






Proper management of thoracic drainages is essential in the recovery of patients after lung resection. This study evaluates the concordance in decision-making for drain removal depending on the type of drainage system used and the previous experience of the personnel.
Material and methodsProspective, comparative, and stratified randomization study on interobserver variability between senior specialist doctors and inexperienced healthcare personnel in the removal of thoracic drains in patients undergoing lung resection connected to conventional systems (CS) or digital systems (DS) with continuous recording. The withdrawal criteria were established before the study, and decisions were recorded during three postoperative days.
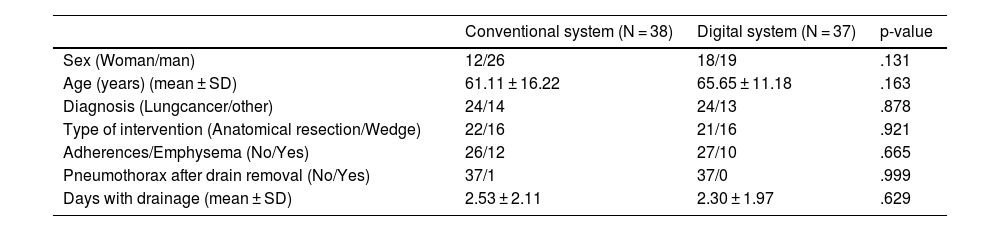
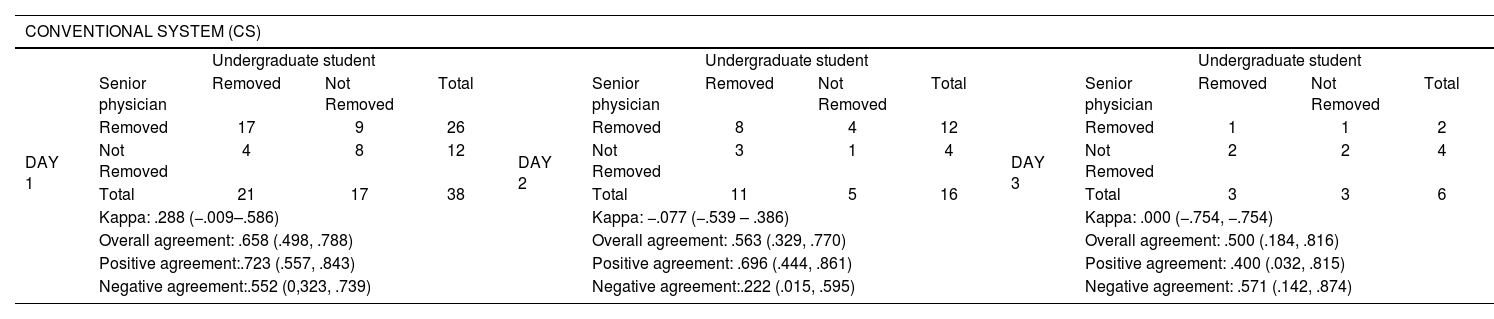
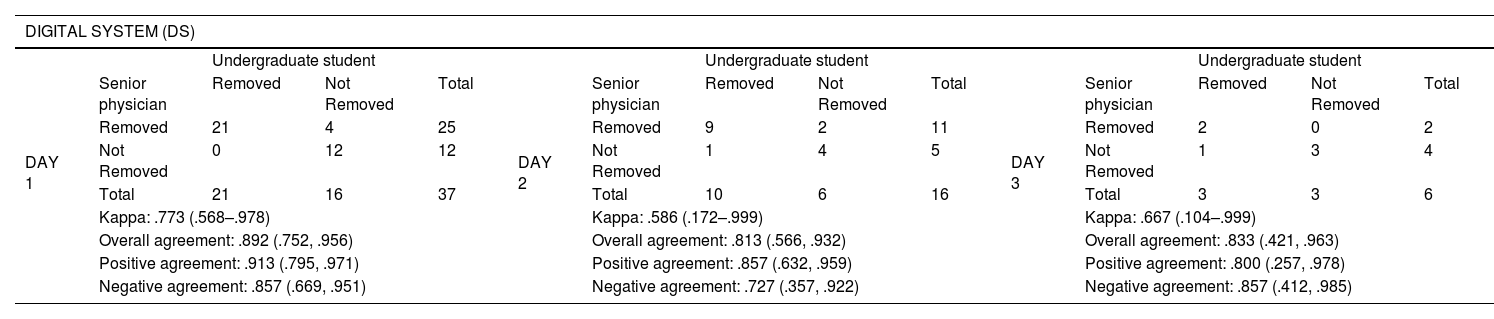
Results75 patients were included, 38 CS and 37 DS, with no statistically significant differences in sex distribution, age, intervention performed, presence of pleuropulmonary adhesions, drain time, or post-extraction complications between the groups. The overall concordance in drain removal decisions was moderate (kappa = 0.452), with notable variations in concordance depending on the drainage system used: CS (kappa = 0.188) with an overall agreement rate of 61.7% compared to DS (kappa = 0.716) with an overall agreement rate of 86.4%. Digital systems showed substantial concordance regardless of the operator's experience, with kappa values indicating high concordance on all postoperative days.
ConclusionsThe use of digital systems for managing thoracic drains significantly improves concordance in clinical decision-making regardless of the experience level. These findings suggest that adopting digital systems not only optimizes patient safety but also reduces the dependence on highly specialized healthcare professionals.
El manejo adecuado de los drenajes torácicos es esencial en la recuperación de los pacientes tras una resección pulmonar. Este estudio evalúa la concordancia en la toma de decisiones de su retirada dependiendo del sistema de drenaje utilizado y la experiencia previa del personal.
Material y métodosEstudio prospectivo, comparativo, de la variabilidad interobservador entre médico especialista senior y personal no experimentado en la retirada de drenajes torácicos en pacientes sometidos a resección pulmonar conectados a sistema convencional (SC) o sistema digitales (SD). Los criterios de retirada se establecieron antes del estudio y las decisiones se registraron durante tres días postoperatorios.
ResultadosSe incluyeron 75 pacientes, 38 SC / 37 SD, sin encontrarse diferencias estadísticamente significativas en la distribución de sexo, edad, intervención realizada, adherencias pleuropulmonares, tiempo con drenaje o complicaciones postextracción. La concordancia global en las decisiones de retirada del drenaje fue moderada (kappa = 0.452), observándose variaciones en la toma de decisiones dependiendo del sistema de drenaje utilizado: SC (kappa = 0.188) con tasa de acuerdo de 61.7% frente al SD (kappa = 0.716) con tasa de acuerdo de 86.4%. Los sistemas digitales demostraron una concordancia sustancial independientemente de la experiencia del operador.
ConclusionesLa utilización de sistemas digitales para el manejo de drenajes torácicos mejora significativamente la concordancia en la toma de decisiones clínicas, independientemente del nivel de experiencia previa. Estos hallazgos sugieren que la adopción de sistemas digitales no solo optimiza la seguridad del paciente sino que también reduce la dependencia de personal altamente especializado.

