







This study aims to describe the implementation of the standard methodology for information transfer in the labour ward and Intermediate Obstetric Care Unit and to identify the impact of this implementation on the factors that act as facilitators and barriers in the procedure.
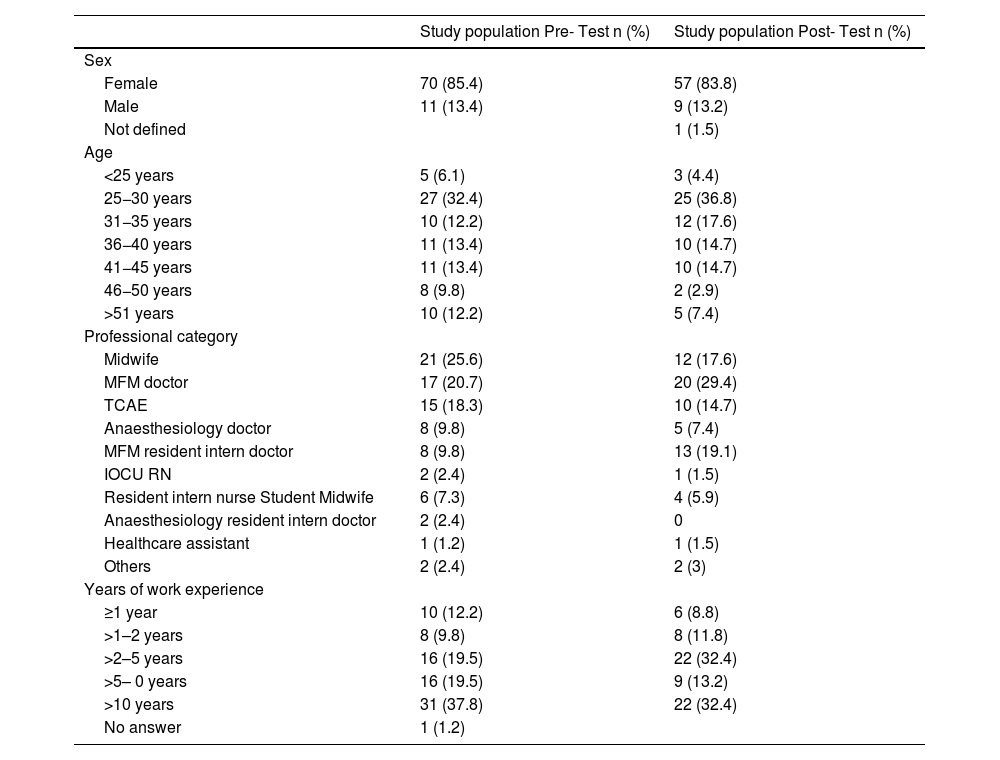
MethodQuasi-experimental pretest-posttest study without a control group in an Intermediate Obstetric Care Unit and delivery room of the Maternal-Fetal Medicine Service of a tertiary hospital in Barcelona. Healthcare staff self-completed an ad hoc questionnaire before and after implementing the standardised IDEAS methodology in the service during 2019 and 2020. Personal self-perception in the information transfer procedure was assessed. The Wilcoxon pairwise test was used for comparison before and after.
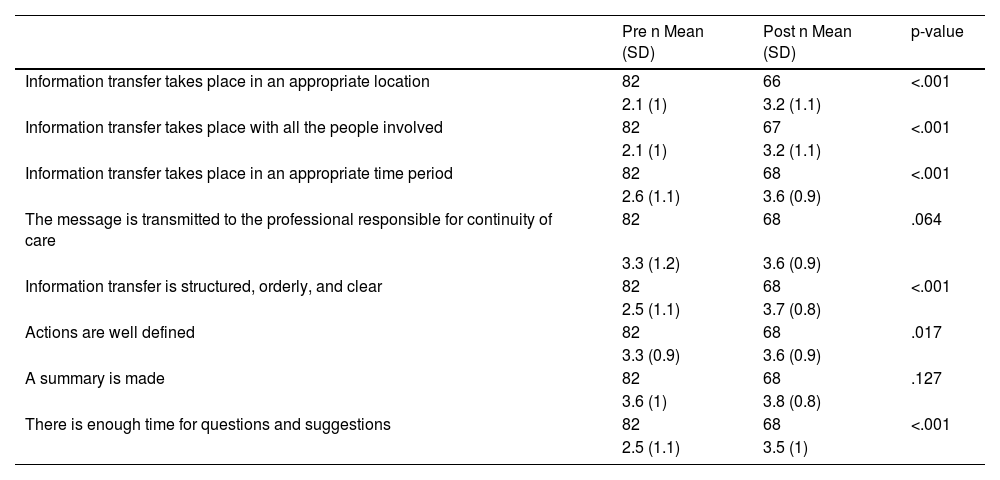
ResultsThe use of a standardised methodology has shown an impact on improving the transmission of information. Significant differences were detected before and after the intervention in the following dimensions: location, people involved, time period of the procedure, structured, orderly and clear, and sufficient time for questions (p < 0.001); while no differences were observed in: transmission to the referring professional, well-defined actions, and completion of a summary.
ConclusionsThere are factors such as structural and organisational aspects and lack of time that hinder effective communication and therefore act as barriers to the transfer of information. The implementation of a methodology with the health professionals involved, the time and the appropriate space allows for the improvement of communication aspects in the multiprofessional team and, therefore, patient safety.
Este estudio tiene como objetivo describir la implementación de la metodología estandarizada en la transferencia de información en sala de partos y Unidad de Cuidados Obstétricos Intermedios en un hospital de tercer nivel de Barcelona e identificar el impacto de esta implementación en los factores que actúan como facilitadores y barreras en el procedimiento.
MétodoEstudio cuasi experimental tipo pretest-postest sin grupo control en la Unidad de Cuidados Obstétricos Intermedios y sala de partos del Servicio de Medicina Materno Fetal de un hospital de tercer nivel de Barcelona. El personal sanitario auto cumplimentó un cuestionario adhoc antes y después de implementar la metodología estandarizada IDEAS en el servicio durante 2019 y 2020. Se evaluó la autopercepción personal en el procedimiento de transferencia de información. El test de Wilcoxon por pares se utilizó para la comparación antes y después.
ResultadosEl uso de una metodología estandarizada ha mostrado un impacto en la mejora de la transmisión de la información. Se detectaron diferencias significativas antes y después de la intervención en las siguientes dimensiones: ubicación, personas implicadas, periodo de tiempo del procedimiento, estructurada ordenada y clara y tiempo suficiente para preguntas (p < 0.001); mientras que no se observaron diferencias en: transmisión al profesional referente, actuaciones bien definidas y realización de un resumen.
ConclusionesExisten factores como, aspectos estructurales, organizativos y falta de tiempo que dificultan la comunicación efectiva, por tanto, actúan como barreras en la transferencia de información. La implementación de una metodología con las personas implicadas, el tiempo y el espacio adecuado permite mejorar aspectos en la comunicación en el equipo multiprofesional y, por tanto, la seguridad del paciente.
Article
Diríjase al área de socios de la web de la SEEIUC, (https://seeiuc.org/mi-cuenta/iniciar-sesion/) y autentifíquese.

