





Glenn surgery is used as a palliative procedure in children with Hypoplastic Left Heart Syndrome (HLHS) and its objective is to partially redirect the systemic venous return.
An individualized care plan is presented for a 7-month-old infant, admitted to the Pediatric Intensive Care Unit (PICU), after undergoing Glenn procedure. And is shown her evolution during admission.
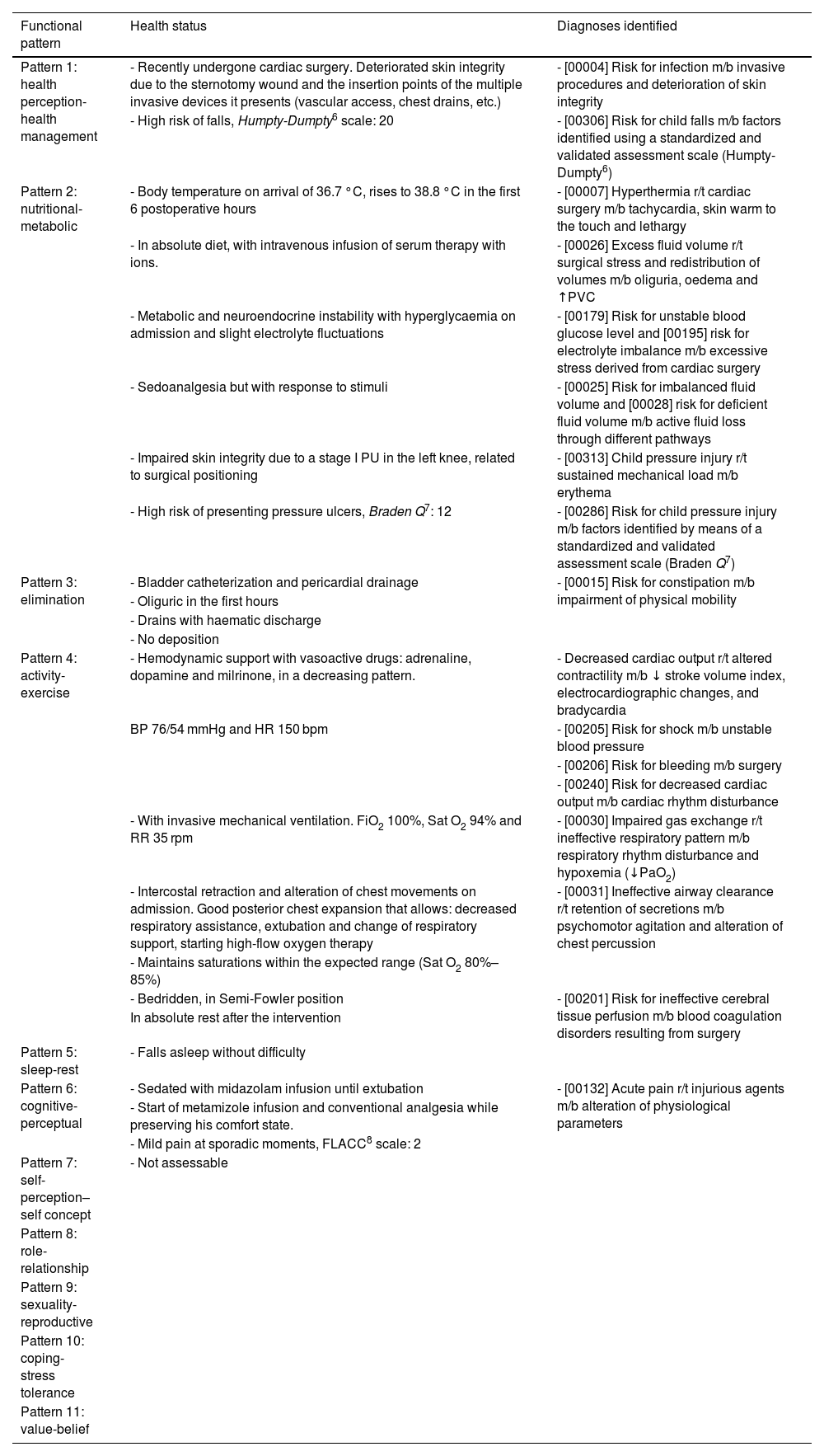
Marjorie Gordon's 11 functional health patterns are used for the nursing assessment, highlighting among the altered patterns, the nutritional-metabolic and the activity-exercise, due to their implication in hemodynamic changes derived from the surgery.
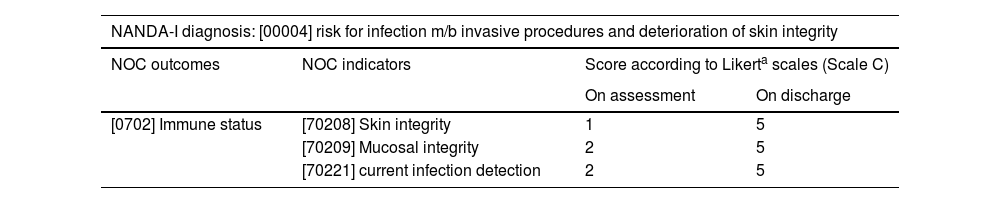
Due to their association with the most common postoperative complications in this type of surgery, 8 diagnoses were prioritised according to NANDA-I taxonomy: risk for infection, excess fluid volume, risk for shock, risk for bleeding, risk for decreased cardiac output, impaired gas exchange, ineffective airway clearance and risk for ineffective cerebral tissue perfusion.
In each of them, expected patient outcomes and nursing interventions, were selected using the NOC and NIC taxonomies, respectively.
Outcome criteria scores showed a favourable evolution after 7 days from admission, only 3 of the diagnoses selected at the beginning remain active.
The development and reassessment of the nursing care plan has made it possible to make an effective monitoring of patient’s postoperative evolution and to standardize nursing care, ensuring safe and quality health care.
The lack of similar case reports in available bibliography has prevented us from comparing actions, therefore it has been necessary to disclose these scientific articles to guarantee best evidence-based practice.
La cirugía de Glenn se emplea como procedimiento paliativo en los niños con ventrículo izquierdo hipoplásico y su objetivo es redirigir parcialmente el retorno venoso sistémico.
Se presenta un plan de cuidados individualizado de una lactante de siete meses de edad, que ingresa en la Unidad de Cuidados Intensivos (UCI) Pediátricos, tras ser intervenida del procedimiento de Glenn. Y se muestra su evolución durante el ingreso.
Para la valoración enfermera se utilizaron los 11 patrones funcionales de Marjory Gordon, destacando entre los patrones alterados, el nutricional-metabólico y el de actividad-ejercicio, por su relación con las alteraciones hemodinámicas derivadas de la cirugía.
Por su asociación con las complicaciones posquirúrgicas que ocurren con mayor frecuencia en este tipo de intervención, se priorizaron ocho diagnósticos según la taxonomía NANDA-I: el riesgo de infección, el exceso de volumen de líquidos, el riesgo de shock, el de sangrado, la probabilidad de disminución del gasto cardíaco, el deterioro del intercambio de gases, la limpieza ineficaz de las vías aéreas y el riesgo de perfusión tisular cerebral ineficaz.
Se seleccionaron para cada uno de ellos los resultados esperados y las intervenciones enfermeras específicas que se implementaron para su consecución, empleando las taxonomías NOC y NIC, respectivamente. Los criterios de resultados mostraron una evolución favorable transcurridos los siete días que duró el ingreso, manteniéndose activos solo tres de los diagnósticos iniciales.
La elaboración y progresión del plan de cuidados ha permitido realizar el seguimiento de la evolución postoperatoria de la paciente y homogeneizar los cuidados enfermeros, logrando una atención sanitaria segura y de calidad.
La escasez de casos clínicos similares en la bibliografía disponible nos ha impedido comparar actuaciones, por ello, se hace necesario dar a conocer este tipo de artículos científicos para garantizar la prestación de cuidados con base en la mejor evidencia.
Article
Diríjase al área de socios de la web de la SEEIUC, (https://seeiuc.org/mi-cuenta/iniciar-sesion/) y autentifíquese.

