




The resting electrocardiogram (ECG) is a widely available, low-cost, and safe tool. It is commonly performed for cardiovascular disease screening, prediction of higher mortality risk, and, promotion of cardiovascular safety.1
An increasing number of studies have shown that discrete ECG alterations in children and young adults are related to age, gender,2 increased BMI (Body Mass Index),3 and consumption of energy drinks4 or alcohol.5
Therefore, we decided to extend our observations by studying the electrocardiographic parameters in healthy students from the División Académica de Ciencias de la Salud of the Universidad Juárez Autónoma de Tabasco (UJAT-DACS), Tabasco, México.
A descriptive, cross-sectional, analytical study was conducted. The following variables were collected: demographic (age and sex), anthropometric measures (weight, height, and BMI), comorbidities, personal, and family history, and 12 lead electrocardiograms. A standard 12-lead ECG was recorded in the supine position using a Bionet CARDIO 7 electrocardiograph at a paper speed of 25mm/s and voltage of 10mV/s, and an experienced cardiologist evaluated all the ECG. The variables were summarized according to their nature. To analyze the changes between sexes, we conducted the T-Test, χ2 test, or Fisher's exact test to compare using GraphPad Prism Software. Differences were considered statistically significant at p<0.05.
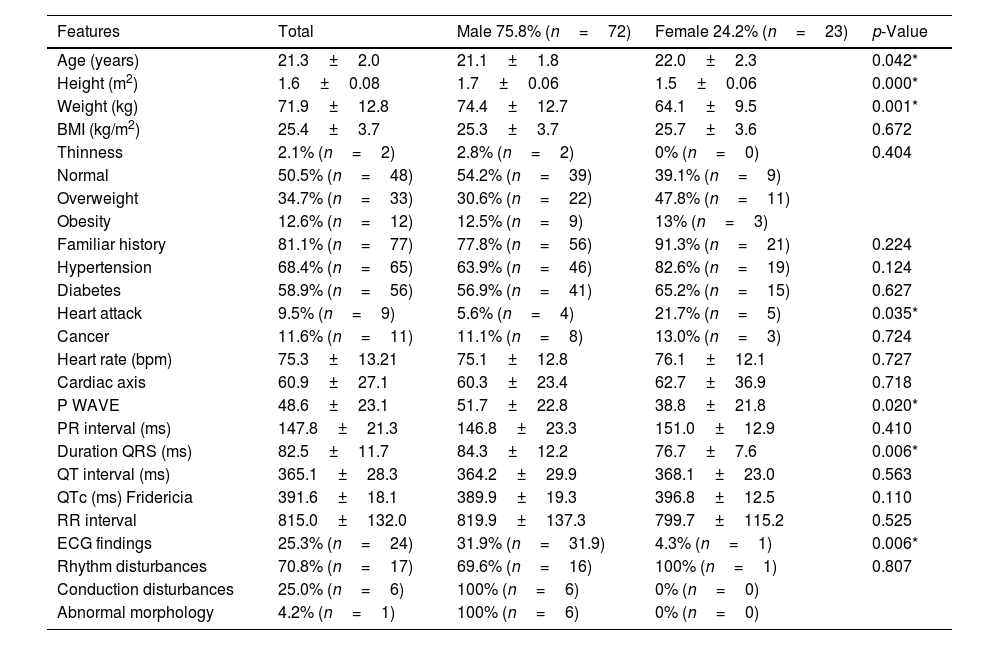
Finally, we examined the standard ECG in the 95 young adults. The mean age of the participants was 21.3±2.0 years, and 75.8% (n=72) were men. The mean body mass index of the group studied was 25.4±3.7kg/m2. In the overall study group, the heart rate mean was normal. Despite this fact, we demonstrated sex differences. More specifically, P wave (51.7±22.8 vs 38.8±21.8, p=0.020), and QRS duration (84.3±12.2 vs 76.7±7.6, p=0.006) were higher in males than women (Table 1), which is consistent with the reports of other studies. Van der Ende and coworkers suggested that the median duration of the P wave, the PQ interval, and the QRSd were higher in males compared with females.6 This observation raises the question that the physiology and anatomy of the male and female heart have important differences. In the heart, the arteries that irrigate it, and the size of the wall of the ventricles (the left one in particular) are smaller in women than in men. It has been described that the female heart has a higher ejection fraction and beats faster but generates a lower cardiac output.
Students features and values of ECG.
| Features | Total | Male 75.8% (n=72) | Female 24.2% (n=23) | p-Value |
|---|---|---|---|---|
| Age (years) | 21.3±2.0 | 21.1±1.8 | 22.0±2.3 | 0.042* |
| Height (m2) | 1.6±0.08 | 1.7±0.06 | 1.5±0.06 | 0.000* |
| Weight (kg) | 71.9±12.8 | 74.4±12.7 | 64.1±9.5 | 0.001* |
| BMI (kg/m2) | 25.4±3.7 | 25.3±3.7 | 25.7±3.6 | 0.672 |
| Thinness | 2.1% (n=2) | 2.8% (n=2) | 0% (n=0) | 0.404 |
| Normal | 50.5% (n=48) | 54.2% (n=39) | 39.1% (n=9) | |
| Overweight | 34.7% (n=33) | 30.6% (n=22) | 47.8% (n=11) | |
| Obesity | 12.6% (n=12) | 12.5% (n=9) | 13% (n=3) | |
| Familiar history | 81.1% (n=77) | 77.8% (n=56) | 91.3% (n=21) | 0.224 |
| Hypertension | 68.4% (n=65) | 63.9% (n=46) | 82.6% (n=19) | 0.124 |
| Diabetes | 58.9% (n=56) | 56.9% (n=41) | 65.2% (n=15) | 0.627 |
| Heart attack | 9.5% (n=9) | 5.6% (n=4) | 21.7% (n=5) | 0.035* |
| Cancer | 11.6% (n=11) | 11.1% (n=8) | 13.0% (n=3) | 0.724 |
| Heart rate (bpm) | 75.3±13.21 | 75.1±12.8 | 76.1±12.1 | 0.727 |
| Cardiac axis | 60.9±27.1 | 60.3±23.4 | 62.7±36.9 | 0.718 |
| P WAVE | 48.6±23.1 | 51.7±22.8 | 38.8±21.8 | 0.020* |
| PR interval (ms) | 147.8±21.3 | 146.8±23.3 | 151.0±12.9 | 0.410 |
| Duration QRS (ms) | 82.5±11.7 | 84.3±12.2 | 76.7±7.6 | 0.006* |
| QT interval (ms) | 365.1±28.3 | 364.2±29.9 | 368.1±23.0 | 0.563 |
| QTc (ms) Fridericia | 391.6±18.1 | 389.9±19.3 | 396.8±12.5 | 0.110 |
| RR interval | 815.0±132.0 | 819.9±137.3 | 799.7±115.2 | 0.525 |
| ECG findings | 25.3% (n=24) | 31.9% (n=31.9) | 4.3% (n=1) | 0.006* |
| Rhythm disturbances | 70.8% (n=17) | 69.6% (n=16) | 100% (n=1) | 0.807 |
| Conduction disturbances | 25.0% (n=6) | 100% (n=6) | 0% (n=0) | |
| Abnormal morphology | 4.2% (n=1) | 100% (n=6) | 0% (n=0) |
Abbreviations: BMI: body mass index.
It is worth noting that ECG findings were higher in males than females. The most common finding on ECG was premature Atrial Contraction (PAC), sinus bradycardia, pre-excitation syndrome, nodal rhythm, Right Bundle Branch Block (RBBB), Incomplete Right Bundle Branch Block (IRBBB), Short QT, and Brugada Pattern Type 2 and QT Prolonged.
To conclude, our findings in this prospective study support the notion of the usefulness of resting electrocardiogram (ECG). The screening ECG in healthy Mexican students suggests that a quarter of the sample had ECG findings, and the benchmark datasets grouped in rhythm disturbances, conduction disturbances, and abnormal morphology.
Ethical considerationsAll participants signed informed consent. This research was developed in reference to General Health Law regulations on Health Research and was approved by the Universidad Juárez Autónoma Research Committee with register number JI-LCA068.
FundingAny funding to declare.
Conflicts of interestAuthors have no conflict of interest.
