



To evaluate the implementation of a flat panel digital radiolography (DR) system with WiFi technology in an emergency radiology area in which a computed radiography (CR) system was previously used. We analyzed aspects related to image quality, radiation dose, workflow, and ergonomics.
Material and methodsWe analyzed the results obtained with the CR and WiFi DR systems related with the quality of images analyzed in images obtained using a phantom and after radiologists’ evaluation of radiological images obtained in real patients. We also analyzed the time required for image acquisition and the workflow with the two technological systems. Finally, we analyzed the data related to the dose of radiation in patients before and after the implementation of the new equipment.
ResultsImage quality improved in both the tests carried out with a phantom and in radiological images obtained in patients, which increased from 3 to 4.5 on a 5-point scale. The average time required for image acquisition decreased by 25s per image. The flat panel required less radiation to be delivered in practically all the techniques carried out using automatic dosimetry, although statistically significant differences were found in only some of the techniques (chest, thoracic spine, and lumbar spine).
ConclusionsImplementing the WiFi DR system has brought benefits. Image quality has improved and the dose of radiation to patients has decreased. The new system also has advantages in terms of functionality, ergonomics, and performance.
Evaluar la implantación de un sistema digital de pantalla plana (flat panel digital radiography [DR]) con tecnología WiFi, en una sala de radiología de urgencias que previamente estaba trabajado con un sistema de radiología computarizada (computed radiography [CR]). Se analizaron aspectos de calidad de imagen, reducción de dosis, flujo de trabajo y ergonomía.
Material y métodosSe estudiaron los resultados obtenidos con sistemas CR y DR-WiFi, relacionados con la calidad de imagen analizada en imágenes obtenidas en maniquí y tras la valoración de imágenes radiológicas por radiólogos, también se analizaron tiempos y flujo de trabajo en la realización de los estudios con ambos métodos y especialmente se estudiaron datos de reducción de dosis en grupos de pacientes antes y después de la instalación del nuevo equipamiento.
ResultadosLa calidad de imagen mejoró tanto en las pruebas realizadas sobre maniquí como en la evaluación por radiólogos, que aumentó de 3 a 4,5 en una escala máxima de 5; los tiempos de estudio disminuyeron un promedio de 25 segundos por cada imagen; se comprobó que se requiere utilizar menos radiación con el panel plano en prácticamente todas las técnicas llevadas a cabo con exposimetría automática, aunque el estudio solo ha mostrado diferencias estadísticamente significativas en algunas de las técnicas (tórax, columna dorsal y lumbar).
ConclusionesLa instalación del sistema DR-WiFi ha sido beneficiosa. Se ha producido un incremento en la calidad de imagen con una reducción de la dosis en los pacientes, junto a ventajas en términos de funcionalidad, ergonomía y rendimiento.
The progressive incorporation of image digital systems to the Radiodiagnostic Services has given rise to a debate about the advantages and drawbacks of said systems.1–3
When planning the replacement of radiology equipment, whether analog or not, for a new, digital one, one of a more advanced technology, it is usual for issues to arise concerning the foreseeable changes in image quality, patient's doses and aspects related to ergonomics and ward efficiency.
The selection of the optimal examination techniques in digital radiology equipment is not trivial. In conventional analog systems, the reduced latitude of a given film-screen combination leaves a relatively narrow margin for choosing the optimal technique in each case. Nevertheless, digital systems allow for a wide range of variations in the techniques used for a given examination, which brings about subtle and continual modifications in the characteristics of the image, said modifications may determine their diagnostic value in ways that, on occasion, are difficult to assess.2,3
In fact, most of the times it is possible to improve image quality with digital systems by increasing the doses given to the patients and since their implantation; it may be observed that derivations to higher doses may occur in this type of systems.4,5 However, at present, the high efficiency of many detectors existing in the market makes it possible for digital radiology to reduce the patients’ doses without compromising the diagnostic value of the examinations.
With the installation of new radiological equipment, it is desirable to achieve an improvement in image quality from the point of view of their diagnostic value, a reduction in the doses given to patients or, preferably a combination of both objectives; moreover, other expected advantages refer to aspects of functionality, ergonomics and performance. In order to assess the efficaciousness of the use of wireless digital radiograph detectors, the study presented in this paper was undertaken in one of the radiology wards at our hospital.
Materials and methodsIn the Segovia Hospital's Emergency Room, the Radiodiagnostic Service has a general radiology ward consisting of a four-year-old X ray apparatus, Siemens Multix Top®, and a seven-year-old computed radiography [CR] system, AGFA ADC Compact Plus®, with phosphorus screens model MD40.
The decision was made to replace the CR, seeking a solution that would keep the X-rays ward analog. The equipment to be installed had to fulfill all the expectations for an ER radiology ward, where work is constant twenty-four/seven, with a daily average of 200 patients in different access conditions: walking, bedridden, polytraumatized, etc., it is necessary to perform examinations with bucky, directly or projections with horizontal rays.
It was imperative for it to be installed rapidly and for the radiology technicians to learn and become acquainted with it quickly, since for operative reasons concerning the services rendered, it was not possible to interrupt the ward's operations.
A flat panel direct digital system with wireless Wi-Fi technology (Wireless Fidelity, Wireless Ethernet Compatibility Alliance®) was chosen, it was supplied by Carestream Health, model DRX-1®, using two flat wireless detectors.
The DRX-1 system is compatible with any conventional radiology ward using radiograph chassis or 35cm×43cm CR, and it does not require making any modifications either in the generator, or in any other elements in the radiology ward. It consists of one or more amorphous silicon flat digital detectors, with a reception area of 2.544×3.056 pixels, each of them 139μm×139μm6 in size.
In order to undertake the study of the radiation doses on the patients, a non-systematic data collection of the images of radiologic studies was carried out before and after the new equipment was installed. The radiology technicians carried out the registration intermittently, within the availability that the heavy workload of the ER radiology ward allowed. Data on the patients’ age, sex or weight were not collected; only technical radiograph data and data on the equipment's operation were collected.
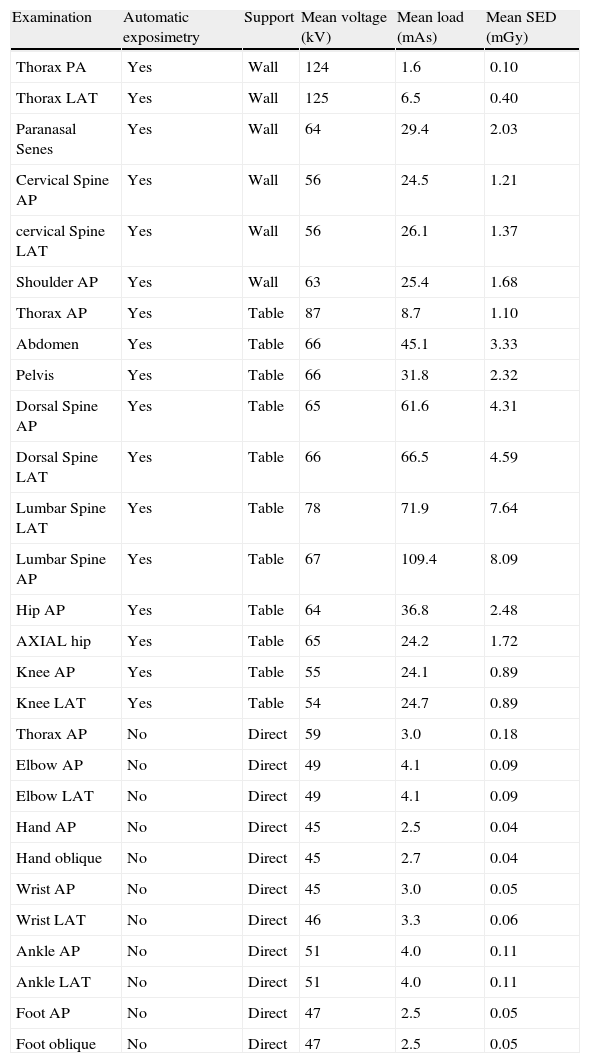
The first sample with 968 images was collected before the system's replacement, with the technical parameters used, adjustment of the Automatic Control of Exposure (ACE), the work methods and procedures of the facility's operators just like they were in that moment, with the AGFA ADC Compact Plus® system. Table 1 presents a selection of the parameters collected.
Average technical parameters used in different examinations and estimation of patient entrance dose (SED) with the CR system, with the usual work methods and procedures in the facilities until the moment they were replaced by the DRX-1 system.
| Examination | Automatic exposimetry | Support | Mean voltage (kV) | Mean load (mAs) | Mean SED (mGy) |
| Thorax PA | Yes | Wall | 124 | 1.6 | 0.10 |
| Thorax LAT | Yes | Wall | 125 | 6.5 | 0.40 |
| Paranasal Senes | Yes | Wall | 64 | 29.4 | 2.03 |
| Cervical Spine AP | Yes | Wall | 56 | 24.5 | 1.21 |
| cervical Spine LAT | Yes | Wall | 56 | 26.1 | 1.37 |
| Shoulder AP | Yes | Wall | 63 | 25.4 | 1.68 |
| Thorax AP | Yes | Table | 87 | 8.7 | 1.10 |
| Abdomen | Yes | Table | 66 | 45.1 | 3.33 |
| Pelvis | Yes | Table | 66 | 31.8 | 2.32 |
| Dorsal Spine AP | Yes | Table | 65 | 61.6 | 4.31 |
| Dorsal Spine LAT | Yes | Table | 66 | 66.5 | 4.59 |
| Lumbar Spine LAT | Yes | Table | 78 | 71.9 | 7.64 |
| Lumbar Spine AP | Yes | Table | 67 | 109.4 | 8.09 |
| Hip AP | Yes | Table | 64 | 36.8 | 2.48 |
| AXIAL hip | Yes | Table | 65 | 24.2 | 1.72 |
| Knee AP | Yes | Table | 55 | 24.1 | 0.89 |
| Knee LAT | Yes | Table | 54 | 24.7 | 0.89 |
| Thorax AP | No | Direct | 59 | 3.0 | 0.18 |
| Elbow AP | No | Direct | 49 | 4.1 | 0.09 |
| Elbow LAT | No | Direct | 49 | 4.1 | 0.09 |
| Hand AP | No | Direct | 45 | 2.5 | 0.04 |
| Hand oblique | No | Direct | 45 | 2.7 | 0.04 |
| Wrist AP | No | Direct | 45 | 3.0 | 0.05 |
| Wrist LAT | No | Direct | 46 | 3.3 | 0.06 |
| Ankle AP | No | Direct | 51 | 4.0 | 0.11 |
| Ankle LAT | No | Direct | 51 | 4.0 | 0.11 |
| Foot AP | No | Direct | 47 | 2.5 | 0.05 |
| Foot oblique | No | Direct | 47 | 2.5 | 0.05 |
AP: anteroposterior; DRX1: WIFI-flat panel digital radiography; LAT: lateral; PA: posteroanterior.
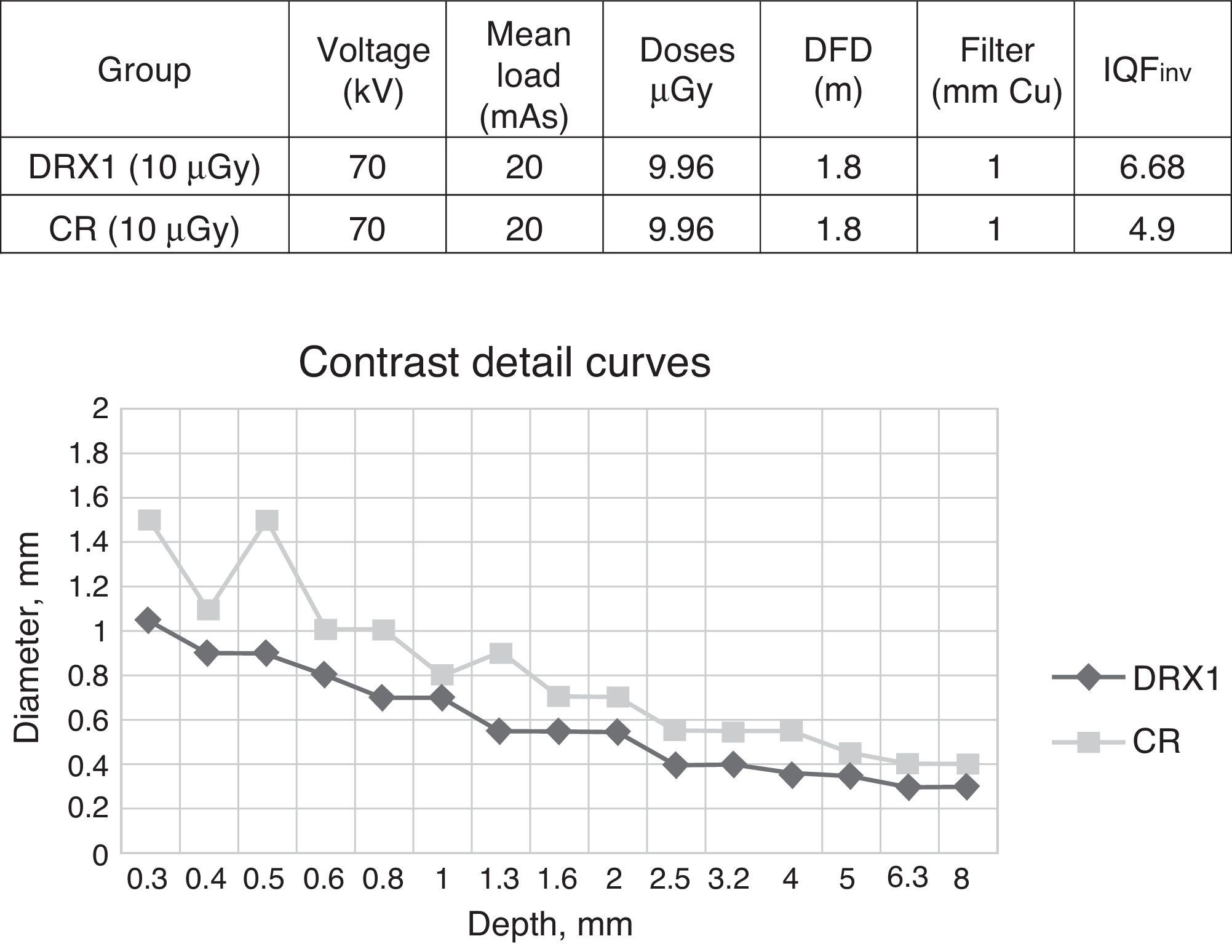
At the moment of the wireless flat panels incorporation (one on the examination table and the other on the wall), a very accurate follow-up of the operations was carried out jointly with the technical services of the suppliers of both the flat panels and the X-ray apparatus. In order to make decisions about the adjustments to be made on the ACE and the parameters of the new digital system, a contrast detail dummy CDRAD 2.0 (Artinis Medical Systems B.V.®) was used, with a 70kW voltage, filtering the radiation beam with 1mm of copper, at a distance of 1.8m, and with an appropriate technique to produce a kerma value in the air of 10μGy at the entrance of each of the detectors.
In order to compare the detectors’ technical efficiency, images were taken with the CR system used so far and with the new Wi-Fi flat panels to be used from then on. The resulting images were subjected to an automatic analysis by means of the software CDRAD Analyser,7 from which both the contrast-detail curves and the IQFinv value (inverse formula image quality index)8 corresponding to each curve were obtained.
An anthropomorphic thorax dummy was used for a preliminary adjustment of the processing software parameters of the images obtained with the flat panels. Once this first adjustment had been established, its refinement began by means of the evaluation of the clinical images by the radiologist in charge of reporting the examinations carried out in the ward. Said refinement was produced for a set of high-frequency or special interest studies (thorax, lumbar spine, abdomen, and wrist-hand).
In one final stage of the process, the ACE was adjusted. It was decided to set up the system in a way so that it would allow for a moderate reduction in patient doses, at least in some examinations, and at the same time the diagnostic quality of most images improved.
The second sample, with 1288 images, was selected from the examinations performed in the two months after substitution of the image system. The technical parameters were collected from the sample for the group of techniques indicated in Table 1.
Due to the type of samples, and because no data on age, sex, weight or other parameters were collected, the samples turned out to be asymmetric and they did not comply with the criteria for normalcy (Kolmogorov–Smirnov test, p≤0.001); that is why a non-parametric test was used for the statistical analysis: the Mann Whitney U Test.9 The statistical significance was established for a value of p<0.05.
The statistical analysis was made with the program SPSS v. 15.0; a comparison of the radiation level in examinations performed with automatic exposimetry was carried out in the two samples (with CR and DRX1), in order to assess the differences in global doses and those by specific techniques, and their statistical significance.
On the other hand, the study has attempted to quantify the possible advantages in terms of image quality appraised by radiologists, functionality and performance at the radiology emergency ward (reduction of time per examination and performance).
Evaluating the diagnostic value improvement of the images obtained after the installation of the new equipment is difficult to objectify; in order to come close to an impression that on many occasions is subjective on the part of the radiologist, a survey was conducted among 10 senior radiologists who usually report to the emergency radiology studies. In the survey they appraised radiological images, obtained both with the previous CR system and the newly installed DRX1, they were requested to compare them with the images taken with other digital equipment with fixed flat panels (flat digital panel radiography DR) installed in the Radiodiagnostic Service. Thorax, lumbar spine, abdomen and wrist-hand examinations were selected from both out patients and hospitalized patients, performed both with grill and directly. All the studies were evaluated in parallel and individually by the radiologists, who assigned to the image a diagnostic quality value in a scale of 1–5, where value 1 corresponded to poor quality and value 5 to maximum quality.
In order to assess the reduction in the time in which the images are obtained, an estimation of the mean examination times was made, in the first patient sample with the CR system, in the second with the DRX1. To this end, several clocked measurements were taken from the moment of X-ray exposure, until the image is processed and is available on the ward's control monitor.
In relation to ergonomics, in order to appreciate the advantages of the DRX1system, a non-ruled survey among the radiology technicians was conducted.
ResultsTable 1 shows a selection of the mean technical parameters used in different examinations with the CR system, with the usual work methods and procedures in the facility up to the moment of replacement for the DRX 1 system. This table also includes the estimated value for the patient's surface entrance dose (SED), estimated for each of the examinations from said parameters, from the equipment's geometric and performance values, all measured in the previous quality control verification of the X-ray emitter. It can be observed that the SED is, in all the cases, below the reference values that the Spanish legislation and the European Union establish as maximal.10
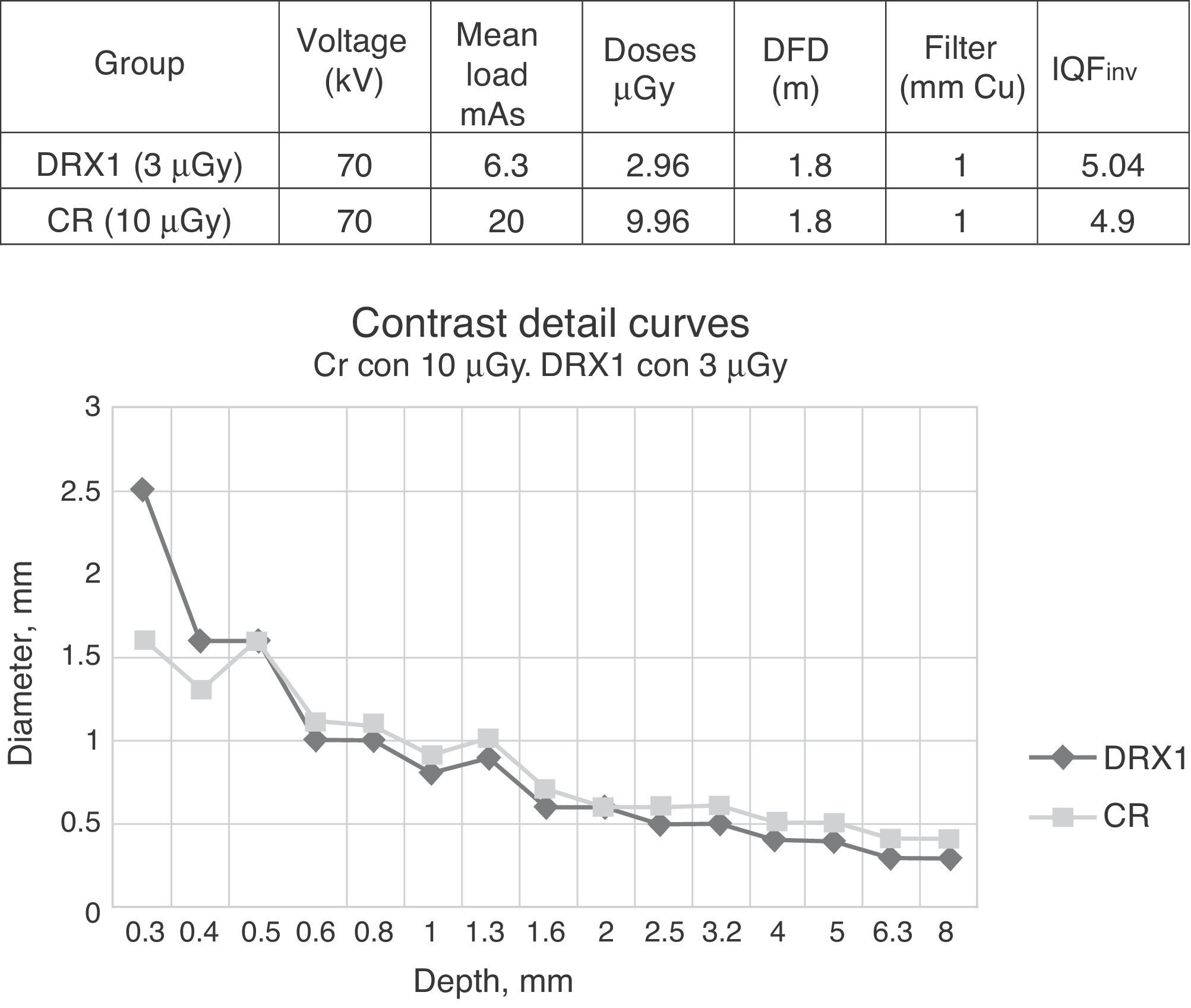
Fig. 1 shows the contrast detail curves and the IQFinv associated to each of them, the greater efficiency of the wireless flat panel analyzed causes the contrast detail curve to move down, at the same dose, or in other words, it causes the quality index IQFinv to increase. In theory, it would allow getting images of significantly greater objective quality with the same doses that were being used. As well, it would be possible to use the alternative option of maintaining quality level reducing the doses given, in order to assess it, images were taken of the CDRAD 2.0 dummy at lower doses. Fig. 2 offers a comparison of the contrast detail curves obtained with the CR system at the reference dose of 10μGy and with the wireless panel at a considerably lower dose (3μGy), and it was possible to observe a practically equal image quality in terms of contrast detail curve and quality index IQFinv, in spite of the considerable dose difference.


From the formal point of view, in terms of image in dummy, the change likewise presupposes an IQFinv index increment, an objective change that guarantees greater detectability of objects with a combination of reduced contrast and size, although it is difficult to translate that in terms of diagnostic results.
The approximation to the perception of improvement of the diagnostic value of the images was carried out by means of surveying the radiologists. For the CR system, the mean perceived image quality was three points, while with the new DRX1 system it rose to an average punctuation of 4.5 point. (The maximum value was fixed at 5 for the quality perceived in the images obtained from the fixed DR equipment that are installed in other wards of the Radiodiagnostic Service.)
Regarding the doses given to the patients, a tendency to reduction may be verified, and it is greater in certain examinations and hardly perceptible in others. It must be borne in mind that some of them are carried out by means of manual techniques, without using the automatic control of exposure (ACE); such manual techniques have not been subjected to revision.
The dose analysis was performed comparing the two samples, the first consisting of 968 radiograph images obtained with the previous CR system, and the second of 1288 images taken with the new wireless flat panel system. Analyzing all the tests performed with automatic exposimetry, flat panels present a global level of lower mean radiation (1.45mGy for DRX1; 1.53mGy for CR). However, these global differences are not statistically significant: Z=0.170; p=0.43.
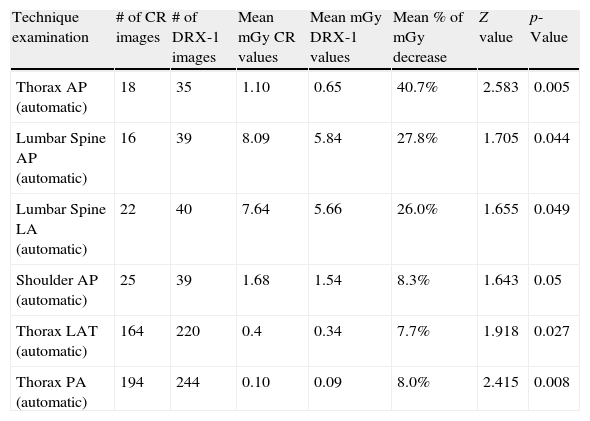
Using the same test, the radiation levels for each type of exploration was compared, and it was confirmed that there is definitely less radiation with the flat panel in practically all the techniques performed with automatic exposimetry, with statistically significant differences in several techniques, which are indicated with their values in Table 2.
Techniques which presented a statistically significant reduction in radiation in mGy with the new DRX-1 system.
| Technique examination | # of CR images | # of DRX-1 images | Mean mGy CR values | Mean mGy DRX-1 values | Mean % of mGy decrease | Z value | p-Value |
| Thorax AP (automatic) | 18 | 35 | 1.10 | 0.65 | 40.7% | 2.583 | 0.005 |
| Lumbar Spine AP (automatic) | 16 | 39 | 8.09 | 5.84 | 27.8% | 1.705 | 0.044 |
| Lumbar Spine LA (automatic) | 22 | 40 | 7.64 | 5.66 | 26.0% | 1.655 | 0.049 |
| Shoulder AP (automatic) | 25 | 39 | 1.68 | 1.54 | 8.3% | 1.643 | 0.05 |
| Thorax LAT (automatic) | 164 | 220 | 0.4 | 0.34 | 7.7% | 1.918 | 0.027 |
| Thorax PA (automatic) | 194 | 244 | 0.10 | 0.09 | 8.0% | 2.415 | 0.008 |
The techniques are shown with the number of images obtained with CR and DR, their mean radiation values in mGy and the decrease percentage attained with DRX-1.
AP: anteroposterior; CR: computed radiography; DRX1: WIFI-flat panel digital radiography; LAT: lateral; PA: posteroanterior.
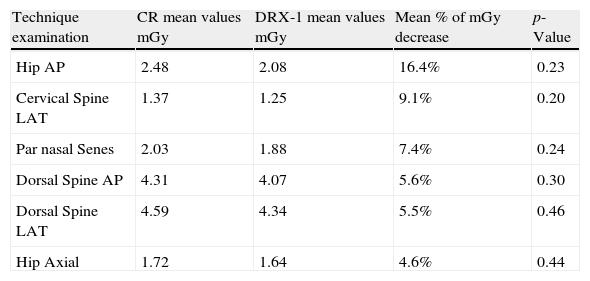
Table 3 shows the techniques with automatic exposimetry, which presented a decrease in radiation with DRX 1, although it was not statistically significant.
Techniques with automatic exposimetry which had a decrease in radiation with DRX-1, although it was not statistically significant (p>0.05).
| Technique examination | CR mean values mGy | DRX-1 mean values mGy | Mean % of mGy decrease | p-Value |
| Hip AP | 2.48 | 2.08 | 16.4% | 0.23 |
| Cervical Spine LAT | 1.37 | 1.25 | 9.1% | 0.20 |
| Par nasal Senes | 2.03 | 1.88 | 7.4% | 0.24 |
| Dorsal Spine AP | 4.31 | 4.07 | 5.6% | 0.30 |
| Dorsal Spine LAT | 4.59 | 4.34 | 5.5% | 0.46 |
| Hip Axial | 1.72 | 1.64 | 4.6% | 0.44 |
The table shows the techniques, their mean radiation values in mGy for CR and DRX1 and the percentage of decrease attained with DRX-1.
AP: anteroposterior; CR: computed radiography; DRX1: WIFI-flat panel digital radiography; LAT: lateral.
The values of time reduction in image acquisition with DRX1 as opposed to CR showed a mean decrease of 25s in obtaining every image, as a consequence of the change of their characteristics and of the change of work model between the DR and CR systems, the mobilization and transportation of the chassis were not necessary.
Regarding ergonomics, during a survey, the radiology technicians reported a marked improvement in the conditions to perform their work.
DiscussionOur study shows that, with the installation of the two wireless flat panel system, the objectives pursued were attained with a decrease of patient dose; the diagnostic quality improves, and the ward presents greater efficiency and functionality.
The results obtained and the decisions made reveal the difficulty inherent to digital systems in establishing the optimal point at which the radiologic examination techniques should be adjusted. From just the analysis of clinical images, it is very difficult to be sure how far or how close a given technique is from that hypothetical optimal point. The analyses of dummy images indeed make it possible for quality in quantitative terms to be objectified, but there remain two issues that must be figured out: on the one hand, what parameter or parameters are relevant for optimization; on the other, what degree of concordance is there between that optimization of the dummy images and those of the clinical images.
Flat panels, as opposed to CR, have a “greater detection quantum efficiency” (DQE, a parameter that combines spatial resolution and noise in the image, and provides a measure of the signal-to-noise ratio in all the frequencies that compose the image), making it possible for the patients’ doses to be reduced significantly without compromising the diagnostic value of the examinations or even improving it.11
Studies by other authors point out that the dose reduction between CR and DR may be in values of up to 50%.12 Our study has observed a decrease in radiation, both globally and separately in all the techniques, although probably some bias in the data collection and the comparison among asymmetric samples have resulted in the fact that statistic significance has only been shown in given techniques presented in Table 2.
The improvement in the working conditions of the radiology technicians and of the functionality of the ward is evident, upon establishing a new workflow and decreasing significantly the times of study in comparison with the previous CR system.13 The change of the work system is, fundamentally, in the fact that the CR chassis of every image obtained do not have to be carried to the reader installed in the control room, and at a later time it is not necessary to place another again on the wall or table chassis holder. With the wireless flat panel system, the chassis remain permanently in the chassis holders in the wards and they are removed only when their built-in battery must be changed or in order to perform direct examinations. For suitable operativeness each flat panel system has two batteries, one inserted in the panel and another as back up fully charged, this way when the system warns that the battery in use has gone dead, the technician changes the battery quickly and simply. Average run time of the batteries in full use is 6h.
It is here, in the work ergonomics department, where we consider that the wireless system is superior to other commercial options where the flat panel is joined with the ward equipment by means of systems with wires. This aspect is important in a radiology emergency room with access to bedridden and polytraumatized patients with multiple elements interfering including beds, chairs, IV drip holders, respirators, etc., a place where working “wireless” provides easier access to radiologic study in any situation (bucky, directly on the table, bed or chair, horizontal rays), without any other obstacle or limitation than the Wi-Fi coverage range, which widely covers the whole ward. The ward's functionality with the new system has maintained all its capacities and has increased its availability and performance significantly. Our observations coincide with those of other authors, who have reported a sensitive decrease in the time for obtaining images with the DRX system 114 (greater speed in the global execution of the examinations, improvement in the times of ward occupation, etc.).
The reduction of the exploration times brings about greater availability of the ward, which may increase to 35% the number of examinations performed, and thus, according to data contributed by other authors15 and business firms, present greater profitability than the installation of a CR and make up for the price difference, which is higher for DR systems; but that is not this paper's objective. In our case, since it is an installation in a radiology emergency room, the number of patients assisted is not a variable of its own; however, the greater availability of the ward has made it possible for us to examine with it bedridden inpatients who were heretofore examined in other radiology wards.
The positive impact of the installation of the DRX1 system must be appraised in all respects, in addition to the ones studied concerning the improvement in diagnostic image quality and radiation decrease for the patients. We must take into account other aspects such as the radiology ward's performance and efficiency, the improvement of the operators’ working conditions and the significant improvement for the patients with conditions that require urgent examination which are diagnosed in a faster, more reliable way.
As a whole, from the information collected in the study, it is deduced that an increase in image quality has been obtained along with a moderate reduction in the patients’ doses. We must add the advantages obtained in terms of ward functionality, ergonomics and performance, which is why we conclude that the decision of installing a wireless flat panel system in the radiology emergency room has been beneficial.
Authorship- 1.
Person responsible for the study's integrity: FJRR
- 2.
Conception of the study: MGB, FJRR, IHG
- 3.
The study's design: MGB, MAO, FJRR, RTC, IHG
- 4.
Data acquisition: MGB, MAO
- 5.
Data analysis and interpretation: MGB, MAO, FJRR, RTC, IHG
- 6.
Statistic treatment: MGB, RTC
- 7.
Bibliographic search: MGB, MAO, FJRR, RTC, IHG
- 8.
Writing of the paper: MGB, FJRR, IHG
- 9.
Critical revision of the manuscript with intellectually relevant contributions: MGB, MAO, FJRR, RTC, IHG
- 10.
Approval of the final version: MGB, MAO, FJRR, RTC, IHG
The authors declare that they do not have any conflicts of interests.
We are grateful to D. José Manuel García de Cecilia, Tutor-consulter of Statistics, SPSS and Methodology of healthcare sciences research, for his help in this paper's statistical treatment.
Please cite this article as: Garrido Blázquez M., et al. Detectores radiográficos digitales inalámbricos en una sala de radiología de urgencias. Una solución eficaz. Radiología. 2013;55:239–46.

