




Epidemiological studies on acute transverse myelitis (ATM) in South America are scarce. The aim of our study was to describe demographic, clinical and para-clinical features of patients with ATM in a health care organisation in Buenos Aires. A further objective was to determine the aetiologies of ATM.
MethodsAll patients diagnosed with ATM between June 1, 2002 and June 30, 2010 were retrospectively identified, using the Transverse Myelitis Consortium Working Group (TMCWG) criteria.
ResultsA total of 40 patients diagnosed with ATM (24 females, 60%) were included. The mean follow-up was 57±8 months. The principal cause of myelitis found was ATM secondary to demyelinating disease (55%). Idiopathic ATM was diagnosed in 15 (37.5%) cases in the sample. The majority of patients had an extensive cord lesion (50%) detectable with spinal MRI.
ConclusionThere are few epidemiological studies concerning ATM in Argentina, and we believe that it is important to be aware of the manner in which this condition manifests itself in this region. We would therefore be able to compare them with studies previously published in other countries.
Existen escasos estudios epidemiológicos sobre mielitis transversa aguda (MTA) en Sudamérica. El objetivo de nuestro estudio fue describir las características clínicas, paraclínicas y demográficas de pacientes con MTA en un centro de salud de Buenos Aires, Argentina. Además, se determinaron las diferentes etiologías asociadas a MTA.
MétodosTodos los pacientes con diagnóstico de MTA entre el 1 de junio del 2002 y el 30 de junio del 2010 fueron identificados retrospectivamente, utilizando los criterios del The Transverse Myelitis Consortium Working Group.
ResultadosSe incluyó a un total de 40 pacientes con diagnóstico de MTA, de los cuales el 60% (n = 24) fueron mujeres. El tiempo medio de seguimiento fue de 57 ± 8 meses. La principal causa de MTA fue la secundaria a enfermedad desmielinizante (55%). La MTA idiopática se presentó en el 37,5% de los pacientes. La mayor parte de los casos se presentaron con mielitis longitudinal extensa en la RM (50%).
ConclusiónConsideramos que es necesario conocer la manera en la cual esta entidad neurológica se presenta en nuestra región y de esta manera poder comparar nuestros resultados con los previamente publicados en otros países. Además, debido a las implicaciones terapéuticas, consideramos que es de suma importancia realizar una exhaustiva evaluación etiológica para diferenciar las diferentes posibles enfermedades asociadas a la MTA.
ATM is a neurological disorder involving focal inflammation of the spinal cord which may have different aetiologies. It forms part of a subgroup of acute myelopathies for which inflammation within the spinal cord is an essential factor for diagnosis.1 The estimated incidence rate of the disorder is 1 to 4 new cases per million inhabitants, it affects individuals of all ages, and it is a major cause of disability around the world.2 Clinically, ATM is characterised by acute onset of motor and sensory symptoms with spinal cord-like distribution, usually associated with bladder dysfunction. Approximately 50% of patients with this condition are unable to walk upon reaching their maximum level of disability,3 and a third recover poorly and remain severely disabled.4
In 2002, the Transverse Myelitis Consortium Working Group (TMCWG) proposed a series of diagnostic criteria for idiopathic ATM and ATM secondary to or associated with a specific disease.2 These criteria have allowed us to harmonise classifications and ensure use of standard language in clinical practice. They also serve as guidelines for recognising cases of inflammatory myelitis for inclusion in studies.
Systematic and complete evaluation in a patient with acute inflammatory myelopathy will help minimise the possibility of diagnostic errors and delays in starting treatment that may affect clinical recovery and prognoses over both the long and short term.
Despite ATM's clinical and epidemiological relevance, the best currently available sources of information on the general characteristics of this syndrome are international studies.3,5–7 Few studies examine the way this disease presents in South America.
The purpose of this study is to describe demographic, clinical, and paraclinical characteristics of patients with ATM evaluated in a full-coverage health system in Buenos Aires, the largest urban centre in Argentina. Our objective was to determine the different aetiologies of ATM and distinguish between idiopathic and secondary disease by using TMCWG criteria.
Patients and methodsParticipantsAll patients diagnosed with ATM by a neurologist between June 1, 2002 and June 30, 2010 were retrospectively identified using medical records in the general electronic database and the neurology department's database pertaining to Hospital Italiano in Buenos Aires.
Patients were examined and evaluated according to TMCWG criteria. All patients underwent brain and spinal MRI scans with and without gadolinium contrast. MRI scans were performed using a 1.5T scanner. Spinal MRI findings were divided into 3 categories according to the length of the lesions: partial myelitis (asymmetrical lesion affecting only 1 or 2 spinal cord segments); longitudinally extensive transverse myelitis (LETM) (central lesion extending 3 or more spinal cord segments); and multisegmental spinal cord lesions. Brain MRI findings were classified according to the Barkhof/Tintore criteria.8,9 Routine CSF studies and PCR testing were performed to check for herpes simplex, herpes 6, varicella-zoster virus, cytomegalovirus, Epstein-Barr virus and enterovirus. PCR tests for flavivirus were only performed in cases in which the virus was suspected. Oligoclonal bands (OCBs) and the IgG index in CSF were analysed using isoelectric focusing. We then tested all patients for HIV virus, syphilis, chlamydia, and mycoplasma. Tests to detect and measure autoantibodies, lupus anticoagulant, anticardiolipin antibodies, complement levels, and angiotensin converter enzyme levels were requested according to the criteria of the consultant neurologist.
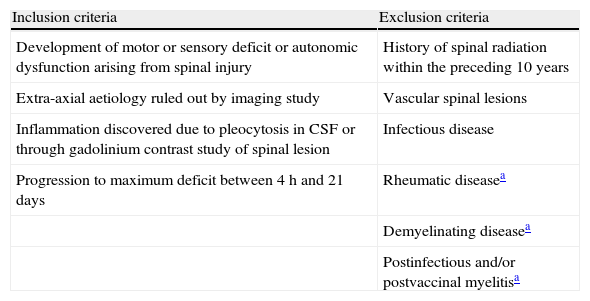
Data from only those patients who met the ATM diagnostic criteria established by the TMCWG were included in this study (Table 1).
Criteria for idiopathic ATM.
| Inclusion criteria | Exclusion criteria |
| Development of motor or sensory deficit or autonomic dysfunction arising from spinal injury | History of spinal radiation within the preceding 10 years |
| Extra-axial aetiology ruled out by imaging study | Vascular spinal lesions |
| Inflammation discovered due to pleocytosis in CSF or through gadolinium contrast study of spinal lesion | Infectious disease |
| Progression to maximum deficit between 4h and 21 days | Rheumatic diseasea |
| Demyelinating diseasea | |
| Postinfectious and/or postvaccinal myelitisa |
The study was approved by the hospital's ethics committee.
ClassificationAfter inclusion of eligible patients and analysis of clinical and paraclinical results, patients were divided into 2 major groups, an idiopathic ATM group and a secondary ATM group. For a diagnosis of secondary ATM, requirements were that the case should meet all inclusion criteria and also present with one of the diseases listed among the exclusion criteria (see Table 1).
Universally accepted standard criteria were used to diagnose multiple sclerosis (MS),10,11 clinically isolated syndrome (CIS),10,11 neuromyelitis optica (NMO),12 acute disseminated encephalomyelitis,13 postvaccinal myelitis,14 postinfectious myelitis,5 and rheumatic diseases.15–17
We gathered data regarding sex; age; date of symptom onset; any infections, vaccinations or trauma in the month prior to symptom onset; history of radiation treatment; time to reach maximum disability; maximum level of disability; level of disability after follow-up; and length of clinical follow-up.
Statistical analysisStatistical analysis was performed using Stata version 9.1. Categorical variables were expressed as percentages and numeric variables as mean±standard deviation. The χ2 test was used to analyse differences in frequency for categorical variables. The Mann–Whitney test was used to analyse continuous independent variables. The level of statistical significance was set at P<.05.
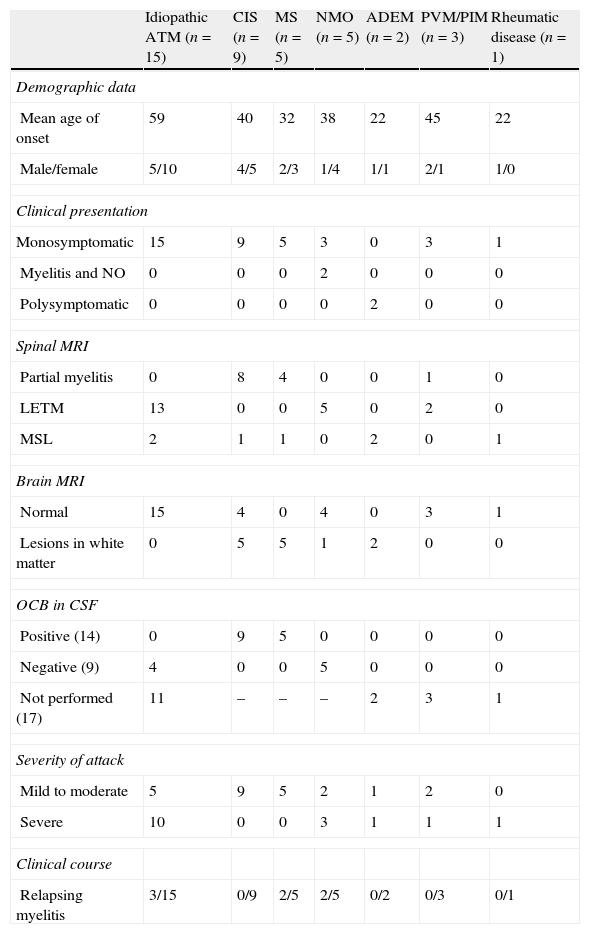
ResultsWe identified 40 patients diagnosed with ATM during the study period: 24 women (60%) and 16 men (40%) with a mean age at onset of 45.8±17.5 years (range, 18–79 years). Mean follow-up time was 57±10 months. The different aetiologies and main clinical and paraclinical characteristics are summarised in Table 2. Spinal MRI showed that the largest percentage of cases (50%) corresponded to LETM (Fig. 1). During follow-up, 17.5% (n=7) experienced at least one recurrence of myelitis. Of these patients, 43% (n=3) had idiopathic ATM, 28.5% (n=2) had NMO, and 28.5% (n=2) had MS. Mean follow-up time was 6.5±2 months.
Aetiology and demographic, clinical, and paraclinical characteristics of ATM cases included in the study (n=40).
| Idiopathic ATM (n=15) | CIS (n=9) | MS (n=5) | NMO (n=5) | ADEM (n=2) | PVM/PIM (n=3) | Rheumatic disease (n=1) | |
| Demographic data | |||||||
| Mean age of onset | 59 | 40 | 32 | 38 | 22 | 45 | 22 |
| Male/female | 5/10 | 4/5 | 2/3 | 1/4 | 1/1 | 2/1 | 1/0 |
| Clinical presentation | |||||||
| Monosymptomatic | 15 | 9 | 5 | 3 | 0 | 3 | 1 |
| Myelitis and NO | 0 | 0 | 0 | 2 | 0 | 0 | 0 |
| Polysymptomatic | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| Spinal MRI | |||||||
| Partial myelitis | 0 | 8 | 4 | 0 | 0 | 1 | 0 |
| LETM | 13 | 0 | 0 | 5 | 0 | 2 | 0 |
| MSL | 2 | 1 | 1 | 0 | 2 | 0 | 1 |
| Brain MRI | |||||||
| Normal | 15 | 4 | 0 | 4 | 0 | 3 | 1 |
| Lesions in white matter | 0 | 5 | 5 | 1 | 2 | 0 | 0 |
| OCB in CSF | |||||||
| Positive (14) | 0 | 9 | 5 | 0 | 0 | 0 | 0 |
| Negative (9) | 4 | 0 | 0 | 5 | 0 | 0 | 0 |
| Not performed (17) | 11 | – | – | – | 2 | 3 | 1 |
| Severity of attack | |||||||
| Mild to moderate | 5 | 9 | 5 | 2 | 1 | 2 | 0 |
| Severe | 10 | 0 | 0 | 3 | 1 | 1 | 1 |
| Clinical course | |||||||
| Relapsing myelitis | 3/15 | 0/9 | 2/5 | 2/5 | 0/2 | 0/3 | 0/1 |
MSL: multi-segment lesions; PIM: postinfectious myelitis; PVM: postvaccinal myelitis; NMO: neuromyelitis optica.

After 6 months of follow-up, 32.5% (n=13) of the patients had a motor disability. The motor disability was caused by LETM in 92.5% of the cases (n=12). There was a significant association between LETM and disability after 6 months, compared with partial and multisegmental myelitis (P=.001; odds ratio =; 95% confidence interval, 2.4–12).
DiscussionATM is an inflammatory neurological disorder with a variety of aetiologies. Given that specific diseases associated with ATM may have different treatments, a complete evaluation is needed in order to diagnose the disorder's aetiology.
In our current retrospective cohort study over 8 years of follow-up in an Argentinian population with a full-coverage health care system, we identified a total of 40 patients with ATM. A full aetiological examination showed that the most common type of ATM was secondary to demyelinating disease.
In 2005, De Seze et al. delivered a multicentre retrospective study carried out in France and including 288 patients.18 Also applying TMCWG criteria, these authors found that only 16% of cases of ATM were classified as idiopathic. ATM secondary to demyelinating disease represented 29% of the cases (MS 11% and NMO 17%) and was the main cause of ATM, as we also determined in our cohort.
On the other hand, recent studies have shown that patients with an initial episode of LETM present a high risk of recurrence if they are positive for NMO-IgG antibodies.19–21 These antibodies have expanded the spectrum of NMO-type disorders, and they are also found in ‘limited’ variants of this disease, including isolated or recurring forms of LETM.22,23
In our retrospective study, 37% of the cases (n=15) were idiopathic ATM; this percentage is high compared to those reported by studies from other countries. Although ATM secondary to demyelinating disease has also been found to be the most common type of ATM, it accounted for more than 50% of the patients in our study; this figure is very high compared to those from other studies.
We observed, as other prior studies have, that the length of the spinal lesion provides data which is helpful in determining ATM aetiology. Following this logic, partial myelitis cases were associated with MS and CIS, while LETM was associated with cases of NMO and idiopathic myelitis.
Significant results from the CSF studies included the fact that all patients with MS and CIS were positive for OCBs. While we do know that these data are not highly specific, they corroborate the high sensitivity for diagnosing MS which has been described for OCBs.10 On the other hand, the role played by OCBs as a factor predicting CIS conversion to MS is now well known,24–27 although their role in determining long-term prognosis requires further clarification.
Our retrospective study has several limits. These include lack of testing for NMO-IgG antibodies. For this reason, determining the true percentage of patients with LETM who formed part of the spectrum of NMO-type disorders was not possible. This fact may partially explain why the percentage of patients with idiopathic ATM was high in our study compared to previously published studies from other countries.18
On the other hand, we believe that our study's high percentage of cases of ATM associated with demyelinating diseases might have to do with the fact that our hospital is a regional centre of reference for the study of these diseases.
Despite its limitations, this study provides an overall idea of the clinical, aetiological and demographic aspects of ATM in the general population in Argentina.
Few clinical or epidemiological studies of ATM have been carried out in Argentina. We feel that understanding the way that this neurological disease presents in our region is crucial in order to compare our results with previously published results from other countries. Furthermore, given the therapeutic implications, it is extremely important to perform an exhaustive aetiological assessment so as to identify the different diseases that may be associated with ATM.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Chaves M, et al. Mielitis transversa aguda en Buenos Aires, Argentina. Estudio de una cohorte retrospectiva de 8 años de seguimiento. Neurología. 2012;27:348–53.
