







The repair of ruptured abdominal aortic aneurysms (R-AAA) entails high mortality. This study aims to analyze differences in postoperative outcomes.
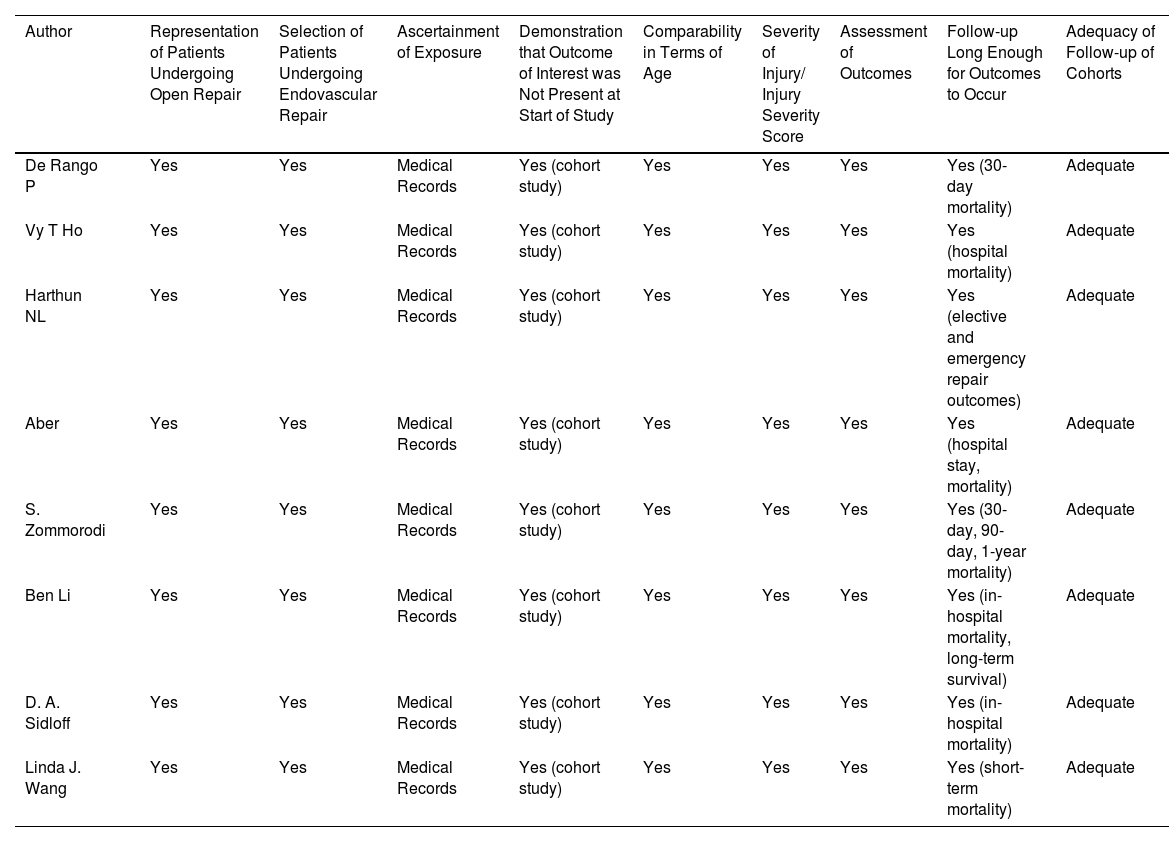
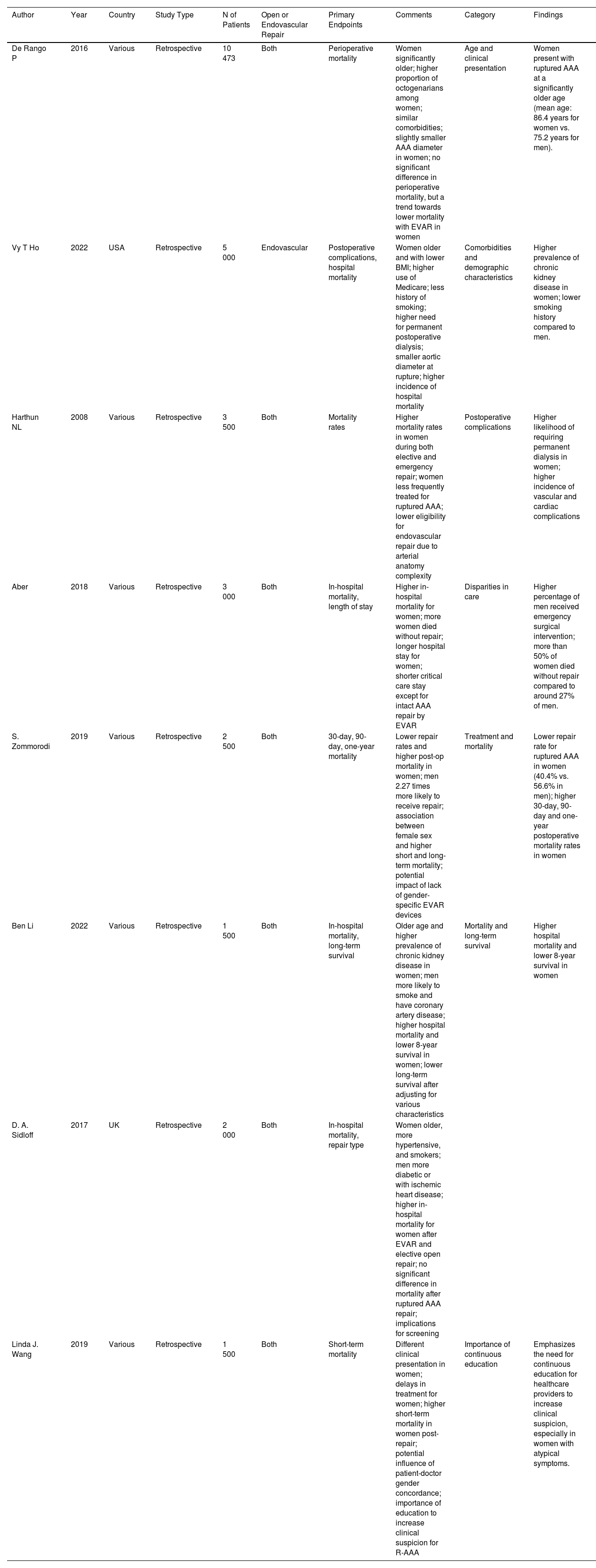
MethodsA meta-analysis was conducted of 8 studies involving 26 473 patients, evaluating 30-day mortality rates by comparing open surgical repair with endovascular repair and stratifying results by sex.
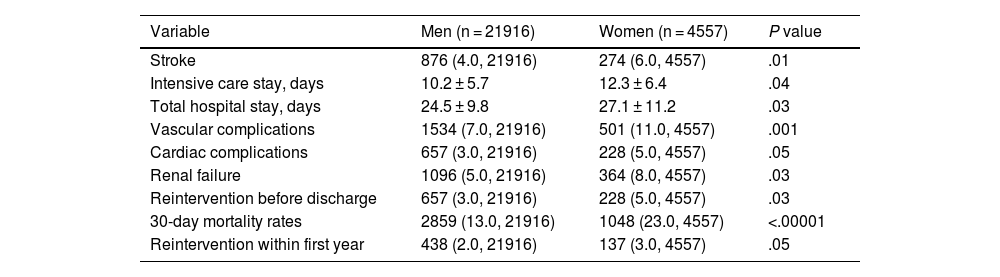
ResultsThe 30-day mortality rate was 23.0% in women versus 13.0% in men, with an odds ratio (OR) of 2.05. Women had higher rates of postoperative complications, such as stroke (6.0% vs. 4.0%) and renal failure (8.0% vs. 5.0%), as well as prolonged ICU stay (12.3 ± 6.4 days vs. 10.2 ± 5.7 days).
ConclusionThese findings highlight the importance of adjusting surgical approaches to improve outcomes in women with R-AAA. Continued prospective studies are recommended to optimize treatment protocols.
La reparación de aneurismas abdominales rotos (R-AAA) implica alta mortalidad. El objetivo de este estudio es analizar las diferencias entre géneros en los resultados postoperatorios.
MétodosSe realizó un metaanálisis de ocho estudios que incluyeron a 26,473 pacientes, evaluando las tasas de mortalidad a 30 días, comparando la reparación abierta con la endovascular y estratificando por género.
ResultadosLa mortalidad a 30 días fue del 23.0% en mujeres frente al 13.0% en hombres, con una OR de 2.05. Las mujeres presentaron mayores tasas de complicaciones postoperatorias, como accidentes cerebrovasculares (6.0% vs. 4.0%) y fallos renales (8.0% vs. 5.0%), así como una estancia en UCI prolongada (12.3 ± 6.4 días vs. 10.2 ± 5.7 días).
ConclusiónEstos hallazgos subrayan la importancia de ajustar los enfoques quirúrgicos para mejorar los resultados en mujeres con R-AAA. Es recomendable seguir realizando estudios prospectivos para optimizar los protocolos de tratamiento.
