




The EASYCare is a multidimensional assessment tool for older people, which corresponds to the concerns and priorities of older people in relation to their needs, health, and quality of life. The EASYCare instrument has been used in many countries worldwide. Lack of reliability evidence has recently been raised by researchers. This study aimed to test the validity and reliability of the EASYCare-2010 instrument in community-dwelling Portuguese older people attended in Primary Health Care centres.
MethodsThe sample for this transversal study (N=244) was collected from Portuguese Primary Health Care Centers. Categorical Principal Component Analysis was used to assess the underlying dimensions of EASYCare-2010. Construct validity was evaluated through correlation with the World Health Organization Quality of Life Assessment Instrument-Short Form.
ResultsA two-factor model (labelled “mobility and activities of daily life”, and “general well-being and safety”) was found. The EASYCare-2010 instrument showed acceptable levels for internal consistency (≥0.70). The EASYCare-2010 factors were correlated with measures of quality of life. Results showed that in most polytomous items, some of the more extreme categories were not considered at all or only by a residual number of participants.
ConclusionEASY Care -2010 version is a valid and reliable instrument for holistic assessment of the older people attended in Primary Health Care centres in Portugal.
El EASYCare es una herramienta de evaluación multidimensional para las personas mayores, que corresponde a las preocupaciones y prioridades de las personas mayores en relación con sus necesidades, salud y calidad de vida. El instrumento EASYCare se ha utilizado en muchos países del mundo. La falta de pruebas de fiabilidad ha sido planteada recientemente por los investigadores. Este estudio tuvo como objetivo probar la validez y fiabilidad del instrumento EASYCare-2010 en personas mayores portuguesas residentes en la comunidad, atendidos en centros de Atención Primaria de la Salud.
MétodosLa muestra para este estudio transversal (N = 244) se recogió en Centros de Atención Primaria de Portugal. Se utilizó el Análisis de Componentes Principales Categórico para evaluar las dimensiones subyacentes de EASYCare-2010. La validez del constructo se evaluó mediante la correlación con el instrumento de evaluación de la calidad de vida de la Organización Mundial de la Salud, instrumento en su forma corta.
ResultadosSe encontró un modelo de dos factores (denominado «movilidad y actividades de la vida diaria» y «bienestar general y seguridad»). El instrumento EASYCare-2010 mostró niveles aceptables de consistencia interna (≥ 0.70). Los factores EASYCare-2010 se correlacionaron con medidas de calidad de vida. Los resultados mostraron que en la mayoría de ítems politómicos en algunas categorías extremas no se consideraron o solo por un número residual de participantes.
ConclusiónLa versión EASY Care-2010 es un instrumento válido y fiable para la evaluación holística de las personas mayores atendidas en centros de Atención Primaria de Salud en Portugal.
Portugal is ageing at an accelerated pace, where 19.9% of the population are 65 years or older and the estimates indicate that by 2030 it will have the third oldest population within Europe.1 Many consequences from the ageing population have been occurring over the past few years, namely arising in the prevalence of non-communicable chronic diseases,2 increased rates of falls,3 reduced mobility, increased morbidity and prolonged hospitalization.4 These factors show that priority in Primary Health Care and community services should be given to meet older people's needs to delay or reduce loss of independence and autonomy.5 In addition, many studies have shown that it is possible to prevent and decrease the growing problems of ageing with valid and sustainable interventions.6,7 However, there is still evidence of a gap in the development of interventions aimed at meeting the needs of older people.
Since 1999, the EASYCare instrument has been used in many countries worldwide to measure and identify the unmet health care needs of older people.8–10 The EASYCare assessment is a multidimensional assessment tool for older people, which corresponds to the concerns and priorities of older people in relation to their needs, health, and quality of life.11 This tool is a simple and feasible instrument that evaluates physical function, including activities of daily living (ADL) and instrumental activities of daily living (IADL), mental functioning, social functioning and well-being.11–15
Changes were made in the form and content of the instrument since 1999. Actually, there are 49 questions included as a check list across seven domains of physical, mental, and social care functioning replacing the previous versions,11 giving rise to the current version (EASY-Care Standard version 2010) designated in this study as the EASYCare-2010. The EASYCare-2010 version is unlike previous versions and more extensive.
In a recent review of EASYCare about the existing evidence of reliability, validity and acceptability and its appropriateness for assessing the needs of community-dwelling older people, it was concluded that research is needed to establishing concurrent and convergent validity of the EASYCare instrument.16 The aim of this study was to analyze the validity and reliability of the EASYCare-2010 in community-dwelling Portuguese older people attending Primary Health Care centres.
MethodsThis cross-sectional study comprises 244 participants, recruited at Primary Health Care centers from the Portuguese National Health Service at Regional Health Administration of central Portugal. The sample was collected from October 2013 to June 2014. The procedure for selection took account of the fact that there is nothing to indicate that subjects would differ from the study population, with respect to the variables investigated, depending on the time of the day at which they are attended in the PHC, or even the time of year. The sample size was estimated considering a minimum subject to item ratio of at least five-to-one. Three nurses and one gerontologist interviewers received training in the standardized use of the EASYCare-2010. Each participant was interviewed by one interviewer. Inclusion criteria were 65 years of age or older and without dementia, psychosis or mental retardation as reported by their physician.
The study was approved by the Ethics Committee of the central Regional Health Administration (Coimbra, Portugal) with the local code 006386 on 12th March, 2013. Before the data collection, all participants were informed about the study and signed the informed consent form. Permission for using the EASYCare-2010 instrument has been obtained from the “EASYCare Foundation Ltd. (http://www.easycarehealth.co.uk/)” which maintains the EASYCare tool.
Construct validity was evaluated through correlation with the World Health Organization Quality of Life - BREF (WHOQOL-BREF).17 The WHOQOL-BREF is a 26-item, multidimensional, self-administered scale covering four domains: psychological, social relationships, physical health and environmental issues. Items are rated on a 5-point Likert scale where 1 indicates very negative perceptions, and 5 indicates highly positive perceptions. High scores demonstrate good quality of life in each domain. Quality of life was measured with the Portuguese version of the WHOQOL-BREF.18
Statistical analysis was performed with SPSS (version 22.0) and two-sided significance tests at the 5% level were used throughout. Categorical variables were described as percentages and quantitative variables as means±standard deviation (SD).
Prior to performing the factor analysis, a careful inspection of EASYCare-2010 was performed in order to define an adequate strategy for its validation. This inspection included both the identification of the number of categories of each item, polychotomous or dichotomous, and a descriptive analysis.
A categorical principle component analysis (CAPTCA)19 was performed to determine the underlying dimensions of the EASYCare-2010 items. The number of factors to be extracted was determined by considering the Eigenvalue criterion: factors with eigenvalues greater than 1 should be retained. The internal consistency criterion was: factor extractions/dimensions with a Cronbach's alpha greater than or equal to 0.70 (i.e., suggesting acceptable internal consistency for that particular factor) should be retained. Cronbach's alpha was used to estimate instrument reliability.
The retaining criteria established in advance for the selection of factor items were: (a) factor loading of 0.4 or higher, (b) at least a 0.10 difference compared to the other factors, (c) having at least three items for one factor, and (d) interpretability.
Construct validity was performed based on the analysis of Pearson correlations computed between the EASYCare-2010 and the World Health Organization Quality of Life Assessment Instrument-Short Form (WHOQOL-BREF). For the correlation coefficients, the following interpretations were used: large if greater than 0.50, moderate correlation for values between 0.30 and 0.49, and small from 0.10 to 0.29.20
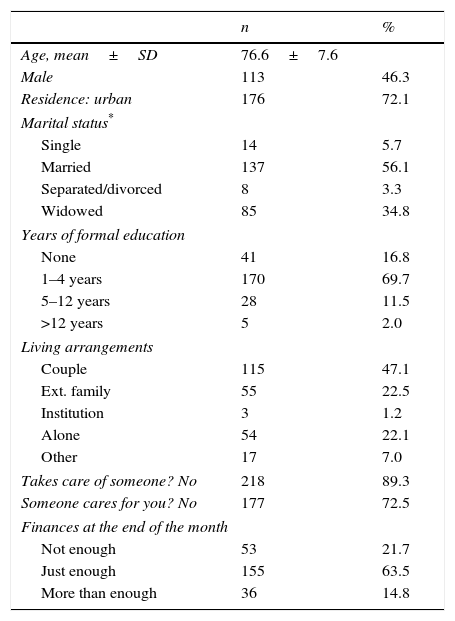
ResultsTable 1 summarizes the socio-demographic characteristics of the 244 participants, 46.3% were males. Almost all participants were married or widowed (91%), 69.6% lived as a couple or with extended family. The majority of the participants had less than 5 years of formal education (86.5%). About 20% of the participants reported that their finances were not enough to cover their expenses until the end of the month.
Socio-demographic characteristics of the participants (N=244).
| n | % | |
|---|---|---|
| Age, mean±SD | 76.6±7.6 | |
| Male | 113 | 46.3 |
| Residence: urban | 176 | 72.1 |
| Marital status* | ||
| Single | 14 | 5.7 |
| Married | 137 | 56.1 |
| Separated/divorced | 8 | 3.3 |
| Widowed | 85 | 34.8 |
| Years of formal education | ||
| None | 41 | 16.8 |
| 1–4 years | 170 | 69.7 |
| 5–12 years | 28 | 11.5 |
| >12 years | 5 | 2.0 |
| Living arrangements | ||
| Couple | 115 | 47.1 |
| Ext. family | 55 | 22.5 |
| Institution | 3 | 1.2 |
| Alone | 54 | 22.1 |
| Other | 17 | 7.0 |
| Takes care of someone? No | 218 | 89.3 |
| Someone cares for you? No | 177 | 72.5 |
| Finances at the end of the month | ||
| Not enough | 53 | 21.7 |
| Just enough | 155 | 63.5 |
| More than enough | 36 | 14.8 |
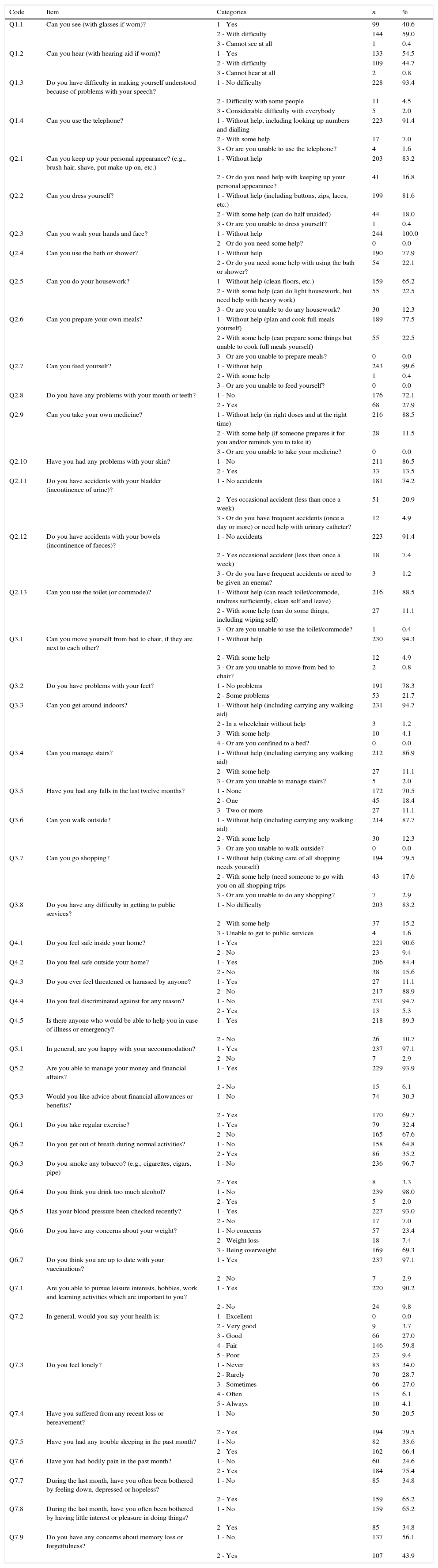
The descriptive analysis of the items of the EASYCare-2010 instrument gave information about whether all response options were considered by the participants (Table 2). The majority of the questions (27 over 49) of the EASYCare-2010 instrument correspond to dichotomous items, 2 items have 5 response categories, 1 item has 4 categories and the other items have 3 response categories (Table 2). The descriptive analysis revealed that in almost all the 20 items with 3 or 4 categories, the more extreme category had very low frequencies or none (5/20). Although merging of adjoining categories should be avoided, because it can affect the quality of the data,21 categories with very low frequencies can cause instability of the principal component analysis solution. The bottom threshold of 8 for categories that should be merged with an adjacent category was considered.19 Adjoining categories in the 3 and 4 response items led to dichotomous items (items Q1.1, Q1.2, Q1,3, Q1.4, Q2.2, Q2.5, Q2.11, Q2.12, Q2.13, Q3.1, Q3.3, Q3.4, Q3.5, Q3.7, Q3.8 and Q6.6). The resulting categories are given in Table 2. Items where all, or almost all participants, scored the same category, were not considered in the factor analysis (items Q2.3, Q2.7, Q5.1, Q6.3, Q6.4, and Q6.7). The resulting items were all dichotomous, with the exception of the 2 items with 5 response categories (items Q7.2 and Q7.3).
Descriptive of the items of the EASYCare-2010 instrument (N=244).
| Code | Item | Categories | n | % |
|---|---|---|---|---|
| Q1.1 | Can you see (with glasses if worn)? | 1 - Yes | 99 | 40.6 |
| 2 - With difficulty | 144 | 59.0 | ||
| 3 - Cannot see at all | 1 | 0.4 | ||
| Q1.2 | Can you hear (with hearing aid if worn)? | 1 - Yes | 133 | 54.5 |
| 2 - With difficulty | 109 | 44.7 | ||
| 3 - Cannot hear at all | 2 | 0.8 | ||
| Q1.3 | Do you have difficulty in making yourself understood because of problems with your speech? | 1 - No difficulty | 228 | 93.4 |
| 2 - Difficulty with some people | 11 | 4.5 | ||
| 3 - Considerable difficulty with everybody | 5 | 2.0 | ||
| Q1.4 | Can you use the telephone? | 1 - Without help, including looking up numbers and dialling | 223 | 91.4 |
| 2 - With some help | 17 | 7.0 | ||
| 3 - Or are you unable to use the telephone? | 4 | 1.6 | ||
| Q2.1 | Can you keep up your personal appearance? (e.g., brush hair, shave, put make-up on, etc.) | 1 - Without help | 203 | 83.2 |
| 2 - Or do you need help with keeping up your personal appearance? | 41 | 16.8 | ||
| Q2.2 | Can you dress yourself? | 1 - Without help (including buttons, zips, laces, etc.) | 199 | 81.6 |
| 2 - With some help (can do half unaided) | 44 | 18.0 | ||
| 3 - Or are you unable to dress yourself? | 1 | 0.4 | ||
| Q2.3 | Can you wash your hands and face? | 1 - Without help | 244 | 100.0 |
| 2 - Or do you need some help? | 0 | 0.0 | ||
| Q2.4 | Can you use the bath or shower? | 1 - Without help | 190 | 77.9 |
| 2 - Or do you need some help with using the bath or shower? | 54 | 22.1 | ||
| Q2.5 | Can you do your housework? | 1 - Without help (clean floors, etc.) | 159 | 65.2 |
| 2 - With some help (can do light housework, but need help with heavy work) | 55 | 22.5 | ||
| 3 - Or are you unable to do any housework? | 30 | 12.3 | ||
| Q2.6 | Can you prepare your own meals? | 1 - Without help (plan and cook full meals yourself) | 189 | 77.5 |
| 2 - With some help (can prepare some things but unable to cook full meals yourself) | 55 | 22.5 | ||
| 3 - Or are you unable to prepare meals? | 0 | 0.0 | ||
| Q2.7 | Can you feed yourself? | 1 - Without help | 243 | 99.6 |
| 2 - With some help | 1 | 0.4 | ||
| 3 - Or are you unable to feed yourself? | 0 | 0.0 | ||
| Q2.8 | Do you have any problems with your mouth or teeth? | 1 - No | 176 | 72.1 |
| 2 - Yes | 68 | 27.9 | ||
| Q2.9 | Can you take your own medicine? | 1 - Without help (in right doses and at the right time) | 216 | 88.5 |
| 2 - With some help (if someone prepares it for you and/or reminds you to take it) | 28 | 11.5 | ||
| 3 - Or are you unable to take your medicine? | 0 | 0.0 | ||
| Q2.10 | Have you had any problems with your skin? | 1 - No | 211 | 86.5 |
| 2 - Yes | 33 | 13.5 | ||
| Q2.11 | Do you have accidents with your bladder (incontinence of urine)? | 1 - No accidents | 181 | 74.2 |
| 2 - Yes occasional accident (less than once a week) | 51 | 20.9 | ||
| 3 - Or do you have frequent accidents (once a day or more) or need help with urinary catheter? | 12 | 4.9 | ||
| Q2.12 | Do you have accidents with your bowels (incontinence of faeces)? | 1 - No accidents | 223 | 91.4 |
| 2 - Yes occasional accident (less than once a week) | 18 | 7.4 | ||
| 3 - Or do you have frequent accidents or need to be given an enema? | 3 | 1.2 | ||
| Q2.13 | Can you use the toilet (or commode)? | 1 - Without help (can reach toilet/commode, undress sufficiently, clean self and leave) | 216 | 88.5 |
| 2 - With some help (can do some things, including wiping self) | 27 | 11.1 | ||
| 3 - Or are you unable to use the toilet/commode? | 1 | 0.4 | ||
| Q3.1 | Can you move yourself from bed to chair, if they are next to each other? | 1 - Without help | 230 | 94.3 |
| 2 - With some help | 12 | 4.9 | ||
| 3 - Or are you unable to move from bed to chair? | 2 | 0.8 | ||
| Q3.2 | Do you have problems with your feet? | 1 - No problems | 191 | 78.3 |
| 2 - Some problems | 53 | 21.7 | ||
| Q3.3 | Can you get around indoors? | 1 - Without help (including carrying any walking aid) | 231 | 94.7 |
| 2 - In a wheelchair without help | 3 | 1.2 | ||
| 3 - With some help | 10 | 4.1 | ||
| 4 - Or are you confined to a bed? | 0 | 0.0 | ||
| Q3.4 | Can you manage stairs? | 1 - Without help (including carrying any walking aid) | 212 | 86.9 |
| 2 - With some help | 27 | 11.1 | ||
| 3 - Or are you unable to manage stairs? | 5 | 2.0 | ||
| Q3.5 | Have you had any falls in the last twelve months? | 1 - None | 172 | 70.5 |
| 2 - One | 45 | 18.4 | ||
| 3 - Two or more | 27 | 11.1 | ||
| Q3.6 | Can you walk outside? | 1 - Without help (including carrying any walking aid) | 214 | 87.7 |
| 2 - With some help | 30 | 12.3 | ||
| 3 - Or are you unable to walk outside? | 0 | 0.0 | ||
| Q3.7 | Can you go shopping? | 1 - Without help (taking care of all shopping needs yourself) | 194 | 79.5 |
| 2 - With some help (need someone to go with you on all shopping trips | 43 | 17.6 | ||
| 3 - Or are you unable to do any shopping? | 7 | 2.9 | ||
| Q3.8 | Do you have any difficulty in getting to public services? | 1 - No difficulty | 203 | 83.2 |
| 2 - With some help | 37 | 15.2 | ||
| 3 - Unable to get to public services | 4 | 1.6 | ||
| Q4.1 | Do you feel safe inside your home? | 1 - Yes | 221 | 90.6 |
| 2 - No | 23 | 9.4 | ||
| Q4.2 | Do you feel safe outside your home? | 1 - Yes | 206 | 84.4 |
| 2 - No | 38 | 15.6 | ||
| Q4.3 | Do you ever feel threatened or harassed by anyone? | 1 - Yes | 27 | 11.1 |
| 2 - No | 217 | 88.9 | ||
| Q4.4 | Do you feel discriminated against for any reason? | 1 - No | 231 | 94.7 |
| 2 - Yes | 13 | 5.3 | ||
| Q4.5 | Is there anyone who would be able to help you in case of illness or emergency? | 1 - Yes | 218 | 89.3 |
| 2 - No | 26 | 10.7 | ||
| Q5.1 | In general, are you happy with your accommodation? | 1 - Yes | 237 | 97.1 |
| 2 - No | 7 | 2.9 | ||
| Q5.2 | Are you able to manage your money and financial affairs? | 1 - Yes | 229 | 93.9 |
| 2 - No | 15 | 6.1 | ||
| Q5.3 | Would you like advice about financial allowances or benefits? | 1 - No | 74 | 30.3 |
| 2 - Yes | 170 | 69.7 | ||
| Q6.1 | Do you take regular exercise? | 1 - Yes | 79 | 32.4 |
| 2 - No | 165 | 67.6 | ||
| Q6.2 | Do you get out of breath during normal activities? | 1 - No | 158 | 64.8 |
| 2 - Yes | 86 | 35.2 | ||
| Q6.3 | Do you smoke any tobacco? (e.g., cigarettes, cigars, pipe) | 1 - No | 236 | 96.7 |
| 2 - Yes | 8 | 3.3 | ||
| Q6.4 | Do you think you drink too much alcohol? | 1 - No | 239 | 98.0 |
| 2 - Yes | 5 | 2.0 | ||
| Q6.5 | Has your blood pressure been checked recently? | 1 - Yes | 227 | 93.0 |
| 2 - No | 17 | 7.0 | ||
| Q6.6 | Do you have any concerns about your weight? | 1 - No concerns | 57 | 23.4 |
| 2 - Weight loss | 18 | 7.4 | ||
| 3 - Being overweight | 169 | 69.3 | ||
| Q6.7 | Do you think you are up to date with your vaccinations? | 1 - Yes | 237 | 97.1 |
| 2 - No | 7 | 2.9 | ||
| Q7.1 | Are you able to pursue leisure interests, hobbies, work and learning activities which are important to you? | 1 - Yes | 220 | 90.2 |
| 2 - No | 24 | 9.8 | ||
| Q7.2 | In general, would you say your health is: | 1 - Excellent | 0 | 0.0 |
| 2 - Very good | 9 | 3.7 | ||
| 3 - Good | 66 | 27.0 | ||
| 4 - Fair | 146 | 59.8 | ||
| 5 - Poor | 23 | 9.4 | ||
| Q7.3 | Do you feel lonely? | 1 - Never | 83 | 34.0 |
| 2 - Rarely | 70 | 28.7 | ||
| 3 - Sometimes | 66 | 27.0 | ||
| 4 - Often | 15 | 6.1 | ||
| 5 - Always | 10 | 4.1 | ||
| Q7.4 | Have you suffered from any recent loss or bereavement? | 1 - No | 50 | 20.5 |
| 2 - Yes | 194 | 79.5 | ||
| Q7.5 | Have you had any trouble sleeping in the past month? | 1 - No | 82 | 33.6 |
| 2 - Yes | 162 | 66.4 | ||
| Q7.6 | Have you had bodily pain in the past month? | 1 - No | 60 | 24.6 |
| 2 - Yes | 184 | 75.4 | ||
| Q7.7 | During the last month, have you often been bothered by feeling down, depressed or hopeless? | 1 - No | 85 | 34.8 |
| 2 - Yes | 159 | 65.2 | ||
| Q7.8 | During the last month, have you often been bothered by having little interest or pleasure in doing things? | 1 - No | 159 | 65.2 |
| 2 - Yes | 85 | 34.8 | ||
| Q7.9 | Do you have any concerns about memory loss or forgetfulness? | 1 - No | 137 | 56.1 |
| 2 - Yes | 107 | 43.9 |
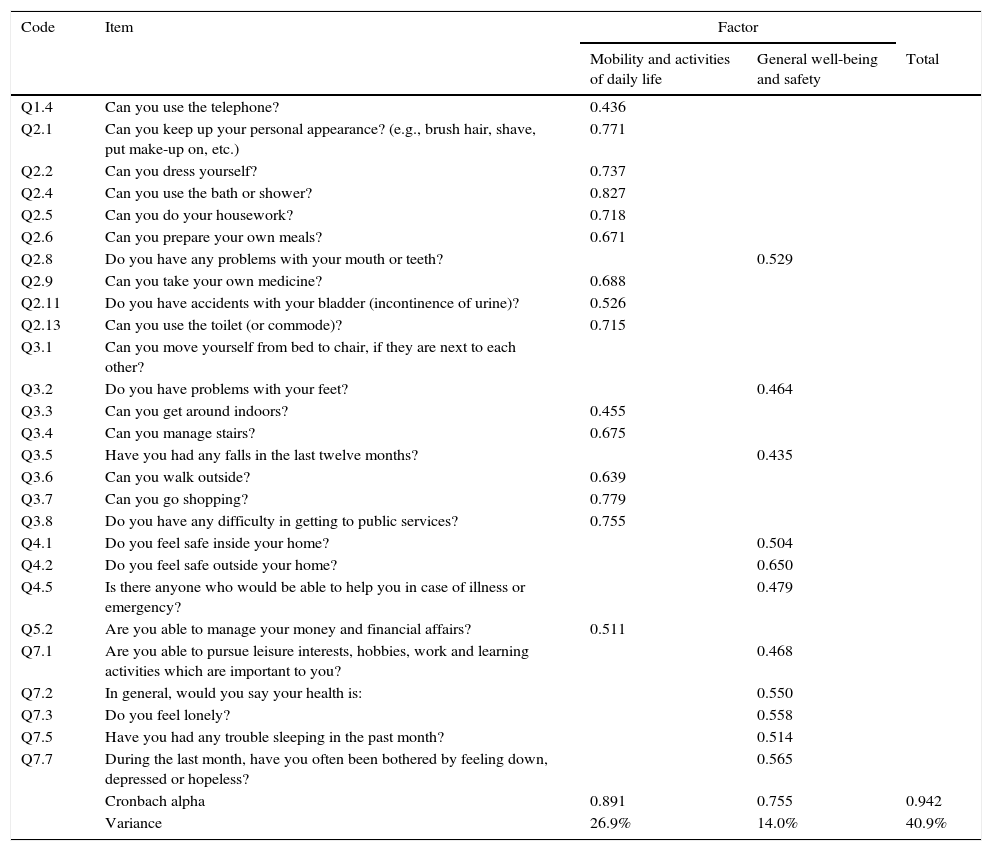
The factor model for the Portuguese population was identified using the CATPCA approach. A two-factor solution was suggested, by both the eigenvalue and the internal consistency criterion. The first component explained 26.9% of the total variance and the second 14.0%. This means that the two selected components explain 40.9% of the variance.
Items, factor loading and alpha coefficients for the two-factor solution are presented in Table 3. The first factor labelled “Mobility and Activities of Daily Life” consists of fifteen items and the second factor, labelled “General well-being and safety” consists of eleven items reflecting self-perception of health and self-perceived safety. Individuals with low values perceive the greatest levels of activity and well-being respectively.
Factor loadings in the EASYCare-2010 instrument (N=244).
| Code | Item | Factor | ||
|---|---|---|---|---|
| Mobility and activities of daily life | General well-being and safety | Total | ||
| Q1.4 | Can you use the telephone? | 0.436 | ||
| Q2.1 | Can you keep up your personal appearance? (e.g., brush hair, shave, put make-up on, etc.) | 0.771 | ||
| Q2.2 | Can you dress yourself? | 0.737 | ||
| Q2.4 | Can you use the bath or shower? | 0.827 | ||
| Q2.5 | Can you do your housework? | 0.718 | ||
| Q2.6 | Can you prepare your own meals? | 0.671 | ||
| Q2.8 | Do you have any problems with your mouth or teeth? | 0.529 | ||
| Q2.9 | Can you take your own medicine? | 0.688 | ||
| Q2.11 | Do you have accidents with your bladder (incontinence of urine)? | 0.526 | ||
| Q2.13 | Can you use the toilet (or commode)? | 0.715 | ||
| Q3.1 | Can you move yourself from bed to chair, if they are next to each other? | |||
| Q3.2 | Do you have problems with your feet? | 0.464 | ||
| Q3.3 | Can you get around indoors? | 0.455 | ||
| Q3.4 | Can you manage stairs? | 0.675 | ||
| Q3.5 | Have you had any falls in the last twelve months? | 0.435 | ||
| Q3.6 | Can you walk outside? | 0.639 | ||
| Q3.7 | Can you go shopping? | 0.779 | ||
| Q3.8 | Do you have any difficulty in getting to public services? | 0.755 | ||
| Q4.1 | Do you feel safe inside your home? | 0.504 | ||
| Q4.2 | Do you feel safe outside your home? | 0.650 | ||
| Q4.5 | Is there anyone who would be able to help you in case of illness or emergency? | 0.479 | ||
| Q5.2 | Are you able to manage your money and financial affairs? | 0.511 | ||
| Q7.1 | Are you able to pursue leisure interests, hobbies, work and learning activities which are important to you? | 0.468 | ||
| Q7.2 | In general, would you say your health is: | 0.550 | ||
| Q7.3 | Do you feel lonely? | 0.558 | ||
| Q7.5 | Have you had any trouble sleeping in the past month? | 0.514 | ||
| Q7.7 | During the last month, have you often been bothered by feeling down, depressed or hopeless? | 0.565 | ||
| Cronbach alpha | 0.891 | 0.755 | 0.942 | |
| Variance | 26.9% | 14.0% | 40.9% | |
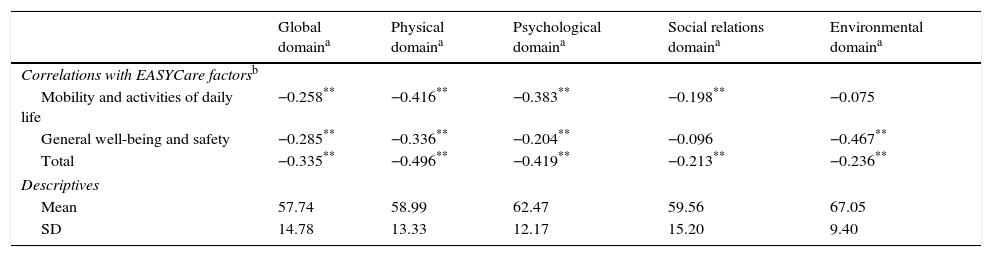
Table 4 shows Pearson correlations between the two retained EASYCare-2010 factors and the domains of the quality of life assessment instrument considered (WHOQOL-BREF). All measurements were significantly and negatively correlated with the EASYCare-2010 factors, with only one exception (social relations), meaning that increased perception of levels of activity or wellbeing were related to higher scores of quality of life. The EASYCare-2010 factor labelled “General well-being and safety” showed the highest correlations with the environmental domain of quality of life (−0.467). The highest correlation with the EASYCare-2010 factor labelled “Mobility and Activities of Daily Life” was the physical domain of quality of life (−0.416).
Pearson correlations between EASYCare-2010 factors and scores of World Health Organization Quality of Life Assessment Instrument – Short Form (WHOQOL-BREF) (N=244).
| Global domaina | Physical domaina | Psychological domaina | Social relations domaina | Environmental domaina | |
|---|---|---|---|---|---|
| Correlations with EASYCare factorsb | |||||
| Mobility and activities of daily life | −0.258** | −0.416** | −0.383** | −0.198** | −0.075 |
| General well-being and safety | −0.285** | −0.336** | −0.204** | −0.096 | −0.467** |
| Total | −0.335** | −0.496** | −0.419** | −0.213** | −0.236** |
| Descriptives | |||||
| Mean | 57.74 | 58.99 | 62.47 | 59.56 | 67.05 |
| SD | 14.78 | 13.33 | 12.17 | 15.20 | 9.40 |
Individuals with low values have low, negative perceptions and high scores demonstrate good quality of life in each domain.
The results of this study contribute to scientific evidence that the EASYCare-2010 is a reliable and valid instrument that can be used in the Portuguese older community-dwelling people attended in Primary Health Care centres.
Given the relevance of EASYCare in identifying the unmet health care needs of older people in many countries worldwide,15 it was considered important to confirm the operationalization of the instrument and its dimensional structure.
The CAPTCA analysis revealed a two-factor model, reflecting self-perceived activity capacities and well-being. The first factor was labelled “Mobility and Activities of Daily Life”, and the second factor “General well-being and safety”. The overall Cronbach's alpha values for the factors were acceptable, indicating satisfactory internal consistency of the scale. The considerably high levels of QOL found in all domains may be explained by the fact that almost all individuals were living in the community. As expected, all factors from the EASYCare-2010 and the quality of life (WHOQOL-BREF) domains were negatively correlated, indicating discriminative validity.
One of the main steps in the analysis of the EASYCare-2010 tool was a careful inspection of the instrument. The conclusion was that in almost all polychotomous items the more extreme response options were not selected at all, or just by a few number of participants. The frequencies of the more extreme categories of several items were very low or even null, questioning the adequacy of those particular categories for Portuguese older people in community settings of primary care. Fewer than five people considered themselves unable to see or hear at all, totally unable to use the telephone, dress themselves, use the toilet/commode or move from the bed to a chair, have frequent accidents or need to be given an enema. No participants felt they needed help washing their hands and face, 22.5% reported that with some help they could prepare meals but no-one considered themselves to be totally incapable of preparing meals. This same trend was observed for the ability to take their medication. With the exception of one participant, who reported needing some help to feed himself, no-one reported being totally incapable of feeding themselves. No participants reported being confined to a bed. Although this last option is perhaps the most unfeasible for participants recruited from community settings of primary care centres, the others that were considered by none or very few participants, correspond to a level of incapacity that is rarely found in Primary Health Care. These options could be adequate for the elderly in other settings such as in hospital units, nursing homes or at home and unable to travel, but not for the elderly that need some autonomy to be able to attend a Primary Health Care for face-to-face consultation.
Results from this study showed that the EASYCare-2010 items could be presented in a simpler format, since some of the categories were not considered at all or only by a residual number or participants. Excluding these extreme categories, the EASYCare-2010 could become a simpler instrument, with dichotomous items replacing polychotomous items, requiring a choice between two alternatives (yes-no) instead of one of three or more alternative responses. Binary items are easier to answer, while polychotomous items demand additional concentration on finer distinctions.22 Since there may be older people who only show extreme deficits in one category, this level of sensitivity would still be clinically useful, and the EASYCare-2010 instrument could be reorganized while maintaining all response options. Polychotomous items could be replaced by dichotomous items, but when a problem is identified a second level of items would identify its severity. A reduction of items should be considered in a new revised version of the EASYCare-2010, in line also with the first meeting at the Consensus Conference sponsored by the WHO in 1993 and with the interest showed by workers and researchers from six different countries.11
Considering that the EASYCare instrument is intended to identify or recognize threats to health, well-being and independence of older people at an early stage of morbidity with a simple and fast approach,23 the findings of this study point to the benefits of a reduction of alternatives when asked to choose one answer. The dichotomous format of questions could more easily alert for the importance of being attentive to an answer which, although not of in itself revealing threat, would warrant clinical evaluation. Alternatively, more rapid assessment methods, for example through a call centre approach may facilitate a more comprehensive but efficient approach to assessment. Because the organization of Primary Health Care is not homogeneous across countries,24 it would be important to validate the instrument in the various locations around the world using EASYCare. Similar or different results obtained by the different countries and cultures would point to the necessary modifications in the review and updating of the instrument for use beyond 2016.
- •
The EASYCare is a holistic assessment of the health and care needs of older people.
- •
In order to extend healthy active life the EASYCare is a tool that helps in the identification of the threats to health independence and well-being in old age.
- •
The EASYCare-2010 version is unlike the previous versions more extensive but lack of validity and reliability evidence of EASYCare has been raised recently by the scientific community.
- •
This study showed that the EASYCare-2010 could become a simpler instrument, with dichotomous items replacing polytomous items.
- •
This study showed that in Portugal the EASYCare-2010 is a valid and reliable scale for the assessment of needs among older community-dwelling people.
Ian Philp is a Director of the EASYCare Foundation Ltd, which holds the international copyright for all EASYCare tools and methods. The EASYCare Standard assessment is available free of charge once registered with the Foundation. Any commercialisation of EASYCare methods by third parties must be approved by the Foundation with royalties paid. Foundation profits are distributed to charities.
We thank Margaret Gomes for providing linguistic support and useful comments in the manuscript.
The work was presented in the 3rd IPLeiria's International Health Congress Portugal (May 6 & 7, 2016) as an oral communication and the abstract which is published on the BMC Health Services Research 2016, Vol. 16 Suppl. 3; DOI: 10.1186/s12913-016-1423-5.
