





5–10% of breast tumor patients develop local breast tumor recurrence. The absence of axillary re-staging could increase future local recurrence and mortality risk in these patients. The lymphoscintigraphy for sentinel lymph node biopsy in recurrences (rSLNB) using a radiotracer injection, can be an option to evaluate axillar status, but other factors known to alter the usual behaviour of SLN migration have to be taken into account, such as previous axillary surgery, breast surgery or adjuvant treatments. Our objective was to evaluate the relationship between these factors and the success rate of rSLNB (overall and aberrant drainage rates, metastases ratio).
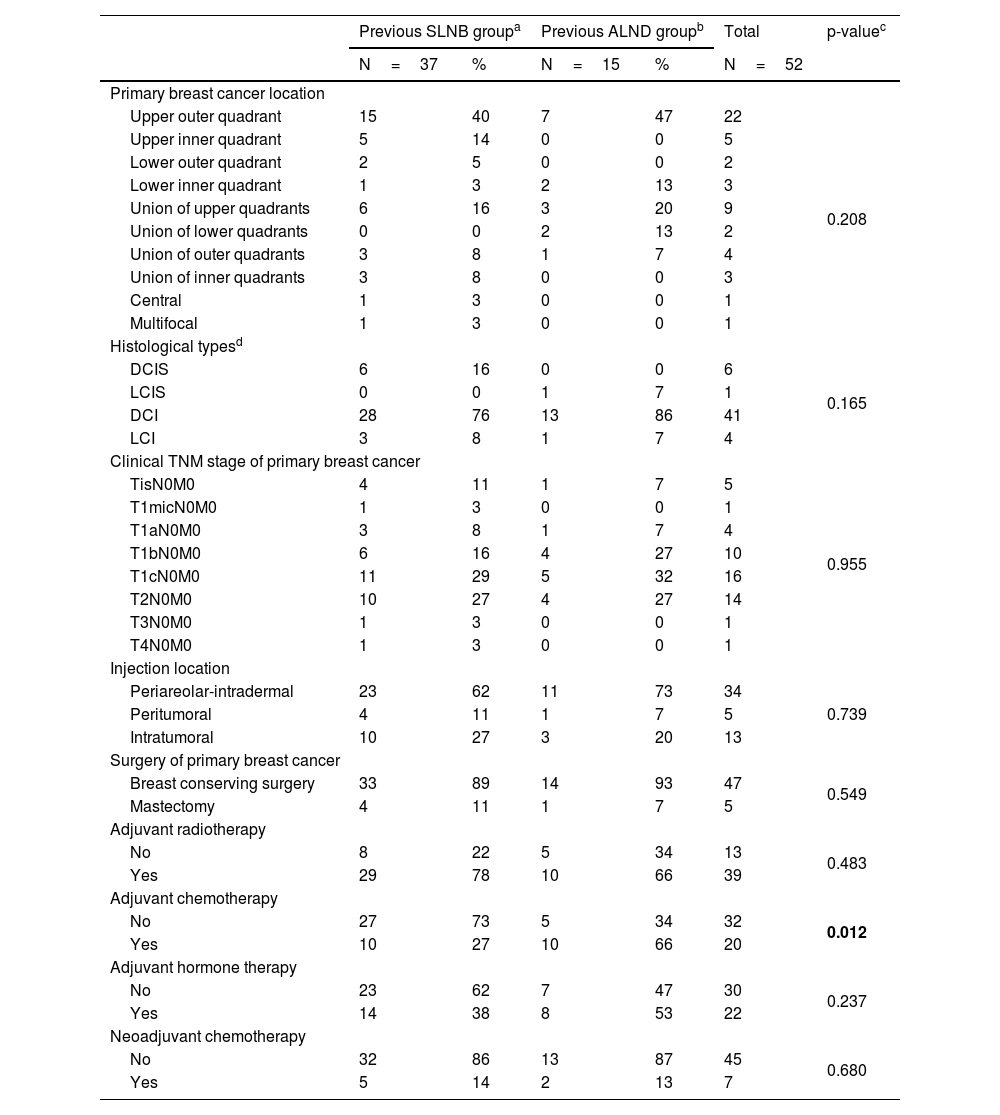
Materials and methods1102 patients were retrospectively evaluated in a tertiary hospital between 10/2018–04/2022. 52 patients with ipsilateral breast tumor recurrence who underwent rSLNB were included. Demographic data, tumor characteristics, previous treatments, drainage rates and characteristics were collected and analyzed (R statistical software).
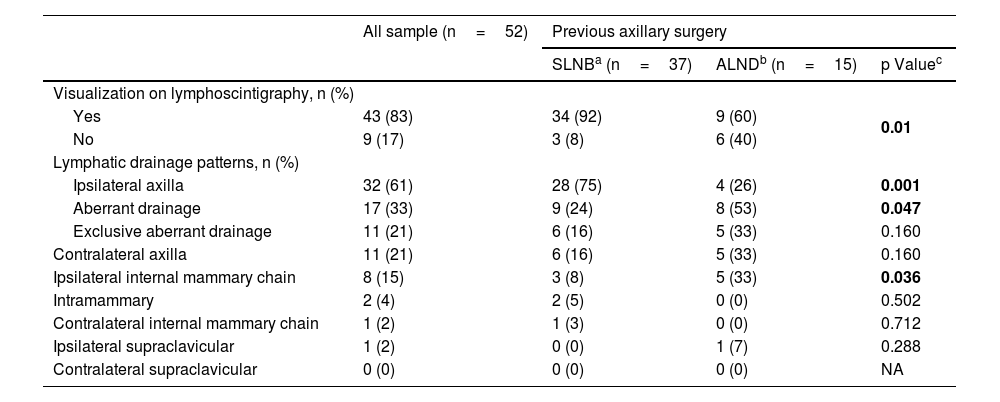
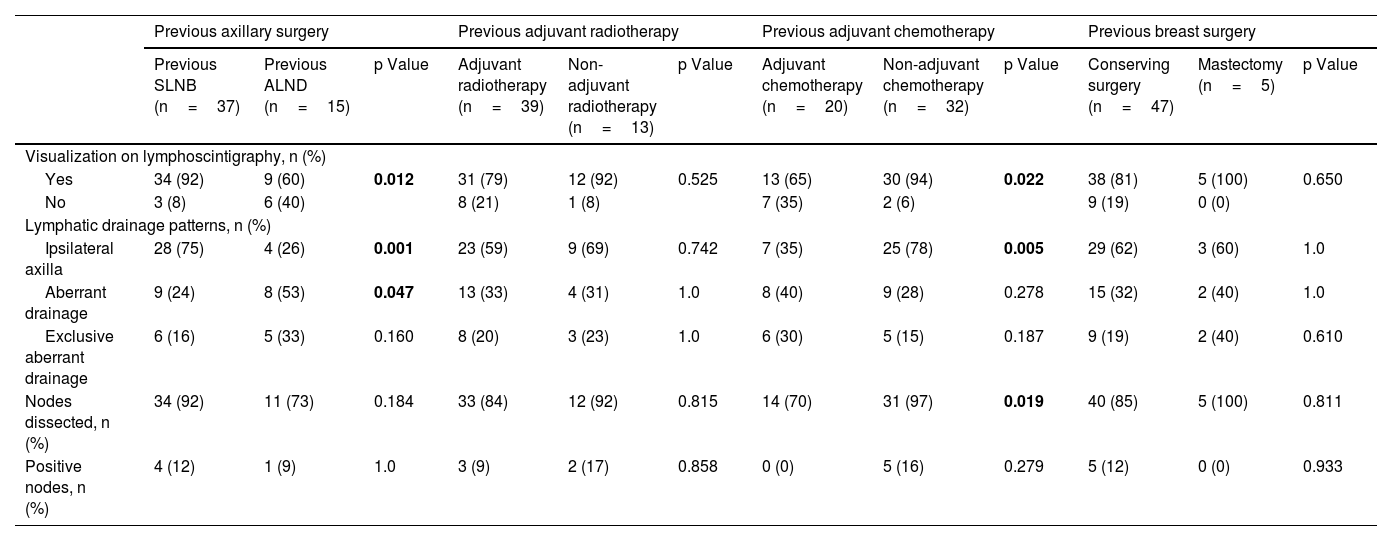
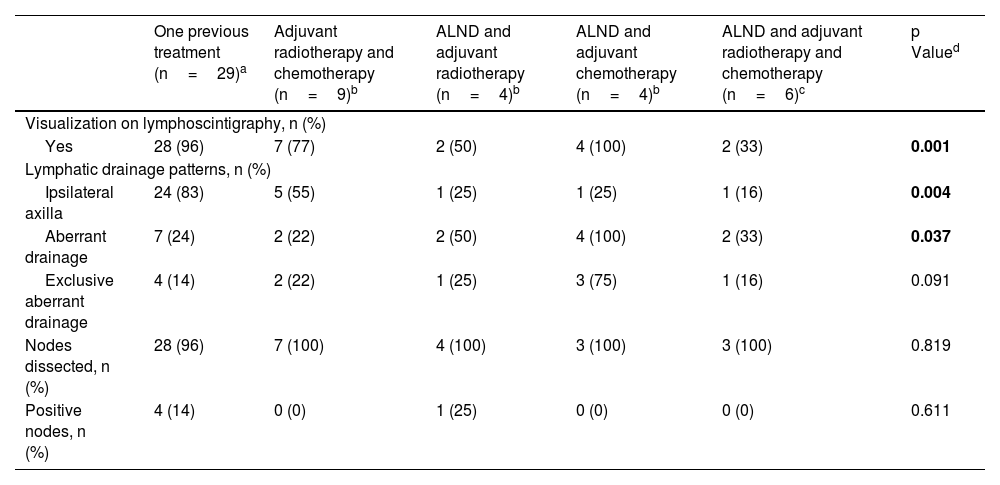
ResultsOverall drainage rate was 83%, in which excision was performed in 91%. Overall migration rate was significantly higher in patients with previous SLNB (92% vs 60%, p-value=0.012) and aberrant drainage was significantly higher in patients with previous axillar lymphadenectomy (ALND) (53% vs 24%, p-value=0.047). No statistical differences were observed in breast surgery or adjuvant radiotherapy. The percentage of positivity found was 13% (3 micrometastases and 2 macrometastases). 20% of metastases were found in aberrant drainage territories.
ConclusionsrSLNB is a feasible and applicable technique in ipsilateral breast tumor recurrence, providing key information in locorregional recurrence management. A considerable percentage of metastases are located in aberrant drainage territories, which would have been missed without rSLNB. Therefore, rSLNB is essential for a correct axillary evaluation in order to trace them.
5–10% de los pacientes con cáncer de mama presentan una recidiva local del cáncer. La ausencia de una nueva estadificación axilar podría aumentar el riesgo de recurrencia local y de mortalidad en estos pacientes. La biopsia selectiva de ganglio centinela en recurrencias (rBSGC, por sus siglas en inglés rSLNB) mediante la inyección de un radiotrazador es una opción para evaluar el estado axilar de estos pacientes. Sin embargo, han de tenerse en cuenta otros factores que pueden alterar la migración de ganglio centinela (GC), como son la cirugía axilar previa, la cirugía de mama o los tratamientos adyuvantes. Nuestro objetivo es evaluar la relación entre estos factores y la tasa de éxito de rBSGC (tasas de drenaje generales y aberrantes, tasa de metástasis).
Material y métodos1.102 pacientes fueron evaluados retrospectivamente en un hospital terciario entre el octubre de 2018 y abril de 2022. Se incluyeron 52 pacientes con recurrencia ipsilateral de cáncer de mama, que se sometieron a rBSGC. Se recopilaron y analizaron datos demográficos, características tumorales, tratamientos previos, tasas de drenaje y sus características (software estadístico R).
Resultadosla tasa de drenaje global fue del 83%, llevando a cabo la escisión ganglionar en un 91%. La tasa global de migración fue significativamente mayor en pacientes con BSGC previa (92% vs 60%, valor p=0.012) y el drenaje aberrante fue significativamente mayor en pacientes con linfadenectomía axilar previa (53% vs 24%, valor p=0.047). No se observaron diferencias estadísticamente significativas en cuanto a la cirugía de mama o la radioterapia adyuvante. El porcentaje de positividad encontrado fue del 13% (3 micrometástasis y 2 macrometástasis). Un 20% de las metástasis se encontraron en territorios de drenaje aberrantes.
ConclusionesrBSGC es una técnica aplicable en la recurrencia ipsilateral del cáncer de mama, proporcionando información clave en el manejo de la recurrencia locorregional. Un porcentaje considerable de metástasis se encuentran en territorios de drenaje aberrantes, que no se hubieran detectado de no haber realizado la rBSGC. Por lo tanto, rBSGC es esencial para una evaluación axilar correcta.
Article
If you experience access problems, you can contact the SEMNIM Technical Secretariat by email at secretaria.tecnica@semnim.es or by phone at +34 619 594 780.
Revista Española de Medicina Nuclear e Imagen Molecular (English Edition)
