








To determine the internal consistency (IC), minimal detectable change (MDC), and sensitivity to change of the Barthel Index (BI) at ICU discharge and three months post-hospital discharge.
MethodsA prospective longitudinal study was conducted between November 2016 and July 2017 in a medical-surgical intensive care unit (ICU). A total of 149 patients over 18 years with a BI score >90 prior to ICU admission were included. The COSMIN checklist was utilized to evaluate the measurement properties. Clinical and demographic variables, BI scores, IC, MDC, and sensitivity to change were analyzed. The Cronbach's alpha coefficient (α) was calculated to determine the IC of the BI by domain and for the overall scale. Effect size (ES) indices and standardized mean response (SMR) were used for sensitivity to change. The MDC was identified using a distribution-based method, calculating the standard error of measurement (SEM). Floor and ceiling effects were assessed, with a threshold of less than 15% considered acceptable.
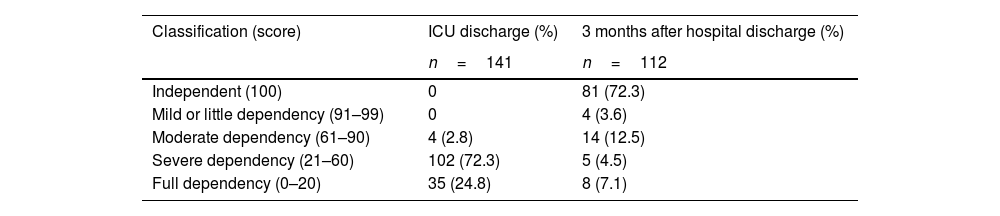
ResultsA total of 141 patients were evaluated at discharge from the ICU. Of these, n=77 (41.7%) were men, with a mean age of 58.5±16.8 years; n=62 (41.6%) required invasive mechanical ventilation. One hundred twelve patients were reassessed three months after discharge. The overall IC was: α=0.70 at ICU discharge and α=0.96 at three months. Ninety two percent (n=103) of the patients showed values greater than or equal to the MDC of 10 points, with statistically significant differences identified in the type of weaning, tracheostomy, and length of stay in the ICU (p<0.005).
ConclusionsThe items of the Spanish version of the BI demonstrate acceptable IC at ICU discharge. The MDC was 10 points, validating its responsiveness and utility for monitoring the functional independence of critically ill patients at ICU discharge and three months after hospital discharge.
Determinar la consistencia interna (CI), el cambio mínimo detectable (CMD) y la sensibilidad al cambio del índice de Barthel (IB) al alta de cuidados intensivos y 3 meses después del alta hospitalaria.
MétodosEstudio longitudinal prospectivo realizado entre noviembre de 2016 y julio de 2017 en una UCI médico/quirúrgica. Se incluyeron 149 pacientes mayores de 18 años con un IB>90 antes del ingreso en la UCI. Se utilizó la lista de chequeo COSMIN. Se analizaron las variables clínicas y demográficas, la puntuación del IB, la CI, el CMD y la sensibilidad al cambio. Se calculó el coeficiente alfa de Cronbach (α) para determinar la CI del IB por dominio y para la escala global. Para la sensibilidad al cambio, se usaron índices de tamaño del efecto (ES) y la respuesta media estandarizada (SRM). El CMD se identificó con el método basado en la distribución, calculando el error estándar de medición (SEM). Se evaluaron los efectos suelo y techo, considerando aceptable un umbral menor al 15%.
ResultadosSe evaluaron 141 pacientes al alta de la UCI. El n=77 (41,7%) eran varones con una edad media de 58,5±16,8 años y n=62 (41,6%) requirió ventilación mecánica invasiva; 112 pacientes fueron reevaluados 3 meses después del alta. La CI global fue: α=0,70 al alta de la UCI y α=0,96 a los 3 meses. El 92% (n=103) de los pacientes mostró valores mayores o iguales al CMD, de 10 puntos, identificándose diferencia estadísticamente significativa en el tipo de destete, traqueostomía y tiempo de estancia en la UCI (p<0,005).
ConclusionesLos ítems de la versión en español del IB presentan una CI aceptable al alta de la UCI. El CMD fue de 10 puntos, esto valida su capacidad de respuesta y su utilidad para el seguimiento de la independencia funcional de los pacientes críticos al alta de la UCI y a los 3 meses después del alta hospitalaria.
Artículo
Diríjase al área de socios de la web de la SEEIUC, (https://seeiuc.org/mi-cuenta/iniciar-sesion/) y autentifíquese.

