









18F-Fluorine fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) imaging is considered the standard imaging modality for patients with non-small cell lung carcinoma. The aim of this study was to compare clinical staging (cTNM) performed with 18F-FDG PET/CT and surgical staging (sTNM) in patients with non-small cell carcinoma treated with surgery.
Materials and methodsWe performed a retrospective analysis of 99 surgical patients with non-small cell carcinoma who underwent 18F-FDG PET/CT examination. Semiquantitative measures were calculated from the primary lesions and mediastinal lymph nodes. Findings of cTNM were compared with final surgical–pathological evaluation. Subjects were divided into two groups as postsurgical cTNM changed and cTNM unchanged. Patients in the cTNM changed group were further classified as postsurgical upstaged (US) and downstaged (DS). Results of the US patients were compared with the results of the remaining patients consisting of cTNM unchanged and DS to evaluate the predictable roles of semiquantitative parameters for postsurgical upstaging. To determine mediastinal tumoral involvement, cut-off values were obtained from calculated semiquantitative results of FDG uptakes in lymph nodes. A p value <.05 was considered statistically significant.
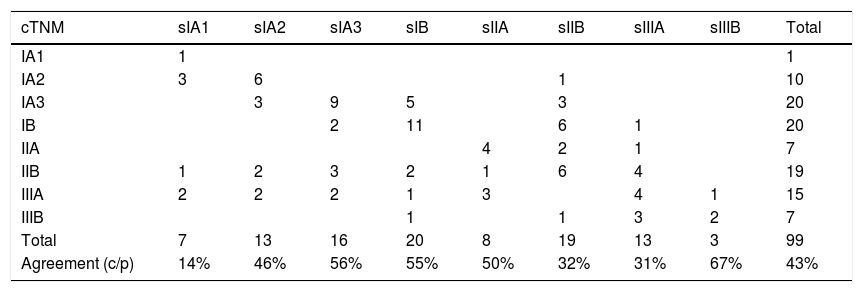
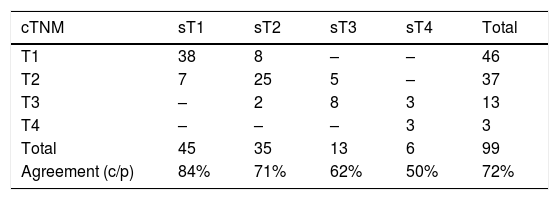
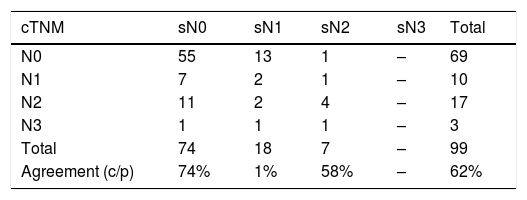
ResultsSubjects were aged 40–82 years with a mean age of 64.78±8.70 years. Classification agreement was observed in 43 patients (43%) and in 57%, postsurgical stage migration was seen. Concurrence of cTNM and sTNM was more pronounced in the T1 and N0 subsets which were 84% and 74%, respectively. The lowest concurrence was observed in N1 classification followed by T4 and N2 (1%, 50% and 58%, respectively). Change in T staging occurred in 20 of 56 (36%), in N staging 22 of 56 (39%) and change in T and N in 14 patients (25%). Distribution of US and DS patients in the cTNM changed group was, 43% (24 of 56) and 57% (32 of 56), respectively. Results of semiquantitative measures were significantly higher in US patients than the results of the group consisting of DS patients and cTNM unchanged patients, for all parameters. Cut-off value calculated from mediastinal uptakes was most specific for metastases in MTV (metabolic tumor volume) with an acceptable sensitivity (90% and 67%, respectively).
ConclusionsThe concordance between cTNM and sTNM was better in staging T category compared to N stations. Semiquantitative measures of primary tumor may play a role in predicting postsurgical upstaging. Taking MTV into consideration in the mediastinal region may be more valuable than other parameters in the assessment of nodal involvement.
La imagen de tomografía por emisión de positrones/tomografía computarizada con 18F-fluordesoxiglucosa (18F-FDG PET/TC) se considera una modalidad de imagen estándar en pacientes con carcinoma de pulmón de células no pequeñas. El objetivo de este estudio fue comparar la estadificación clínica (cTNM) realizada con 18F-FDG PET/TC y la estadificación quirúrgica (qTNM) en pacientes con carcinoma de células no pequeñas tratados con cirugía.
Material y métodosRealizamos un análisis retrospectivo de 99 pacientes con carcinoma de células no pequeñas intervenidos quirúrgicamente a los que se realizó un estudio 18F-FDG PET/TC. Se realizaron medidas semicuantitativas en las lesiones primarias y los ganglios linfáticos mediastínicos. Los hallazgos de cTNM se compararon con la evaluación quirúrgica-patológica final. Los pacientes se dividieron en dos grupos, qTNM posquirúrgico modificado y qTNM no modificado. Los pacientes en el grupo con cambio de qTNM se clasificaron adicionalmente como upstaged (US) y downstaged (DS) postquirúrgicos. Los resultados de los pacientes US se compararon con los resultados de los pacientes restantes, que consistían en qTNM sin cambios y DS, para evaluar el posible papel predictivo de los parámetros semicuantitativos en la estadificación postoperatoria. Para determinar la afectación mediastínica tumoral, se obtuvieron valores de corte de los resultados semicuantitativos de captación de FDG en los ganglios linfáticos. Un valor p <0,05 fue considerado estadísticamente significativo.
ResultadosLos pacientes tenían entre 40 y 82 años, con una edad media de 64,78 ± 8,7 años. Se observó un acuerdo de clasificación en 43 pacientes (43%), y en 57% se observó modificación en la estadificación posquirúrgica. La concurrencia de cTNM y qTNM fue más destacada en la clasificación T1 y N0, con valores de 84% y 74%, respectivamente. La concurrencia más baja se observó en la clasificación N1 seguida de T4 y N2 (1%, 50% y 58%, respectivamente). El cambio en la estadificación T ocurrió en 20 de 56 pacientes (36%); el cambio en la estadificación N, en 22 de 56 (39%); y el cambio en T y N, en 14 pacientes (25%). La distribución de pacientes de US y DS en el grupo con cambio de cTNM fue de 43% (24 de 56) y 57% (32 de 56), respectivamente. Los resultados de las medidas semicuantitativas fueron significativamente más altos en los pacientes de US que los resultados del grupo compuesto por pacientes con DS y qTNM sin cambios, para todos los parámetros. El valor de corte calculado a partir de las captaciones mediastínicas fue más específico para metástasis en el MTV (volumen metabólico tumoral) con una sensibilidad aceptable (90% y 67%, respectivamente).
ConclusionesLa concordancia entre TNM y qTNM es mejor en la clasificación de la categoría T en comparación con la categoría N. Las medidas semicuantitativas en los tumores primarios pueden jugar un papel en la predicción del US posquirúrgico. El MTV en la región mediastínica puede tener un mayor valor que otros parámetros en la evaluación de la afectación ganglionar.
Article
If you experience access problems, you can contact the SEMNIM Technical Secretariat by email at secretaria.tecnica@semnim.es or by phone at +34 619 594 780.
Revista Española de Medicina Nuclear e Imagen Molecular (English Edition)
