





The breast is affected by a variety of benign disorders with a wide range of imaging and histopathological characteristics. Epidemiological investigations indicate that more than 50% of women will have one of the benign breast disorders beyond the age of 20 years.
ObjectivesThe objective of this study is to evaluate females with benign breast disorders attending the breast clinic in Duhok city by the triple assessment method.
Patients and methodsThis is a prospective study conducted in Duhok Breast Clinic at Azadi Teaching Hospital from May 2017 to July 2018 which included 445 female patients with benign breast diseases. The patients were assessed by the triple assessment method (clinical examination, imaging and histopathological evaluation), females from all age groups were included. Patients with malignant disease and male patients were excluded from the study.
ResultsThe mean age of the patients was 34.65 years; breast pain was reported in 403 patients 73 patients presented with breast lump or lumps, 42 patients presented with nipple discharge, 36 patients were presented with nipple retraction.
From these the total number of the patients 55 of them were reassured and no further work up was done, 235 sent for ultrasound examination,36 sent for mammography, 22 sent for both ultrasound and mammography and 4 patients were sent for MRI of the breast.
Excisional biopsy done for 37 patients, FNAC in 28 patients, tru cut biopsy in 10 patients and cytological examination for the fluid discharge in 18 patients.
Mastalgia was the commonest disorder seen in 376 patients, Ductectasia in 60 cases, Fibrocystic disease in 36cases, fibroadenoma in 33cases, breast cysts in 28 cases.
ConclusionsBenign breast diseases is a common problem in women, in this study mastalgia is the commonest followed by benign and inflammatory lesions. The use of the triple assessment to approach breast pathologies increase the diagnostic yield. Surgeons evaluating breast pain should have more rational criteria in using further sophisticated, expensive and invasive tests.
La mama se ve afectada por una variedad de trastornos benignos con una amplia gama de características de imagen e histopatológicas. Las investigaciones epidemiológicas indican que más del 50% de las mujeres tendrán uno de los trastornos benignos de los senos después de los 20 años.
ObjetivosEl objetivo de este estudio es evaluar a mujeres con trastornos benignos de la mama que asisten a la clínica de mama en la ciudad de Duhok mediante el método de triple evaluación.
Pacientes y métodosSe trata de una prospectiva realizada en la Clínica de mama Duhok del Hospital Universitario Azadi desde mayo de 2017 hasta julio de 2018. Se incluyeron en el estudio 445 mujeres con enfermedades benignas de la mama. Los pacientes fueron evaluados mediante el método de evaluación triple (examen clínico, imagenología e histopatología), se incluyeron mujeres de todos los grupos de edad. Los pacientes con enfermedad maligna y los pacientes masculinos fueron excluidos del estudio.
ResultadosLa edad media de los pacientes fue de 34,3 años; se informó dolor de mama en 403 pacientes73 pacientes presentaron un bulto o bultos en la mama, 42 pacientes presentaron secreción del pezón, 36 pacientes presentaron retracción del pezón.
De estos, el número total de pacientes 55 fueron tranquilizados y no se realizaron más estudios, 235 enviados para ecografía, 36 para mamografía, 22 para ecografía y mamografía y 4 pacientes para RM de mama.
Se realizó biopsia escisional en 37 pacientes, FNAC en 28 pacientes, biopsia trucut en 10 pacientes y examen citológico para la descarga de líquido en 18 pacientes.
La mastalgia fue el trastorno más común observado en 376 pacientes, ductectasia en 60 casos, enfermedad fibroquística en 36 casos, fibroadenoma en 33 casos, quistes de mama en 28 casos.
ConclusionesLas enfermedades benignas de la mama son un problema común en las mujeres, en este estudio la mastalgia es la más común seguida de las lesiones benignas e inflamatorias. El uso de la triple valoración para abordar patologías mamarias aumenta el rendimiento diagnóstico. Los cirujanos que evalúan el dolor de mama deben tener criterios más racionales al utilizar pruebas más sofisticadas, costosas e invasivas.
The breast is a preferential site for the occurrence of many benign lesions with a wide range of clinical, imaging, and histopathological characteristics. Epidemiological investigations indicate that more than 50% of women will have some disorders beyond the age of 20 years. Benign breast disorders are a group of breast diseases which is not cancer. It is the most common cause of breast problems in females.1,2
Non-cancerous disorders of the breast have great concern because of the public awareness of breast cancer, some may increase the risk of later breast cancer such as proliferative or atypical breast lesions have a two-fold risk of developing breast cancer in the future.3
Two classification systems are used to describe these benign disorders; the clinical and the pathological classification. The clinical classification is based on the symptoms and the signs and is more useful for the primary care physician. Females in their reproductive age experience varying degrees of breast swelling, fullness, lumpiness and tenderness which are related to the menstrual cycles and are physiologic and hormonally mediated. If in doubt present about the nature of the lumpiness, the patient should be examined after one or two menstrual cycles during midcycle when these changes regress. The pathologic classification based on tissue findings on biopsy, it is useful in assessing the risk of breast cancer.4,5
Breast pain, or mastalgia, is a very common symptom and usually associated with heaviness and tenderness. Mastalgia is broadly classified as either cyclic or noncyclic, based on its relationship to the menstrual cycle.5,6
Cyclic mastalgia usually starts few days before menses and subsides after that. It accounts for about two thirds of cases of mastalgia and is more responsive to treatment than the noncyclic one. Noncyclic mastalgia is unrelated menses and shows poorer response to therapy.7
The majority of breast lumps are benign. Nevertheless, they are a source of considerable anxiety. A benign mass is usually mobile with smooth and regular edges; it may be solid or cystic. A malignant mass is mostly firm and has irregular borders, and may be fixed to the skin or surrounding tissues. Cancer may cause skin changes or nipple retraction.8,9
Many women suffer from nipple discharge which may be physiological and is expressed with nipple manipulation. It may be bilateral and affects multiple ducts. The discharge may be milky, yellow, green, brown, or black, and is generally non-bloody and non-watery. A spontaneous non-malignant bloody discharge occasionally occurs in the third trimester. It resolves spontaneously and cancer should be excluded if it persists after delivery.10
Duct ectasia is a common cause of nipple discharge, followed by intraductal papilloma. Other causes include cancer and mastitis. A pathologic discharge warrants proper assessment. If the discharge is not bloody but shows signs of a pathologic process, it should be tested for occult blood. The role of nipple fluid cytology and galactography is controversial and will depend on local practice. Most patients with pathologic discharge will need terminal duct excision, which is diagnostic and therapeutic.10
Mastitis can be broadly classified into lactational and non-lactational. The diagnosis of lactational mastitis is generally straightforward and is due to obstruction of the breast ducts by engorged milk which become secondarily infected with bacteria. A wedge-shaped abscess subsequently develops. There is associated breast pain and axillary lymphadenitis. Treatment includes symptom-relieving measures like warm pads, analgesia, and continuing breast-feeding through the unaffected breast, antibiotics are usually needed. A localized abscess needs drainage. Non lactational mastitis usually presents as peri-areolar abscess, typically associated with duct ectasia, it has a chronic course. Sub-areolar and peri-areolar abscesses require surgical intervention because they may require duct excision. Mondor disease is rare self-limiting, it is defined as superficial thrombophlebitis of the breast. Any patient with mastitis that doesn’t resolve completely after one month of proper treatment will need biopsy to rule out inflammatory breast cancer.11
The triple assessment is the combination of the clinical breast examination, imaging, and tissue sampling. When the three assessments are done properly has a diagnostic accuracy that may reach 100%. It was initially described in 1975, by Haagensen. This will efficiently detect cancer and minimize unnecessary tests and procedures.12
Many new diagnostic tests such as tumor markers and some new imaging techniques are being used for the screening and the diagnosis of cancer and its differentiation from benign lesions. Ductal lavage for females at high risk of breast cancer such as strong family history of cancer or personal history of atypical proliferative disease may be done in combination with ductoscopy to obtain specimens for cytological examination.13
Tumor marker expression and immunohistochemical analysis of specimens may help to identify the subgroup of breast lesions with higher risk of malignant transformation.13
MRI is highly sensitive in diagnosing cancer because it can differentiate benign from malignant lesions, and assessing the axilla especially in patients with previous breast surgery. Technetium-99 labeled substances may have a role in the diagnosis of breast lesions that cannot be clearly assessed using the conventional mammography.14
Aim of the studyTo report the pattern of various benign breast diseases amongst females presented to Duhok Breast Clinic (DBC) emphasizing their assessment and categorizing them to initiate their natural profile which may help for possible future management.
Patients and methodsThis is a prospective, cross sectional descriptive study conducted in the DBC from May 2017 to July 2018 which included 445 female patients with benign breast diseases were included in the study. The patients were assessed by the triple assessment method (clinical examination, imaging and histopathological evaluation). All female patients who referred DBC with any benign disorder/disease from all age groups, were included. Women with malignant disease or those who had been treated for malignancy earlier, were excluded in this study. Male patients were excluded from the study.
The patients were required to give a consent prior to their enrolment in the study and a clearance was taken as per the institute's ethical committee guidelines.
The statistical calculations were done in Statistical Package for Social Sciences (SPSS 25:00 IBM: USA).
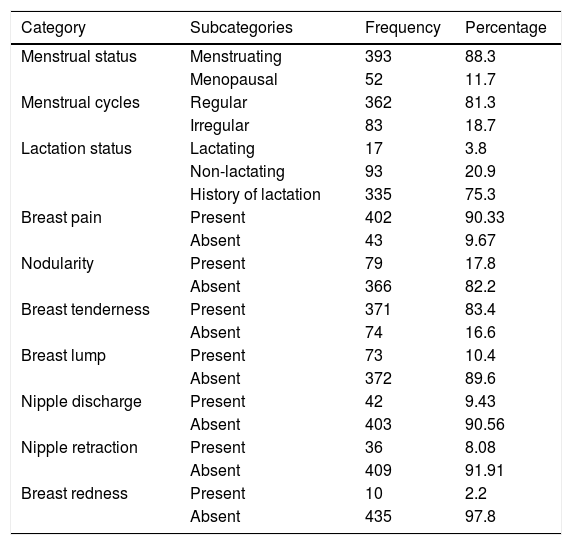
ResultsThe mean age of our patients was 34.65 years (SD: 10.717), with an age range 16-65 years. The mode of presentation and the patient characteristics are shown in Table 1.
Showing the patients characteristics and the types of presentations.
| Category | Subcategories | Frequency | Percentage |
|---|---|---|---|
| Menstrual status | Menstruating | 393 | 88.3 |
| Menopausal | 52 | 11.7 | |
| Menstrual cycles | Regular | 362 | 81.3 |
| Irregular | 83 | 18.7 | |
| Lactation status | Lactating | 17 | 3.8 |
| Non-lactating | 93 | 20.9 | |
| History of lactation | 335 | 75.3 | |
| Breast pain | Present | 402 | 90.33 |
| Absent | 43 | 9.67 | |
| Nodularity | Present | 79 | 17.8 |
| Absent | 366 | 82.2 | |
| Breast tenderness | Present | 371 | 83.4 |
| Absent | 74 | 16.6 | |
| Breast lump | Present | 73 | 10.4 |
| Absent | 372 | 89.6 | |
| Nipple discharge | Present | 42 | 9.43 |
| Absent | 403 | 90.56 | |
| Nipple retraction | Present | 36 | 8.08 |
| Absent | 409 | 91.91 | |
| Breast redness | Present | 10 | 2.2 |
| Absent | 435 | 97.8 |
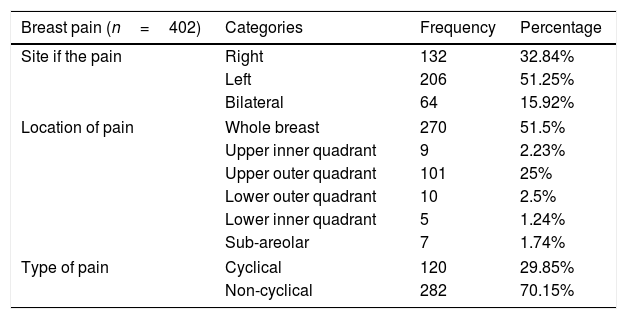
Breast pain was the commonest symptom in our patients, the detailed analysis of pain is presented in Table 2.
The analysis of the breast pain.
| Breast pain (n=402) | Categories | Frequency | Percentage |
|---|---|---|---|
| Site if the pain | Right | 132 | 32.84% |
| Left | 206 | 51.25% | |
| Bilateral | 64 | 15.92% | |
| Location of pain | Whole breast | 270 | 51.5% |
| Upper inner quadrant | 9 | 2.23% | |
| Upper outer quadrant | 101 | 25% | |
| Lower outer quadrant | 10 | 2.5% | |
| Lower inner quadrant | 5 | 1.24% | |
| Sub-areolar | 7 | 1.74% | |
| Type of pain | Cyclical | 120 | 29.85% |
| Non-cyclical | 282 | 70.15% | |
From those who presented with pain, 183 patients were normal with subsequent studies and 26 patients in addition to breast pain had pain in other sites such as the neck, shoulder or the chest wall.
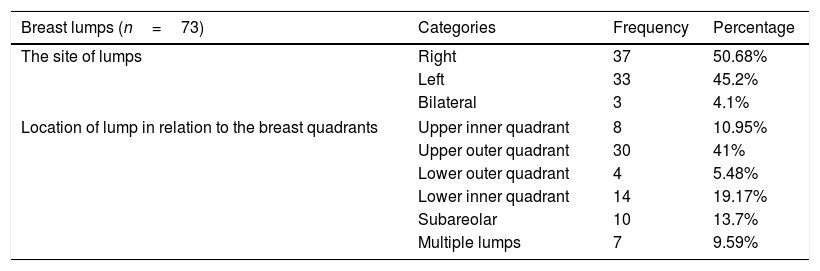
Seventy-three patients presented with breast lump or lumps, 7 of them had lumps at multiple sites (Table 3).
The site of the lumps and their locations in relations to the breast quadrants.
| Breast lumps (n=73) | Categories | Frequency | Percentage |
|---|---|---|---|
| The site of lumps | Right | 37 | 50.68% |
| Left | 33 | 45.2% | |
| Bilateral | 3 | 4.1% | |
| Location of lump in relation to the breast quadrants | Upper inner quadrant | 8 | 10.95% |
| Upper outer quadrant | 30 | 41% | |
| Lower outer quadrant | 4 | 5.48% | |
| Lower inner quadrant | 14 | 19.17% | |
| Subareolar | 10 | 13.7% | |
| Multiple lumps | 7 | 9.59% | |
Forty-two patients presented with nipple discharge, 21 of them were bilateral, 12 were from the left breast and 9 cases from the right breast, Fig. 1.

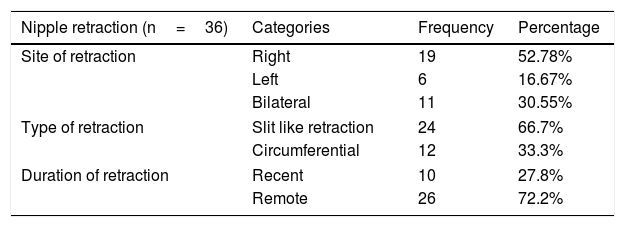
Thirty-sex patients had nipple retraction, the type of retraction is shown in Table 4.
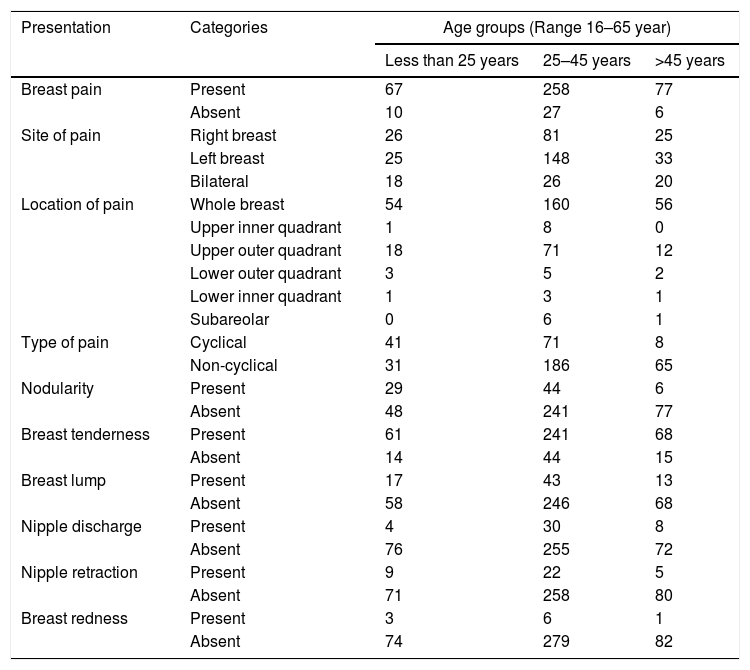
Different clinical presentations were also grouped according to different age groups (Table 5).
The types of clinical presentations according to the age groups.
| Presentation | Categories | Age groups (Range 16–65 year) | ||
|---|---|---|---|---|
| Less than 25 years | 25–45 years | >45 years | ||
| Breast pain | Present | 67 | 258 | 77 |
| Absent | 10 | 27 | 6 | |
| Site of pain | Right breast | 26 | 81 | 25 |
| Left breast | 25 | 148 | 33 | |
| Bilateral | 18 | 26 | 20 | |
| Location of pain | Whole breast | 54 | 160 | 56 |
| Upper inner quadrant | 1 | 8 | 0 | |
| Upper outer quadrant | 18 | 71 | 12 | |
| Lower outer quadrant | 3 | 5 | 2 | |
| Lower inner quadrant | 1 | 3 | 1 | |
| Subareolar | 0 | 6 | 1 | |
| Type of pain | Cyclical | 41 | 71 | 8 |
| Non-cyclical | 31 | 186 | 65 | |
| Nodularity | Present | 29 | 44 | 6 |
| Absent | 48 | 241 | 77 | |
| Breast tenderness | Present | 61 | 241 | 68 |
| Absent | 14 | 44 | 15 | |
| Breast lump | Present | 17 | 43 | 13 |
| Absent | 58 | 246 | 68 | |
| Nipple discharge | Present | 4 | 30 | 8 |
| Absent | 76 | 255 | 72 | |
| Nipple retraction | Present | 9 | 22 | 5 |
| Absent | 71 | 258 | 80 | |
| Breast redness | Present | 3 | 6 | 1 |
| Absent | 74 | 279 | 82 | |
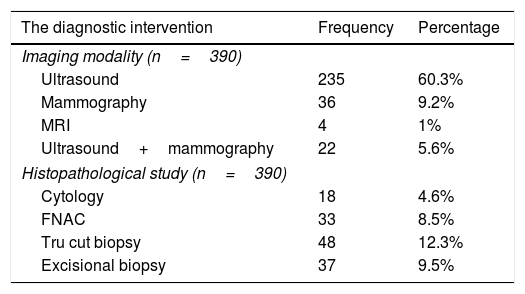
From these 445 patients 55 of them were reassured and followed up and no further test were needed, and the rest of the patients were sent for radiological and histopathological examination (Table 6).
Showing the types of the diagnostic interventions.
| The diagnostic intervention | Frequency | Percentage |
|---|---|---|
| Imaging modality (n=390) | ||
| Ultrasound | 235 | 60.3% |
| Mammography | 36 | 9.2% |
| MRI | 4 | 1% |
| Ultrasound+mammography | 22 | 5.6% |
| Histopathological study (n=390) | ||
| Cytology | 18 | 4.6% |
| FNAC | 33 | 8.5% |
| Tru cut biopsy | 48 | 12.3% |
| Excisional biopsy | 37 | 9.5% |
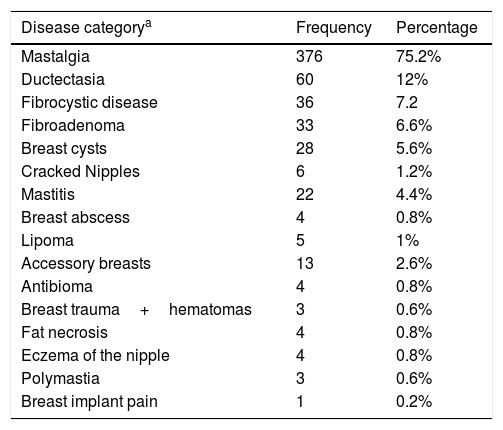
After the triple assessment for the patients, the various disease categories were diagnosed as shown in Table 7.
The types of the imaging and the histopathological tests performed for the patients.
| Disease categorya | Frequency | Percentage |
|---|---|---|
| Mastalgia | 376 | 75.2% |
| Ductectasia | 60 | 12% |
| Fibrocystic disease | 36 | 7.2 |
| Fibroadenoma | 33 | 6.6% |
| Breast cysts | 28 | 5.6% |
| Cracked Nipples | 6 | 1.2% |
| Mastitis | 22 | 4.4% |
| Breast abscess | 4 | 0.8% |
| Lipoma | 5 | 1% |
| Accessory breasts | 13 | 2.6% |
| Antibioma | 4 | 0.8% |
| Breast trauma+hematomas | 3 | 0.6% |
| Fat necrosis | 4 | 0.8% |
| Eczema of the nipple | 4 | 0.8% |
| Polymastia | 3 | 0.6% |
| Breast implant pain | 1 | 0.2% |
Breast disorders include a heterogeneous group of conditions which range from normal, aberrations in the normal physiology, to frank disease. Patients with benign breast diseases generally present with breast pain, breast lump, lumpiness, nipple discharge, nipple retraction, problems related to the size of the breasts, or some other presentations.15,16
In our study breast pain was reported in 403 patients (90.33%), 132 patients (32.84%) presented with pain in the right breast, 206 patients (51.25%) had pain in the left breast and 64 patients (15.92%) had bilateral breast pain, the majority of our patients (51.5%) had pain in the whole breast and 25% of them had pain in the upper outer quadrant. A study done in India involving 18659 patients showed that right side breast involvement in 47.63%, the left breast was involved in 39.73% and both breasts in 12.63%. In another study from Pakistan which involved 800 females, it showed that 71.42% of then presented with breast pain and 34% had breast tenderness, in our study 310 patients (62%) had breast tenderness on examination.17,18
The pain was cyclical in 120 patients (29.85%) and noncyclical in 282 patients (70.15%), 26 patients (5.2%) in addition to breast pain had pain in other sites such as the neck in 1.9%, the shoulder in 1.3% or the chest wall in 2%.19
Ductectasia was diagnosed in 60 patients (12%) and 42 patients (8.4%) complained from nipple discharge, the majority of the patients were in the 3rd and the 4th decade of life, 6 cases had bloody nipple discharge and on subsequent tests 3 of them were diagnosed as intra-ductal papilloma and they underwent microductectomy, the histopathology showed benign lesions, 6 cases of a study which was done by Engin (3%) were diagnosed as intra-ductal papilloma.20,21
From the cases complained from nipple discharge, 3 cases had bilateral galactorrhea and one case diagnosed as pituitary adenoma and referred to the neurosurgeon. In the study of Imad El-Hag 16.9% of his patients presented with nipple discharge, while that done by Mim B showed that 8% of his patients were complaining from ductectasia.22–24
The treatment of the nipple discharge must be done first, to exclude carcinoma. Mammary duct ectasia generally does not require surgery and it should be managed conservatively, reassurance may be sufficient, but when the discharge is intolerable surgery may be needed done to excise the affected ducts. Four of our patients underwent quadrantectomy for chronic intolerable discharge, 2 of them have more than one operation for the same problem in the past. The fibrocystic disease was diagnosed in 36 patients (7.2%) in our study and the majority of the patients belonged to the 2nd decade of life, breast cysts were diagnosed in 5.6% of our cases, in a study which was done by Harold Ellis, he showed that 22.3% of his patients were diagnosed as fibrocystic changes and 15% of patients had breast cysts. The study done by Engin showed that 23.5% of patients had fibrocystic disease and 22.5% of patients had breast cysts.20,22,23
It has been recommended that all the patients with discrete breast lumps should undergo a triple assessment, by this approach we provide the diagnoses of most of the benign and malignant breast conditions. In our study, 73 patients (14.6%) presented with breast lump or lumps, the lump was located in the right breast in 37 patients (50.68%), in the left breast in 33 patients (45.2%), and 3 cases (4.1%) had bilateral breast lumps. Fibroadenomas comprises the most common of the lumps and accounts for 6.6% of the lumps. Lipoma of the breast diagnosed in 1% of our patients which is higher than the percentage in a Nigeria study showing 0.6%.25–27
Accessory breasts were present in 13 of our patients (2.6%), from these 6 of them underwent surgery. In a study done by Babatunde the percentage of the accessory breasts was 2.5%.28
Thirty-sex patients (7.2%) presented with nipple retraction, 18 cases diagnosed as ductectasia,10 cases were normal with subsequent tests,6 cases had fibrocystic disease and 2 cases had chronic sub-areolar abscesses, ductectasia cause chronic periductal inflammatory process and eventually this will cause fibrosis and nipple retraction.
Breast trauma and hematomas were diagnosed in 3 patients (0.6%) and all of them had blunt trauma to the breast. One case with breast implant had pain after the implant placement.29
Four cases (0.8%) presented with fat necrosis after old trauma and malignancy excluded by tru cut biopsy. Imad El-Hag showed that 8% of his patients diagnosed as having fat necrosis, sometimes the clinical examination of fat necrosis and malignancy is very similar and the assessment should include the tissue examination either by tru cut biopsy or even surgical excision. Four of our cases (0.8%) had eczema of the nipple which was bilateral and consultation to the dermatologist done and treatment given.22,30
ConclusionsBenign breast diseases is a common problem in women, in this study mastalgia is the commonest followed by benign and inflammatory lesions. The use of the triple assessment to approach breast pathologies increase the diagnostic yield. Surgeons evaluating breast pain should have more rational criteria in using further sophisticated, expensive and invasive tests.
FundingThe author is the only source of funding.
Ethical considerationsThe study is approved by the local ethical surgical committee.
Conflicts of interestThere is no conflict of interest to be declared.

