



To compare the methods of right ventricle segmentation in the short-axis and 4-chamber planes in cardiac magnetic resonance imaging and to correlate the findings with those of the tricuspid annular plane systolic excursion (TAPSE) method in echocardiography.
Materials and methodsWe used a 1.5T MRI scanner to study 26 patients with diverse cardiovascular diseases. In all MRI studies, we obtained cine-mode images from the base to the apex in both the short-axis and 4-chamber planes using steady-state free precession sequences and 6mm thick slices. In all patients, we quantified the end-diastolic volume, end-systolic volume, and the ejection fraction of the right ventricle. On the same day as the cardiac magnetic resonance imaging study, 14 patients also underwent echocardiography with TAPSE calculation of right ventricular function.
ResultsNo statistically significant differences were found in the volumes and function of the right ventricle calculated using the 2 segmentation methods. The correlation between the volume estimations by the two segmentation methods was excellent (r=0.95); the correlation for the ejection fraction was slightly lower (r=0.8). The correlation between the cardiac magnetic resonance imaging estimate of right ventricular ejection fraction and TAPSE was very low (r=0.2, P<.01).
ConclusionBoth ventricular segmentation methods quantify right ventricular function adequately. The correlation with the echocardiographic method is low.
Comparar los métodos de segmentación del ventrículo derecho en los planos eje corto y 4 cámaras, en los estudios de resonancia magnética cardíaca, y realizar una correlación con el método ecocardiográfico tricuspid annular plane systolic excursion (TAPSE).
Material y métodosSe estudiaron 26 pacientes con diversas enfermedades cardiovasculares con un equipo de resonancia magnética de 1,5T. Se adquirieron en todos los estudios imágenes en modo cine en eje corto y en 4 cámaras (steady-state free precession, 6mm de grosor de corte, desde la base al ápex ventricular). En todos los pacientes se cuantificaron los volúmenes telediastólico, telesistólico y la fracción de eyección del ventrículo derecho. A 14 pacientes se les practicó también una ecocardiografía y se calculó la función ventricular derecha (TAPSE), el mismo día que se realizó el estudio de resonancia magnética cardíaca.
ResultadosNo hubo diferencias estadísticamente significativas en los volúmenes y la función del ventrículo derecho determinados con los 2 métodos de segmentación. La correlación al estimar los volúmenes fue excelente (r>0,95) y disminuyó levemente para la fracción de eyección (r>0,84). La correlación entre fracción de eyección del ventrículo derecho y TAPSE fue muy baja (r=0,2; p<0,01).
ConclusiónAmbos métodos de segmentación ventricular cuantifican adecuadamente la función del ventrículo derecho. La correlación con el método ecocardiográfico es discreta.
The cardiac magnetic resonance (CMR) with gradient echo sequence in steady-state free precession (SSFP) is becoming more and more the most highly reproducible and precise image modality for the study of the anatomy of the heart. Also the CMR gives us quantitative information both on the size and ventricular function and on the blood flow as well as valuable data on the myocardium and segmental contractility. For all these reasons it is an essential image modality in patients with diseased ventricles. As a matter of fact there is general consensus on its clinical utility and study method.1–5 In the standard CMR the analysis of the left ventricular function is very important since it is a powerful diagnostic and prognostic measure of various heart conditions. But also the analysis of volume and right ventricular function is important especially for the clinical follow-up of patients with congenital heart diseases.6
Both the quantification of volume and the left ventricular function are based on the short-axis “piling”1–5 yet it remains unclear if this is the best tool for the right ventricle. The function of the right ventricle has always been harder to evaluate6–8 and according to some authors the images of the short-axis can be less reproducible.6 To solve this problem the 4-chamber plane and the cross reference or 4-chamber biplanar correspondence has been suggested as possible alternatives–all of them determining more easily the planes of the mitral and tricuspid valves.9–11 The goal of this study is to compare the segmentation of the right ventricle in the short-axis plane and 4-chambers through CMR images and then correlate the results with those of the tricuspid annular plane systolic excursion (TAPSE) echocardiography.
Materials and methodsPatientsThe study population was 26 consecutive patients (3 women between 40 and 61 years old with an average age of 49 years old; 23 men between 40 and 61 years old in between 19 and 75 years old with an average age of 51 years old). Twenty (20) patients had been referred to undergo one CMR for several clinical reasons: 6 due to myocardial infarction; 2 due to possible myocarditis; 7 due to cardiomyopathies (4 dilated cardiomyopathies, 1 hypertrophic cardiomyopathies, 2 non-compaction cardiomyopathies) and 5 due repaired Fallot's tetralogy and pulmonary regurgitation. In the remaining 6 patients the goal of the study was discarding one arrhythmogenic dysplasia of the right ventricle in 3 patients (one of them tested positive), in 2 patients with suspicion of apical thrombus and in one patient with suspicion of Tako-Tsubo syndrome. All patients gave their prior written informed consent before the test. The ethical committee approved the study protocol. Given the characteristics of the design this is a transversal study for the comparison of 2 methods.
TechniqueStudies were performed with a 1.5T magnetic resonance system with a 30mT/m maximum gradient and 125T/m/s slew rate (Magnetom Symphony Quantum; Siemens Medical Systems, Erlangen, Germany). One 4-channel phased array antenna was used too.
The study protocol consisted of balanced cardiac SSFP gradient echo cine (GRE) images. Images were acquired in apnea at the end of aspiration in the vertical long axis, 4-chamber planes and short axis plane these last 2 were used to quantify cardiac function. Other CMR routine sequences (and planes) were also obtained–adequate for every clinical indication. The patient was in the decubitus supinus position. In all studies we did between 10 and 14 cuts in the short-axis and 4-chamber planes. One 156×192 matrix was used and 25 different phases for each cut were estimated. Cutting thickness 6mm; TR 4.26ms; TE 1.3ms; flip angle 60. Apnea time of each cut was between 10 and 12s. All cases were of an adequate quality so the segmentation of the right ventricle was technically feasible.
Fourteen patients also underwent one ultrasound the very same day of the CMR study. For the study of the right ventricular function the systolic displacement analysis from the tricuspid annular plane systolic excursion (TAPSE) was used. One ultrasound expert with 14 years of experience (AM) was collecting all data.
The following parameters were quantified for the right ventricle: telediastolic volume (TDV), telesystolic volume (TSV), and ejection fraction (EF). The estimates were performed from balanced SSFP GRE images both at the short-axis and 4-chamber planes. The volumes of all cuts from the right and left ventricles were added up both in the phase of greater relaxation and in the phase of greater concentration to obtain the TDV and TSV, respectively (Simpson method). The EF was estimated in percentage (%) as (TDV−TSV)×100/TDV.
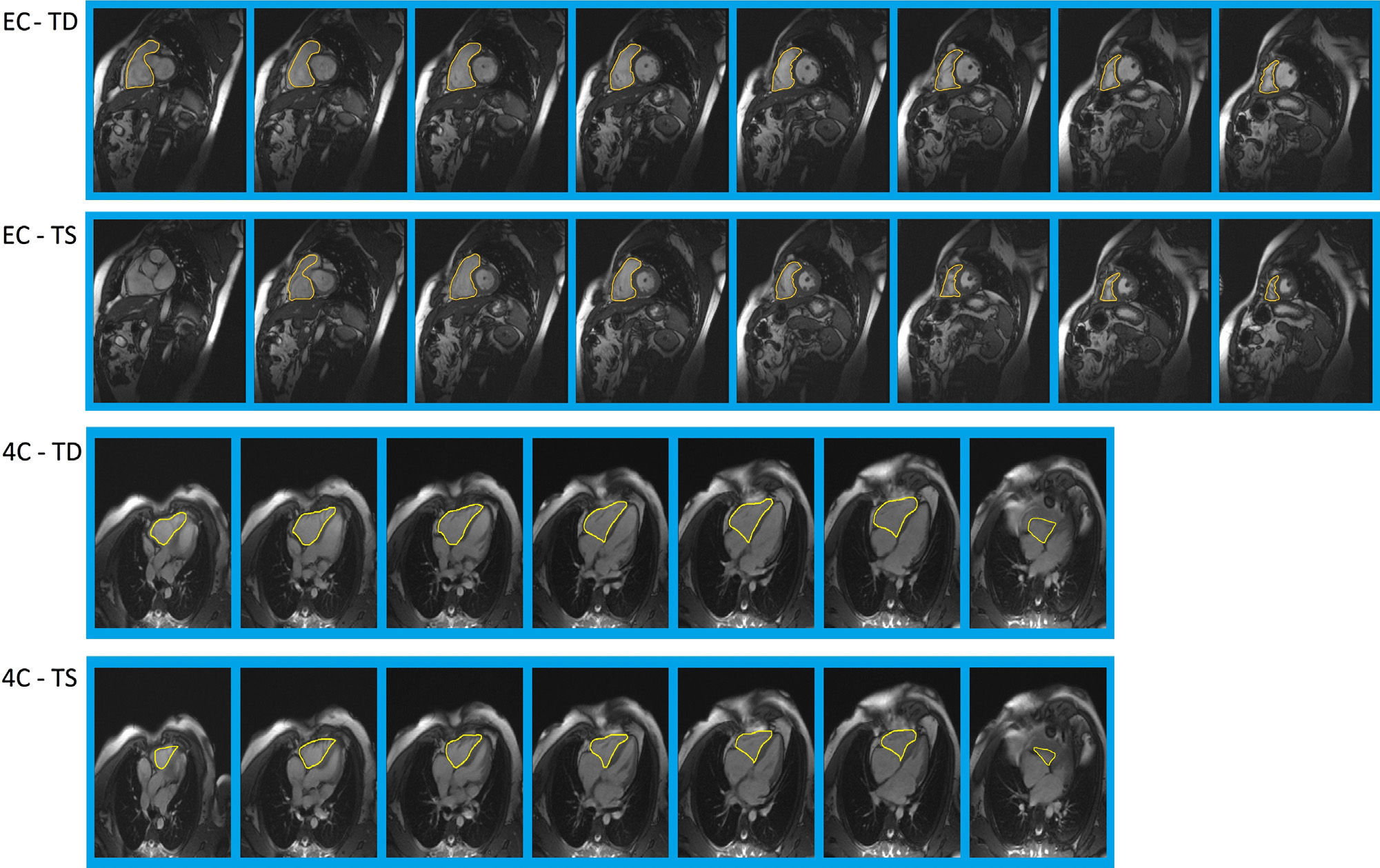
To draw the edges of the right ventricle (Fig. 1) the basal cuts proximal to the valve plane precluded the right atrium were thoroughly reviewed. The papillary and trabecular muscles were considered part of the ventricular volumes. The trabeculations of the right ventricle were included in the estimates of volumes and EF in both planes, the short-axis or 4-chambers to reduce the inter-operator variability. We paid special attention to the complete inclusion of the outflow tract.12,13
 and 4-chambers (down). In each and every one of the 2 planes we need to pay special attention to one fundamental issue: in the short-axis the exact identification of the valvular plane, and in the 4-chamber plane the complete inclusion of the arterial cone (outflow tract). SSFP sequence: steady-state free precession; TD: telediastole; TS: telesystole.")
Definition of endocardial edges for the right ventricle in the short-axis (up) and 4-chambers (down). In each and every one of the 2 planes we need to pay special attention to one fundamental issue: in the short-axis the exact identification of the valvular plane, and in the 4-chamber plane the complete inclusion of the arterial cone (outflow tract). SSFP sequence: steady-state free precession; TD: telediastole; TS: telesystole.
The analysis of ventricular function was carried out in an outside working station (Leonardo, Siemens Medical Solutions, Erlangen, Germany) equipped with a software package for the post-processing of acquired images in CMR studies (Argus, Syngo, Siemens Medical Solutions, Erlangen, Germany). To that end we based ourselves on the manual drawing of ventricular edges–the method considered to be the reference standard in the actual clinical practice. The end of TDV and TSV was visually established in cine images both in the short-axis and the 4-chamber planes by identifying the images from the maximum diastolic relaxation and the maximum systolic contraction. Ventricular edges were manually drawn in one medial telediastolic image and spread throughout the remaining telediastolic images of the ventricular apex base. Once corrected by the user the resulting edges were spread from the telediastole to the telesystole and corrected again if necessary. One operator (MS) with a 6-year experience in CMR was in charge of collecting data.
Statistical analysisThe assessed parameters are introduced as the average±standard deviation. The normal distribution of data was confirmed through the Kolmogorov–Smirnov test and the Student's t test for paired samples to study the differences among the results obtained through both methods. The confidence interval was defined in 95% of cases and the p values ≤0.05 were considered statistically significant. For the analysis of linear correlation the Pearson correlation test was used. As for the analysis of concordance between both methods the method proposed by Bland and Altman14 was used.
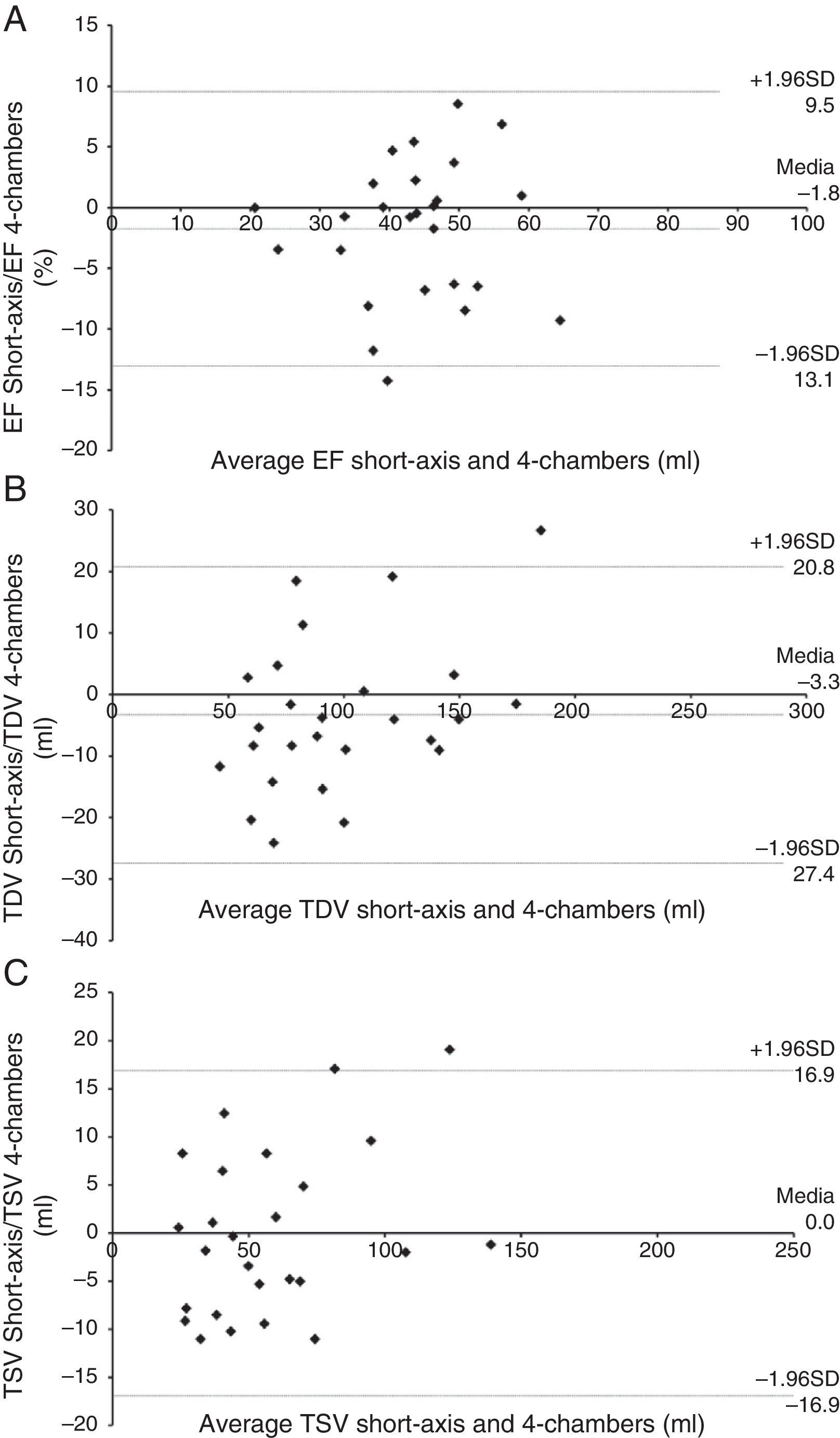
ResultsThere were no statistically significant differences in the parameters of the right ventricular function quantified in the short axis plan and the 4-chamber plane (Table 1). The correlation between both planes when assessing the TDV and TSV was excellent (r>0.95 in both cases) and went down slightly in the case of ventricular function (r>0.84) (Fig. 2). The average difference in the values of the ventricular function parameters obtained through the methods of segmentation in the short-axis plane and the 4-chamber plane was −1.8±5.8% for the EF; −3.3±12.3 for the TDV; 0.0±8.6 for the TSV. The correlation between the FE of tright ventricle and TAPSE was modest (r=0.2; p<0.01).
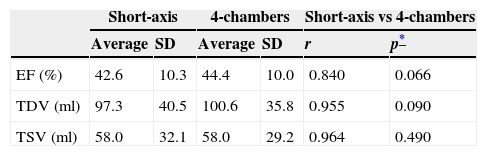
Quantification of parameters of the right ventricular function based on segmentation methods in 4-chambers and short-axis.
| Short-axis | 4-chambers | Short-axis vs 4-chambers | ||||
|---|---|---|---|---|---|---|
| Average | SD | Average | SD | r | p* | |
| EF (%) | 42.6 | 10.3 | 44.4 | 10.0 | 0.840 | 0.066 |
| TDV (ml) | 97.3 | 40.5 | 100.6 | 35.8 | 0.955 | 0.090 |
| TSV (ml) | 58.0 | 32.1 | 58.0 | 29.2 | 0.964 | 0.490 |
SD: standard deviation; EF (%): ejection fraction in percentage; TDV (ml): telediastolic volume in mililiters; TSV (ml): telesystolic volume in mililiters; r: Pearson correlation coefficient.
 Ejection fraction (EF). (B) Telediastolic volume (TDV). C) Telesystolic volume (TSV).")
Our results show that the RF and the right ventricle volumes–both in cases with normal and dilated ventricles can be correct and precisely assessed using the segmentation both in the short axis and in the 4-chamber plane.
The assessment of ventricular function and in particular of the right ventricular function is very important in congenital cardiac malformations and acquired conditions and has a decisive prognostic value in patients undergoing Fallot's tetralogy, transposition of large arteries and pulmonary hypertension.7,9,15 This is why a quick, reproducible, non-invasive method to quantify the right ventricular function is of great clinical use.16,17
The ultrasound allows us to adequately determine the EF of the left ventricle.18 However there is not an appropriate echocardiographic method to assess the right ventricular function19–21 since its geometric characteristics make this hard to happen.
Several volumetric methods have been described to quantify the right ventricle systolic function. The most widely used measurement that can be quantified as the index of the right ventricle systolic function is TAPSE in the 4-chamber apical plane that in normal conditions needs to be over 2cm. It is an overall function measurement highly dependent on the loading conditions. Other parameters used are the tricuspid ring S’ speed established by tissue Doppler which is a highly reproducible parameter not as influenced by loading conditions; the Tei index or myocardial performance index used to identify the exact start of isovolumetric contraction; and the strain or degree of myocardial deformity that can be measured in different spatial orientations (longitudinal, transversal or circumferencial). However measuring the ventricular function through CMR is still considered to be the standard of reference both for the right and left ventricles.7,20
This study focused on the comparison of 2 methods of segmentation of the right ventricle in the short-axis and 4-chamber planes in CMR studies. In our study the EF calculated in the short-axis was slightly lower than that obtained through segmentation in 4-chambers. However the outcomes were not statistically significant. In the study sample the segmentation of the short-axis usually underestimated telediastolic volumes (18 out of 26 patients) and consequently also the EF. These non-significant differences can be due to the fact that–as it also happens in other studies the effect of partial volume and the difficulty to analyze the more basal cuttings through CMR might have promoted the involuntary exclusion of a small ventricle portion in the short-axis segmentation. The difficulty to outline the valve level in the short-axis10,16 is well-known. Another factor that should be taken into account in this case in the assessment of telesystolic volume in both planes is the trabeculations of the right ventricle that are more prominent during the systole and can make the identification of the endocardial edge difficult to achieve. These are very important matters not only due to the morphological characteristics of the right ventricle highly trabeculated but also to the effects of partial volume which poses problems like the definition of the sector that needs to be included in the study of more basal and apical cuts. The inclusion or exclusion of basal cuts in the short-axis is very interesting since the atrial volume can be included by mistake.
When data from our study are compared to those of other authors we need to highlight here that some of our cases correspond with pathologic ventricles even though patients with a normal right ventricle and conditions in both ventricles have also been included especially patients with corrected Fallot's tetralogy and pulmonary regurgitation which might have biased our study. Alfakih et al.6 compared the axial and short-axis planes and established that volumes derived from axial cuts were inferior to the short-axis (in particular the telediastolic volume was 4.8% lower). For these authors the values assessed in the axial plane were more reproducible than those of the short-axis and consequently recommended the axial plane to assess the right ventricular function. Mooij et al.10 studied patients with right ventricle conditions being the reproducibility of results derived from the segmentation of the short-axis good. These authors used the biplanar cross-reference to determine the basal planes included in the analysis. Cross-reference or biplanar correspondence, 4-chambers-short axis have been proposed as an alternative to better determine the mitral and tricuspid valve-planes and solve the problem of the inclusion of the atrium by mistake.9,10 This formula seems plausible and will be studied in future research.
This study has several limitations. In particular the small population of the study. We need to test these segmentation techniques in a larger amount of patients. It would be interesting to study the right ventricular function in the short-axis and the 4-chambers in the overall population, in more patients and in different types of cardiovascular conditions. In particular it would be interesting to study those patients operated for the correction of Fallot's tetralogy and pulmonary regurgitation.22 On the other hand one inter-observer variability analysis has not been carried out here. Even though that was not the main goal of our study it is important to study the reproducibility of these techniques applied to the right ventricle since not very many studies have done so. Given the complexity of the manual drawing of ventricular edges, multiplanar segmentation and the anatomical characteristics of the right ventricle, the drawing of ventricular edges was supervised and agreed on by the authors¿ multidisciplinary team and if anything always including one radiologist, the participating cardiologist and one physicist or computer expert–all of them with years of experience in ventricular segmentation through CMR. This alleviates in part the fact of not including one variability study that we will include in a future study specifically designed to that end.
In sum our results show that both the short-axis and the 4-chamber planes are appropriate for the right ventricle segmentation and the study of its function. The correlation of the parameters obtained with both planes is good. The 4-chamber plane is a useful alternative to the short-axis plane in patients whose more basal cuts might be hard to analyze. The correlation between the right ventricle EF and TAPSE was a discrete one.
Ethical responsibilitiesProtection of humans and animalsAuthors confirm that all proceedings and experiments followed relate to the committee of responsible human experimentation ethical rules and regulations in compliance with the World Medical Association and the Declaration of Helsinki.
Data confidentialityAuthors confirm that the protocols of their centers have been followed on matters concerning the publishing of data from patients. They also confirm that all patients included in this study have been given enough information and handed over their written informed consent for their participation in this study.
Right to privacy and informed consentAuthors confirm that they have obtained the written informed prior consent from patients and/or subjects appearing in this article. This document is in the possession of the corresponding author.
Author contributions- 1.
Manager of the integrity of the study: MSB.
- 2.
Original idea of the study: MSB, LMC, CRP, JCV.
- 3.
Study design: MSB, LMC, CRP, JSC, AMM, MCP, JVC.
- 4.
Data mining: MSB, LMC, CRP, MCP.
- 5.
Data analysis and interpretation: MCP, LMC, JSC, JVC.
- 6.
Statistical analysis: MCP.
- 7.
Reference search: MSB, LMC, AMM, MCP.
- 8.
Writing: MSB, LMC, CRP, AMM, MCP, JCV.
- 9.
Manuscript critical review with intellectually relevant contributions: JSC, JCV.
- 10.
Final version approval: All authors.
Study sponsored in part by: Xunta de Galicia (file # PGIDIT06BTF20802PR).
Conflict of interestAuthors have no conflict of interest whatsoever.
Please cite this article as: Souto Bayarri M, Masip Capdevila L, Remuiñan Pereira C, Suárez-Cuenca JJ, Martínez Monzonís A, Couto Pérez MI, et al. Análisis de la función ventricular derecha en resonancia magnética cardíaca. Comparación de la cuantificación en los planos eje corto y 4 cámaras. Radiología. 2015;57:50–55.

