





The clinical information process is the basis of the doctor–patient relationship. It starts with the information provided before signing informed consent and ends on the termination of the doctor–patient relationship. The influence of demographic variables in the information process has not been thoroughly studied for inpatients undergoing surgery. In this study we aim to answer two questions: (1) Does gender have an influence on the information process for these patients? (2) Are there other factors that affect the process?
MethodA prospective study carried out using an ‘ad hoc’ designed survey on a 200-inpatient sample after undergoing surgery in the trauma and orthopaedics department of our hospital. Sampling was simple random.
ResultsWe found differences in the consistency of the answers by gender in the question regarding surgical priority, with the women having a better understanding of it (P=.04). The rest of the questions show no differences by gender. However, in the population analysed, age and educational level are the main modifiers of understanding, and they are both related to gender (P<.0001; P=.003, respectively).
ConclusionsIn clinical practice, it is fundamental to keep in mind the factors that affect the information process. According to our results, the factors that define greater vulnerability in relation to the information process are age and low educational level.
El proceso de la información clínica es el pilar de la relación médico-paciente; comienza con la información proporcionada antes de la firma del consentimiento informado y finaliza al terminar la relación médico-enfermo. La influencia de las variables demográficas en el proceso de información ha sido poco estudiada en el paciente hospitalizado intervenido quirúrgicamente. En este estudio respondemos a dos cuestiones: 1) ¿Influye el género en el proceso de información en estos pacientes? 2) ¿Existen otros factores que influyan en el mismo?
MétodoEstudio prospectivo realizado a través de un cuestionario diseñado «ad hoc» en una muestra de 200 pacientes ingresados tras la realización de una intervención quirúrgica en el servicio de Cirugía Ortopédica y Traumatología en nuestro hospital. El muestreo se ha realizado de manera aleatoria simple.
ResultadosHemos hallado diferencias en la concordancia de las respuestas por género en la pregunta sobre el tipo de prioridad de la cirugía, siendo la mujer la que mejor lo conoce (p=0.04). El resto de preguntas no muestran diferencias por género. Sin embargo, en la población analizada, son la edad y el nivel de estudios los principales factores modificadores de la comprensión, y ambos están relacionados con el género (p<0.0001; p=0.003, respectivamente).
ConclusionesEn la práctica clínica es importante tener presente aquellos factores que influyen en el proceso de información. Según nuestros resultados, los factores que definen una mayor vulnerabilidad con relación al proceso de información son la edad y el bajo nivel de estudios.
Doctor–patient communication is the basis of the doctor–patient relationship.1 The communication process is complex and continuous and involves multiple factors, and the doctor is responsible for it. It does not solely involve communicating information, as language here is used to communicate a purpose.2 This process starts with the first visit to the doctor. The patient is then informed about the surgical operation: what it consists of, possible risks, postoperative care, the foreseen result… This process does not end with the signing of the informed consent document (IC), as the process continues throughout hospitalisation, giving data on the operation, the condition of the patient and postoperative care. The communication process is cooperative.2 The concept of patient-centred care means that it is the patient himself who plays an active role in decision-making. This model is dynamic and flexible, and it involves the doctor interacting with the patient. The aim is to achieve complete and precise comprehension of the procedure, following a helicoidal model3 in which repetition and feedback are essential elements. Effective communication skills improve the doctor–patient tie, increasing the precision of diagnoses and increasing adherence to treatment and its success, while reducing disputes and improving satisfaction.3–5
In Spain, doctors are obliged by Law 41/2002, of 14 November, which is the basic law governing the independence of patients as well as rights and duties in the field of information and clinical documentation,6 to supply the necessary information prior to performing a surgical operation. However, we have found no publications that evaluate the comprehension of the information received by patients surgically operated on by the Orthopaedic Surgery and Trauma Department (OST).
The aim of our work is to answer two questions: (1) Does gender influence the process of informing hospitalised patients operated by the OST? (2) What other factors may influence this?
MethodWe carried out a prospective study by administering a questionnaire to 200 patients who had been operated on and admitted to the OST department in our hospital. The study was approved by the Research Work Evaluation Commission (CETI) of our health area. The sample size was calculated by taking the total number of patients operated in 6 months, with a confidence margin of 92%. Prior to starting the study the internal consistency of the questionnaire was validated by 60 cases, using Cronbach's alpha test, and confirming the validity of the same (Cronbach's alpha=.87). Data were gathered from September 2017 to March 2018. Simple random sampling was used.
Inclusion criteria: (1) Patients who had undergone surgery by the OST in our hospital during the study period. (2) Legally of age. (3) Surgery with hospitalisation. (4) Hospitalisation lasting longer than one day after surgery. (5) Suitable cognitive level.
Exclusion criteria: (1) Minors. (2) Patients who underwent major outpatient surgery. (3) Surgery with hospitalisation of one day or less after the operation.
Patients were verbally informed of the study objective. All of the patients took part voluntarily and signed the IC before filling out the questionnaire.
The questionnaire was designed “ad hoc” for this study. It consists of 14 questions: 6 on demographic data, 2 on diagnosis, 4 on the surgical procedure and 2 on the IC (Appendix A, supplementary material). The surveys were undertaken by a single researcher at least 2 days after surgery and during hospitalisation. The same researcher verified the answers supplied by the patients using the data shown in their clinical histories. We described it as “correct” when a patient answered a question affirmatively in a way that agreed with their clinical history; “unknown” when the patient stated that they did not know, and “error” when the patient answered a question affirmatively but when this did not agree with the clinical history data. In connection with these questions we evaluated their knowledge of the surgical procedure.
Data were analysed using the SPSS v24 statistical program. After the descriptive study of the demographic variables, the relationship between gender and the other variables was analysed using a t-test for independent samples, ANOVA for normal variables, the Chi-squared test and non-parametric tests for variables without a normal distribution. Statistical significance was set for P<.5.
The sample is composed of 200 patients, of which 91 (45.5%) are men and 109 (54.5%) are women. The average age of the men is 60.4±16 years old, while the average age of the women is 67.7±10 years old. The average number of days of hospitalisation after surgery and before the administration of the questionnaire is 3.10±1 days, with a median of 3 days and a mode of 2 days (range 2–13). Patients operated for degenerative pathology as well as trauma were included.
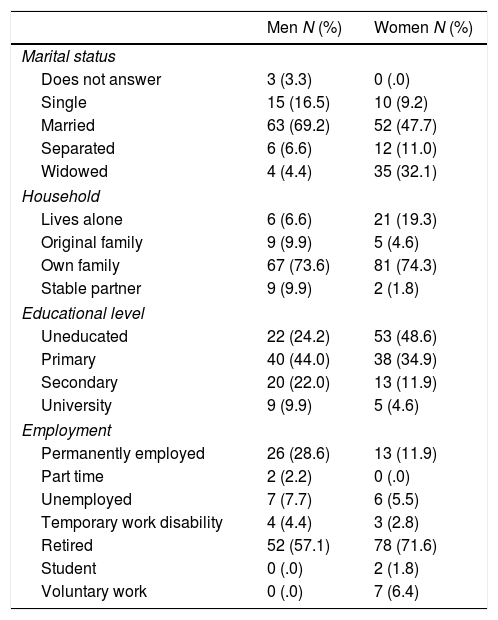
ResultsTable 1 shows the sociodemographic variables grouped according to gender.
Descriptive analysis of the demographic variables, grouped according to gender.
| Men N (%) | Women N (%) | |
|---|---|---|
| Marital status | ||
| Does not answer | 3 (3.3) | 0 (.0) |
| Single | 15 (16.5) | 10 (9.2) |
| Married | 63 (69.2) | 52 (47.7) |
| Separated | 6 (6.6) | 12 (11.0) |
| Widowed | 4 (4.4) | 35 (32.1) |
| Household | ||
| Lives alone | 6 (6.6) | 21 (19.3) |
| Original family | 9 (9.9) | 5 (4.6) |
| Own family | 67 (73.6) | 81 (74.3) |
| Stable partner | 9 (9.9) | 2 (1.8) |
| Educational level | ||
| Uneducated | 22 (24.2) | 53 (48.6) |
| Primary | 40 (44.0) | 38 (34.9) |
| Secondary | 20 (22.0) | 13 (11.9) |
| University | 9 (9.9) | 5 (4.6) |
| Employment | ||
| Permanently employed | 26 (28.6) | 13 (11.9) |
| Part time | 2 (2.2) | 0 (.0) |
| Unemployed | 7 (7.7) | 6 (5.5) |
| Temporary work disability | 4 (4.4) | 3 (2.8) |
| Retired | 52 (57.1) | 78 (71.6) |
| Student | 0 (.0) | 2 (1.8) |
| Voluntary work | 0 (.0) | 7 (6.4) |
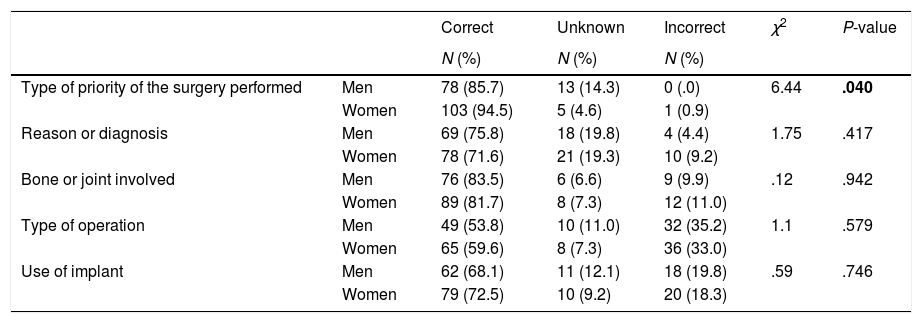
The answers to the variables that indicate knowledge according to gender are shown in Table 2. No differences according to gender were found in the correspondence of the answers to the data in the clinical histories for the following questions: reason for the operation, bones or joints operated, type of surgery performed and the use of an implant. Differences were only found in the type of priority of the surgery performed (χ2=6.4; P=.04), as the women knew more in this respect. We wish to underline that 46.2% of the men and 40.4% of the women either did not know or gave an incorrect answer to the question about the type of surgery.
Results of the concordance of the answers that indicate comprehension of the information about the surgical procedure.
| Correct | Unknown | Incorrect | χ2 | P-value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Type of priority of the surgery performed | Men | 78 (85.7) | 13 (14.3) | 0 (.0) | 6.44 | .040 |
| Women | 103 (94.5) | 5 (4.6) | 1 (0.9) | |||
| Reason or diagnosis | Men | 69 (75.8) | 18 (19.8) | 4 (4.4) | 1.75 | .417 |
| Women | 78 (71.6) | 21 (19.3) | 10 (9.2) | |||
| Bone or joint involved | Men | 76 (83.5) | 6 (6.6) | 9 (9.9) | .12 | .942 |
| Women | 89 (81.7) | 8 (7.3) | 12 (11.0) | |||
| Type of operation | Men | 49 (53.8) | 10 (11.0) | 32 (35.2) | 1.1 | .579 |
| Women | 65 (59.6) | 8 (7.3) | 36 (33.0) | |||
| Use of implant | Men | 62 (68.1) | 11 (12.1) | 18 (19.8) | .59 | .746 |
| Women | 79 (72.5) | 10 (9.2) | 20 (18.3) |
Statistically significant results are shown in bold type (P<.05).
The second factor analysed was age. Patient age is associated with the concordance of the answers to the questions about whether they knew the diagnosis and which bones or joints were involved (Pearson −0.2; P=.003 and Pearson −0.2; P=.001, respectively). The patients who knew the diagnosis had an average age of 62.8±15 years old, as opposed to those who cited an incorrect diagnosis or reason, 67.5±10 years old, and these findings are statistically significant (CI 95%: −9.8 at 0.4; P=.02). The patients who did not know the reason for the operation had an average age of 72.2±8 years old, which is higher than the other patients. The differences between the patients who knew the diagnosis and those who did not know it are also statistically significant (CI 95%: −18.1 at −1.8; P=.013).
In connection with the question about the bone or joint that was operated on, the patients who answered correctly had an average age of 63±14 years; those who did not had an average age of 68.3±5 years old, a statistically significant difference (CI 95%: −13.3 at 2.6; P=.002). The patients who did not know the name of the bone or joint involved had an average age of 73±9 years old, a statistically significant difference in comparison with those who gave a correct answer (CI 95%: −16.1 at −3.4; P=.016).
We also found a statistical association between age and gender (CI 95%: −11.2 at −3.4; P<.0001) as the women in our population are older than the men.
The third factor analysed is the educational level of the population. There is a statistically significant relationship (F=2.9; P=.037) between patients who knew their diagnosis or reason for surgery and educational level, so that the patients with the highest educational level are those who best know their diagnosis or reason for surgery. No statistical difference was found in the other questions.
Educational level is associated with gender and age in a statistically significant way. We found a higher percentage of uneducated women than we did men, and the percentage of those with university studies was twice as high in the latter (χ2=14; P=.003). The average age of the group of uneducated patients was 72±9 years old; those with primary education, 64.6±11 years old; with secondary education, 54±14 years old; and university or higher, 46.5±19 years old. Statistically significant differences were found between the uneducated patients and the other groups (CI 95%: 4 at 10.7; P=.012; CI 95%: 13.4 at 22.6; P<.0001; CI 95%: 19 at 32; P<.0001), as well as between the patients with primary education and those who had gone to university (CI 95%: 10.7 at 25.6; P=.002). No differences were found in the other associations.
Comprehension of the surgical procedure therefore rises with the increasing educational level of patients. Age and gender are factors that are associated with educational level.
Reading of the IC document may be another variable that influences comprehension of the procedure, given that it includes all of the data which were asked about in the questionnaire. Table 3 shows the results of crossing the gender variable with reading the IC. These differences are statistically significant (χ2=13.4; P=.004), and fewer women read the IC. Reading this document and comprehending it are influenced by educational level (Table 4), and there is a statistically significant relationship between both of them (χ2=47.5; P<.0001). Reading the IC is not associated with age.
Results of crossing the gender variable with reading of the IC document.
| Read IC | Yes, before signing it | Yes, after signing it | No | Does not remember | χ2 | P-value |
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |||
| Men | 20 (22.0) | 26 (28.6) | 45 (49.5) | 0 (.0) | 13.4 | .004 |
| Women | 18 (16.5) | 13 (11.9) | 75 (68.8) | 3 (2.8) |
Statistically significant results are shown in bold type (P<.05).
Results of crossing the educational level variable with reading of the IC document.
| Read IC | Yes, before signing it | Yes, after signing it | No | Does not remember | χ2 | P-value |
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |||
| Uneducated | 5 (6.7) | 6 (8.0) | 62 (82.7) | 2 (2.7) | 47.5 | .000 |
| Primary | 16 (20.5) | 19 (24.4) | 42 (53.8) | 1 (1.3) | ||
| Secondary | 10 (30.3) | 14 (42.4) | 9 (27.3) | 0 (.0) | ||
| University or higher | 7 (50.0) | 0 (0.0) | 7 (50.0) | 0 (.0) |
Statistically significant results are shown in bold type (P<.05).
Another possibly influential factor is the number of days of hospitalisation, as it seems reasonable to think that the exactitude of answers may be affected by this. However, when our data were analysed no differences were found according to the number of days between surgery and the administration of the questionnaire in the questions on whether they knew the diagnosis or reason for surgery and the bones or joints involved. Longer hospitalisation does not therefore increase the number of correct answers. Nor were there any differences in the days of hospitalisation until the administration of the questionnaire according to gender, so that days of hospitalisation are not a factor that influences the answers.
DiscussionThe factors that influence comprehension of the information hospitalised patients are given when operated on by the OST department have hardly been studied in the literature.
Our study found that women knew more about the priority of the surgical operation they had been subjected to. This may be relevant, given that surgical priority influences the prognosis, result, hospitalisation time and complications. We found no differences in comparison with men for the other questions. Although we found no other study which evaluates the same type of questions as ours, the gender variable has been studied in the literature. Guillén-Perales et al.7 evaluate the quality of the information given in the process of obtaining IC for anaesthesia in 150 oncological patients subjected to surgery, and they found no difference in the answers according to gender. The same results for gender were obtained in the study by Kadakia et al.,8 in a series of 146 orthopaedic patients operated for fractures, in which they evaluated comprehension of the procedure. Crepeau et al.9 present a sample of 98 orthopaedic patients, with no statistically significant findings in terms of gender regarding the comprehension of the process of obtaining their IC. Fink et al.,10 in a sample of 575 surgical patients in different specialities, including trauma patients, among others, evaluate comprehension of the information process and found no association with gender.
Age is another factor that has to be considered. We found that age is a factor that influences comprehension, as the older individuals were found to understand the information less well, as shown by a lower percentage of correct replies to questions about their diagnosis and the bones or joints affected. Age has been evaluated in several studies, with contradictory results. Statistical differences were found in the study by Fink et al.,10 although none were found in the studies by Guillén-Perales et al.7 and Kadakia et al.8 Unlike the finding described in the study by Crepeau et al.,9 we found that the operated women were older than the men. Age therefore varies according to gender, and this association is statistically significant. Our sample of women was older than the sample of men, and this influences the information process, indirectly leading the women to understand the information less well. This may lead us to falsely conclude that women understand the procedure less well, although as we have seen, it is patient age and not gender that influences this. Paradoxically, it was the group of women which best knew the priority of the surgery they had received.
There is greater agreement on the relationship between educational level and its influence on comprehension of the information: a higher educational level is associated with better comprehension of the information process.7–10 The relationship in our study between educational level and comprehension of the procedure, gender and age is statistically significant. We pointed out above that the oldest patients are women; in the same way, the uneducated patients were more often elderly and female. We can therefore identify a group at risk: elderly and uneducated women.
Although it is legally necessary to sign the IC document prior to a surgical operation, this does not guarantee that the surgical procedure has been understood.7,11,12 Good quality information is an indispensible requisite previous to signing the IC document.1,11 This document explains what the operation consists of, its purpose and its risks and consequences, as well as therapeutic alternatives. By signing it the patient expresses their satisfaction with the information and states that they have sufficiently understood the procedure. This study shows that this is not always the case. Signing the IC document does not mean that the procedure has been understood. Although 97% of the sample state that they signed the IC document, 9.0% did not know the priority of the surgery involved. 26.5% did not know the diagnosis, 17.5% did not know which bone or joint had been operated on, 43% did not know what type of operation had been performed and 29.5% did not know whether prosthetic or osteosynthesis material had been implanted. Gender influences the reading of the IC, as men read it more than women. Reading the IC document is not associated with age, although the average age of the patients who do so is lower than that of those who do not. There is a strong statistical association between educational level and reading the document, and the majority of the patients who read the IC document have some level of education.
The intrinsic limitations of this study design must be taken into account: it is an observational, descriptive and prospective study, in which time distortion may influence patients’ recall of information, above all in those operated after a long time in the waiting list. As this is a single hospital study it may not be possible to extrapolate the results to all of the patients operated by the OST.
To summarise, according to our results the most important factor which influences comprehension of the information about the surgical procedure is educational level. It is fundamental that patients understand the information they are given for their signing of the IC document to be valid. When informing patients it is necessary to be proactive with elderly women with a low educational level, given that their level of comprehension will be lower than that of the rest of the population.
Level of evidenceLevel of evidence II.
FundingThis research received no specific grants from public, commercial or not-for-profit bodies.
Conflict of interestsThe authors have no conflict of interests to declare.
I would like to thank the patients for their unselfish participation, as well as the collaborating authors for their invaluable help.
The following are the supplementary data to this article:
Please cite this article as: García-García EM, Sánchez-Sabater B, Medrano-Morte I, Luna-Maldonado A. Determinantes sociodemográficos de la comprensión de la información clínica en pacientes hospitalizados intervenidos de cirugía traumatológica. Rev Esp Cir Ortop Traumatol. 2019;63:355–360.
