




It is estimated that 30−50% of patients with heart failure with reduced ejection fraction (HFrEF) are women. This population appears to differ in terms of clinical characteristics, aetiology and treatment optimisation compared to men. Our main objective was to analyse these considerations, the influence of female sex on cardiac remodelling and neurohormonal response, as well as their impact on medium- to long-term prognosis.
MétodosRetrospective study of a cohort of HFrEF patients from real clinical practice. A comparative analysis was performed between male and female patients.
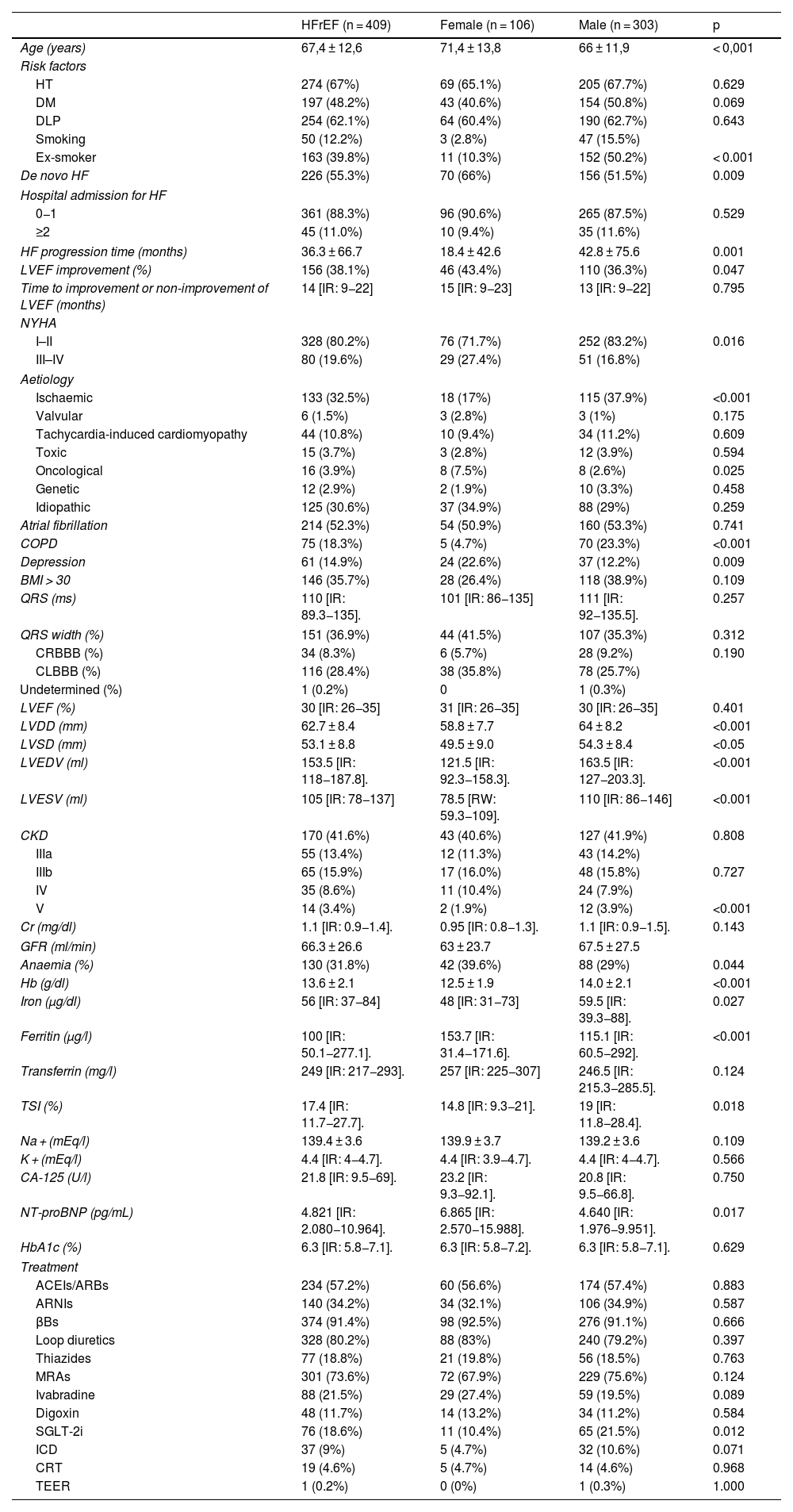
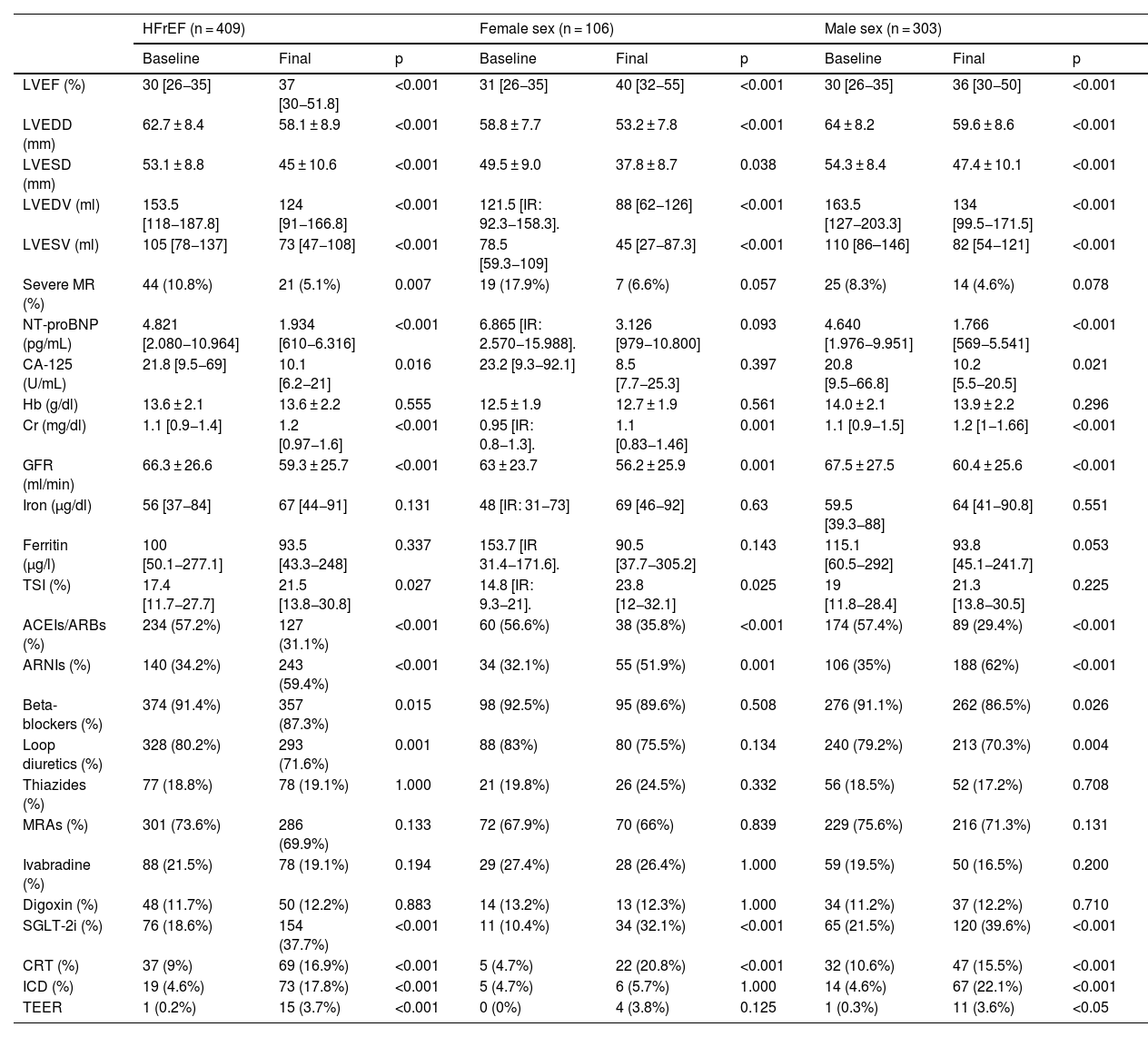
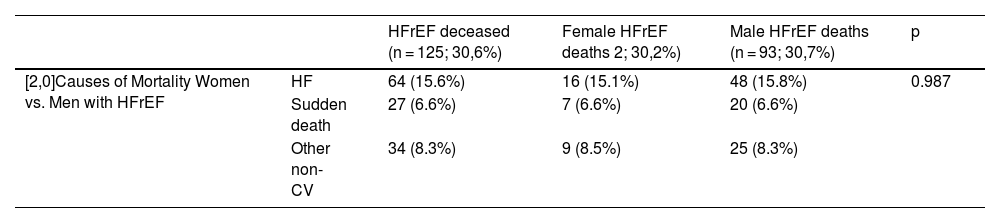
Resultados409 patients were analysed, a total of 106 females (25.4%), with a higher mean age than males (71.4 ± 13.8 vs. 66 ± 11.9; p < 0.001), higher prevalence of de novo HF (66.6% vs. 51.5%; p = 0.009), with a shorter HF evolution time (18.4 ± 42.6 vs. 42.8 ± 75.6 months; p = 0.001). Without significant differences in treatment optimisation, women had better cardiac remodelling at follow-up, as well as better neurohormonal response, with higher % reduction of NT-proBNP [−61,9% vs. −54,2%; p < 0.01], and of CA125 [−63,4% vs. −50,9%; p < 0.01]. With a median follow-up of 5 years, there were no differences in hospital readmissions or HF mortality in both sexes.
ConclusionesWomen with HFrEF have different clinical and aetiological characteristics compared to men. In evolution, they have better cardiac remodelling and neurohormonal response, although this has no impact on prognosis, readmission or mortality due to heart failure.
Se estima que entre el 30−50% de los pacientes con insuficiencia cardiaca con fracción de eyección reducida (ICFEr) son mujeres. Esta población parece presentar diferencias en cuanto a características clínicas, etiología y optimización del tratamiento con respecto al varón. Nuestro objetivo principal fue analizar estas consideraciones, la influencia del sexo femenino en el remodelado cardiaco y respuesta neurohormonal, así como su impacto en el pronóstico a medio-largo plazo.
MétodosEstudio retrospectivo de una cohorte de pacientes con ICFEr de práctica clínica real. Se realizó un análisis comparativo entre pacientes de ambos sexos.
ResultadosSe analizaron 409 pacientes, un total de 106 mujeres (25,4%), con una edad media superior al varón (71,4 ± 13,8 vs. 66 ± 11,9; p < 0,001), mayor prevalencia de IC de novo (66,6% vs. 51,5%; p = 0,009), con un tiempo de evolución de IC más corto (18,4 ± 42,6 vs. 42,8 ± 75,6 meses; p = 0,001). Sin grandes diferencias en la optimización del tratamiento, las mujeres tuvieron un mejor remodelado cardiaco en el seguimiento, así como una mejor respuesta neurohormonal, con mayor % de reducción de NT-proBNP [−61,9% vs. −54,2%; p < 0.01], y de CA125 [−63,4% vs. −50,9%; p < 0.01]. Con una mediana de seguimiento de 5 años, no hubo diferencias en cuanto a reingresos hospitalarios, ni mortalidad por IC en ambos sexos.
ConclusionesLas mujeres con ICFEr presentan características clínicas diferenciales, evolutivas y etiológicas con respecto al varón, obteniendo un mejor remodelado cardiaco y respuesta neurohormonal en el seguimiento, si bien esto no impacta en el pronóstico, en reingresos y mortalidad por IC.
