Oct 23 | Headache, vomiting, fever, rash, meningismus, convulsion | Death |
| 5 | N.664/09 | 25/F | Yes | 2009 Oct 23 | Headache, vomiting, meningismus | Death |
| 6 | N.686/09 | 22/M | Yes | 2009 Oct 23 | Headache, vomiting, fever, rash, meningismus | Survived |
| 7 | N.663/09 | 22/M | Yes | 2009 Oct 23 | Headache, vomiting, fever, rash | Survived |
| 8 | No | 14/M | Yes | 2009 Oct 23 | Headache, vomiting, meningismus | Survived |
| 9 | N.684/09 | 39/M | No | 2009 Oct 28 | Headache, vomiting, fever, rash, meningismus | Death |
ID, identification.
For PFGE, genomic DNA was prepared in agarose plugs and digested with the restriction enzyme Nhe I7 and DNA digested were separated by electrophoresis in agarose 1% w/v gels as described by Popovic et al.7 and restriction profiles were analyzed according to the criteria of Tenover et al.8 and using Bionumerics (Applied Maths, St-Martens-Latem, Belgium). The isolates showing similarity >85% were considered to be closely related.
Serological typingSerotyping and serosubtyping were performed by dot blotting using whole cell suspensions as previously described9 using a panel of 18 PorB and 15 PorA murine MAbs specific for the variable regions, respectively.3
Multilocus sequence typing (MLST)MLST was performed according to the methods of Maiden et al.10 Primers, determination of a sequence alleles, and designation of sequence types are described on the MLST website (http://neisseria.org/nm/typing/mlst).
Antimicrobial susceptibility testingIsolates were tested for susceptibility to penicillin, ampicillin, ceftriaxone, ciprofloxacin, chloramphenicol and rifampin using the broth microdilution procedure established by the Clinical and Laboratory Standards Institute (CLSI).11 The susceptibility/resistance breakpoints were those recommended by the European Monitoring Group on Meningococci.12
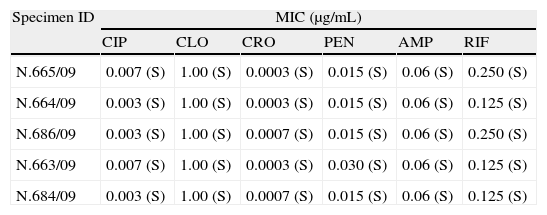
ResultsBased on the 9 cases, the MD incidence was 198 per 100,000 Trancoso inhabitants and, considering the 8 party-associated cases separately, the incidence among party participants was 800 per 100,000. Among the 5 N. meningitidis isolates, there were 2 closely related restriction profiles: one (4 isolates) was designated PFGE type A and was considered to be the outbreak strain, and the remaining isolate was designated as PFGE type A1; PFGE types A and A1 had 92% relatedness to each other (Fig. 1). Both types were shown by MLST to be ST-3780, which belongs to the ST-103 complex. All the isolates displayed the phenotype C:23:P1.5. All strains were susceptible to all antibiotics tested (Table 2).

Susceptibility to six different antimicrobials of Neisseria meningitidis strains isolated from Porto Seguro – Bahia cases.
| Specimen ID | MIC (μg/mL) | |||||
| CIP | CLO | CRO | PEN | AMP | RIF | |
| N.665/09 | 0.007 (S) | 1.00 (S) | 0.0003 (S) | 0.015 (S) | 0.06 (S) | 0.250 (S) |
| N.664/09 | 0.003 (S) | 1.00 (S) | 0.0003 (S) | 0.015 (S) | 0.06 (S) | 0.125 (S) |
| N.686/09 | 0.003 (S) | 1.00 (S) | 0.0007 (S) | 0.015 (S) | 0.06 (S) | 0.250 (S) |
| N.663/09 | 0.007 (S) | 1.00 (S) | 0.0003 (S) | 0.030 (S) | 0.06 (S) | 0.125 (S) |
| N.684/09 | 0.003 (S) | 1.00 (S) | 0.0007 (S) | 0.015 (S) | 0.06 (S) | 0.125 (S) |
MIC breakpoints to CIP: Susceptible, ≤0.03μg/mL; Resistant, ≥0.5μg/mL; CLO: Susceptible, ≤2μg/mL; Resistant, ≥8.0μg/mL; CRO: Susceptible, ≤0.12μg/mL; PEN: Susceptible, ≤0.06μg/mL; Resistant, ≥1.0; AMP: Susceptible, ≤0.12μg/mL; Resistant, ≥2.0μg/mL; RIF: Susceptible, ≤0.25μg/mL; Resistant, ≥2.0μg/mL.
MIC, minimum inhibitory concentration; CIP, ciprofloxacin; CLO, choramphenicol; CRO, ceftriaxone; PEN, penicillin; AMP, ampicillin; RIF, rifampicin; (S), susceptible.
N. meningitidis serogroup C strains isolated from areas where the disease is endemic, or from outbreaks, have usually belonged to the ST-11 or ST-8 complex.13N. meningitidis serogroup C isolates belonging to the ST-11 complex have been responsible for numerous epidemics and outbreaks in the United States, Canada, and Europe, since the early 1990s. These hyperinvasive strains have predominantly affected adolescents and young adults, and have required frequent, massive public health investigations and interventions.14,15 In contrast, most serogroup C sporadic disease and outbreaks in Brazil since 2000 have been caused by strains belonging to the ST-103 complex,3 which differs from ST-11 at all 7 MLST loci, indicating that they are highly unrelated to each other (www.pubmlst.org). This is in contrast to ST-8 N. meningitidis which caused substantial serogroup C disease in Brazil during in the 1990s.3 ST-8 has been previously shown by whole genome sequencing to be closely related to ST-11, with which it shares 3 MLST loci16 (www.pubmlst.org).
The origin of the ST-103 complex is unknown. In addition, the impact of serogroup C conjugate vaccine, which was introduced into the routine childhood immunization schedule in 2010, on pharyngeal carriage caused by ST-103 strains is also not known. Efforts are needed to continue to monitor its spread and define its virulence in order to understand the evolution of this clone in Brazil.
The ST-103 complex, with most strains displaying the 23:P1.14-6 phenotype,3 have been present in Brazil since 1989 and were associated with the serogroup C epidemic in the 2000. Although ST-103 is relatively uncommon globally as a cause invasive disease, it has recently been reported in Poland (phenotype C:NT:P1.3,6).17
Although most of the N. meningitidis serogroup C, ST-103 complex strains isolated in Brazil have displayed the 23:P1.14-6 phenotype, in the present outbreak, all of the tested strains displayed the 23:P1.5 phenotype. This change in antigenic profile likely occurred through horizontal gene transfer and would have contributed to both the generation and the spread of novel antigenic variants of the protein.18 Antigenic shift within ST-11 serogroup C strains in association with increase in MD incidence has been described in the United States.19
PFGE has been successfully applied to determine the relatedness of bacterial isolates suspected of being part of an outbreak.8 PFGE has the advantage of being able to identify subclones of the same clone20 and has been systematically used to identify N. meningitidis outbreaks.7,21–23 In this study, we identified 2 PFGE patterns among strains belonging to the same clone (ST-103 complex) and observed excellent correlation between the epidemiological data and PFGE results: all the 4 strains isolated from the cases linked with the party had indistinguishable PFGE, consistent with an outbreak; in addition, PFGE was able to differentiate the outbreak strain from the case that was not linked to the party.
Overcrowding facilitates the spread of meningococcal carriage and, in susceptible individuals infected with a virulent strain, subsequent disease. Our data suggest that the party could have provided an opportunity for the dissemination of N. meningitidis. Four MD cases linked to the party, including 3 survivors and 1 who died, were users of illicit drugs or used cocaine at the party. The short period between the party and the onset of symptoms, in addition to genetic similarity of the strains, allow us to hypothesize that the cocaine inhalation associated with the party could have predisposed to invasive disease through injury to the respiratory mucosa.24 An outbreak of MD involving illicit drugs use was reported in New York, with cocaine use reported as the most common risk factor for MD.25 MD has also been associated with other factors that can promote a breakdown in host defense mechanisms or damage to the upper respiratory tract, such as influenza and others acute respiratory diseases.21,26,27
Other social behaviors associated with MD include alcohol consumption, cigarette smoking, and attendance at nightclubs, discotheques, and bars.22,23,28 Other crowded environments, such as the Hajj pilgrimage, educational and military institutions have also been associated with outbreaks, indicating that crowding also facilitates transmission.29,30
In the outbreak described here, all the party cases occurred within 5 days of the event, similar to an outbreak of serogroup C disease associated with nightclub attendance in Australia.21
The combination of epidemiologic data and molecular characterization were essential for understanding this outbreak. To our knowledge, this is the first reported MD outbreak associated with the serogroup C ST-103 complex and the first reported party and illicit drug use-associated outbreak in Brazil.
Conflict of interestThe authors declare no conflicts of interest related to this study.
We thank Joana D’Arc dos Reis, the coordinator of Public Health Laboratories, Ministry of Health from 2008 to 2010; Marta Galhardo, Conceição Zanelato and Maria Vaneide de Paiva for serogrouping and antimicrobial susceptibility testing the isolates; Samanta Cristine Grassi Almeida for assistance with Bionumerics software. This work was supported in part by a career development award to Lee H Harrison, National Institute of Allergy and Infectious Diseases (K24 AI52788); and by a Fogarty International Center Global Infectious Diseases Research Training Program grant, National Institutes of Health, to the University of Pittsburgh (D43TW006592).

