




To determine the thickness of dental tissue through which Prime Dent Resin® might exhibit light-polymerization with minimum shrinkage and suitable curing depth.
Method80 laminae measuring 1, 2, 3 and 4mm thickness were obtained from molars (20 laminae per group). Contraction was measured and resin shrinkage was calculated by polymerization (Visilux 2, 3M) though each lamina (60 s, 400 mW/cm2). Bonded-disk technique was used. Depth of curing tests were undertaken by measuring the thickness of polymerized resin according to ADA's specification number 27. A control group without dental tissue was prepared for both properties. Data were analyzed using ANOVA with Tukey test (p < 0.001).
ResultsCuring depth: curing depth decreased as thickness increased. All groups revealed statistically significant differences. The thickness that exhibited lesser shrinkage nonetheless meeting with suitable curing depth (ADA establishes minimum value of 1mm) was the 3mm group. Shrinkage: as thickness increased, shrinkage decreased; no statistically significant difference was reported for groups 2 and 3mm.
ConclusionsAccording to obtained results, it is possible to polymerize through a 3mm thickness, therefore polymerization is not recommended through a 4mm depth. It will be necessary to obtain further mechanical properties using different thicknesses of dental tissue.
Determinar el espesor de tejido dental a través del cual se presente la fotopolimerización de la resina Prime Dent® con mínimo encogimiento y profundidad de curado adecuada.
MétodoSe obtuvieron 80 láminas de molares de 1, 2, 3 y 4mm de espesor (20 por grupo). Se midió la contracción y se calculó el encogimiento de la resina polimerizando (Visilux 2, 3M) a través de cada lámina (60 s, 400 mW/cm2). Se utilizó la técnica de bonded-disc. Se realizaron pruebas de profundidad de curado, midiendo el espesor de resina polimerizada de acuerdo con la especificación No. 27 ADA. Un grupo control sin tejido dental fue preparado para ambas propiedades. Los datos fueron analizados usando ANOVA con prueba de Tukey (p < 0.001).
ResultadosProfundidad de curado: a medida que aumentó el espesor, ésta disminuyó, existiendo diferencia estadísticamente significativa en todos los grupos. El espesor que mostró menor encogimiento, cumpliendo con una profundidad de curado adecuada (ADA marca como valor mínimo, 1mm) fue de 3mm. Encogimiento: a medida que aumentó el espesor, éste disminuyó, no existiendo diferencia estadísticamente significativa entre los grupos de 2 y 3mm.
ConclusionesDe acuerdo con los resultados, es posible polimerizar a través de un espesor de 3mm, por lo que no se recomienda polimerizar a través de un espesor de 4mm. Es necesario obtener más propiedades mecánicas utilizando diferentes espesores de tejido dental.
Contraction and general effort generated in dental resins during polymerization are the main problems encountered in adhesive dentistry, since they interfere with the integrity of the restored tooth.1
Polymerization of dental composite resins is accompanied by a 1.5 to 5% volumetric contraction, which causes an internal effort.2
Effort concentration is greater in the restorationtooth inter-phase and can be the cause of space formation at the margins, margin discoloration, postoperative sensitivity and secondary caries.3–6
In composite resins polymerization, the chemical reaction involves breakage of double links carbon-carbon to form polymeric chains with carbons linked by simple links.7,8
Contraction caused by monomer polymerization is caused by conversion of inter-molecular forces (called Van der Waals) in simple covalent links during polymerization.
Initially, contraction in a cavity is totally compensated by the composite resin flow, nevertheless, within a short time after polymerization begins, there is a decrease in flow and the resins begins to transfer effort to the cavity's walls.9
One way to reduce contraction would be to decrease light intensity, since it has been shown that post-gel contraction as well as residual effort are dependent on the intensity of curing light.
To this date, there are few studies assessing light-polymerization alternative methods (varying light transmission) to reduce contraction.
Davidson10 found that ramp polymerization caused lesser contraction (approximately 33% of total volumetric contraction) and similar degree of conversion when compared to a continuous light activation.
A discontinued light-polymerization does not significantly decrease contraction. A two-step curing technique (lesser light intensity followed by greater intensity) allowed to reduce contraction to 19 and 30% of all total volumetric contraction.11–13
Studies conducted on marginal integrity when using «soft-start» polymerization (polymerization beginning with low intensity to be followed by normal intensity) showed contradictory results.
While some studies reported better marginal integrity when non-continuous curing methods were used (ramp polymerized and «soft start»),14–19 other studies did not report significant differences when comparing these techniques with the conventional method. Nevertheless, it must be taken into account that when intensity is decreased, polymerization degree associated to mechanical properties will also decrease and this could impact in a poor clinical performance of the restorations. Use of greater intensity can exert a negative effect on restorations’ marginal integrity since it causes faster polymerization contraction and can increase the magnitude of contraction-associated method. Nevertheless, use of high intensity generally results in higher polymerization degrees, which in turn is associated to improvement of mechanical properties and biocompatibility of composite resins.20–22 The aim of the present research was to determine at which thickness of dental tissue Prime Dent® resin could achieve suitable polymerization with minimum shrinkage, as well as assessing curing depth of said composite resin.
The hypothesis to be tested in the present research project was the proposal that there is an existing relationship between thickness of dental tissue through which Prime Dent® resin is polymerized and the degree of shrinkage caused by polymerization.
MATERIAL AND METHODSFor the present study molars free of caries and fracture as well as lacking structural defects were selected. Cuts were undertaken in the sagittal plane so as to obtain dental tissue laminae measuring 1, 2, 3, and 4mm depth. 20 laminae were obtained for each thickness. Thickness groups were called A, B, C and D respectively. Cuts were executed with a trimmer (Hamco Machines Inc, Rochester NY).
Polymerization was undertaken with Prime Dent A3® resin laminae (Prime Dental Manufacturing Inc., USA).
POLYMERIZATION-INDUCED SHRINKAGENon-polymerized resin was extracted from the syringe, weighed and placed in a plastic container in order to prevent polymerization onset caused by environmental light. Weight of the resin sample varied from 0.12 to 0.15 grams. With a spatula used for cements, resin was placed at the center of each dental lamina. After this, a 1.24mm high bronze ring was put into place.
A slide cover (22 × 22 × 0.13mm) was placed on the resin, pressure was then exerted with a slide (75 × 25 × 1mm) against the surface of the ring, so as to ensure uniform thickness in the resin sample (1.24mm). Once the slide was removed, the sample was transferred to the contraction-measuring test instrument. This instrument included a metallic base with an 8mm diameter orifice, a transducer (Solatron OD5, Solatron Metrology England) which had a freemoving rod connected to a data capturing equipment (PICO ADC-16, Pico Technology Ltd, Hardwick, Cambridge UK).
All samples were polymerized for 60seconds through the dental lamina (according to manufacturer's instructions for A3 shade). Using a light-polymerization lamp (Visilux 2, Dental Products 3M, St Paul MN, USA) which provided light output of 400 mW/cm2, light intensity was measured with a curing radiometer (Demetron, Model 100, Demetron Research Corp, Danbury, CT USA).
Polymerization-induced shrinkage was calculated8 in each sample during 600seconds (60seconds of light irradiation and 540 with no irradiation).
As a control group, resin samples were polymerized substituting dental laminae with glass slide covers, which were reported as 0mm thick.
CALCULATION OF CONTRACTION AND SHRINKAGETransducer calibrationA conversion factor was required in order to transform voltage data captured by PICO ADC-16 and transform them to a longitude measure. Voltage values in function of a micrometer (Mitutoyo, Japan) displacement (distance) were expressed in a graph, the relationship between both values represented the conversion factor which we called K. K was calculated through a linear regression (r2 = 0.9996) and was registered as 17.46mV/μm.
The fact of converting voltage values into displacement values allowed the calculation of polymerization-induced contraction as well as shrinkage using the following mathematical expressions:

Where Lo is the initial thickness (thickness of the bronze ring) with a value of 1.24mm and Lt is the thickness at different times.
Lt was calculated when relating exit voltage with K calibration factor such as:

Where Vt is voltage at different times and Vt 0 is voltage at the beginning of the test.
Shrinking percentage (S) was calculated in function of time, such as:

These equations allowed to obtain the graph %S-time
Curing depthA metal mold (6mm high, 4mm diameter) was placed on a polystyrene clear film (Mylar), the mold was then filled with resin care being exerted not to trap any air bubbles. With use of resin, the upper limit of the mold was exceeded, placing a second clear film. Pressure was exerted on the mold and the bands located between slides so as to allow flow of excess material. The upper slide was removed, and the corresponding dental tissue lamina was placed. All specimens were irradiated by placing the tip of the lamp against the surface of the dental tissue, according to manufacturer's instructions.
After exposition to light, samples were removed from the mold with a plastic spatula, non-polymerized material was removed and the height of the cured material cylinder was measured with a micrometer (Fowler & NSK Japan.) Obtained value was divided by two according to ADA norm 27 requirements.23 This figure was recorded as curing depth. Test of curing dept in light-polymerized resin samples without interposition of dental tissue was conducted (control group).
Statistical analysisStatistical analysis was conducted using Sigma-Stat 2.03 (SPSS Science). One way ANOVA with Tukey test with statistical significance of 99.9% (p < 0.001) was used to execute comparisons among groups.
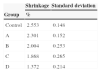
RESULTSPolymerization-induced shrinkageMean shrinking values obtained as well as their standard deviations are shown in table Iandfigure 1. With exception of groups B and C all groups presented polymerization-induced shrinkage with statistically significant differences.

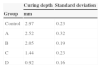
Table IIandFigure 2 show average values of curing depth as well as their standard deviations. Multiple comparisons executed with Tukey test revealed statistically significant differences for all groups.

Figures 1 and 2 show linear behavior between shrinking and curing depth values. This would indicate that thickness is directly proportional to both properties.
DISCUSSIONIn the present study, it was found that as dental lamina thickness increased (lamina interposed between light source and resin sample) shrinkage decreased from 10 to 46% (10, 21, 27 and 46% respectively) with respect to control group. This could be due to lesser passage of light as dental tissue thickness increases, since the tooth absorbs energy originating from the light-polymerizing lamp. This absorption can vary in direct relation with the chemical composition of the tooth. Therefore, patient age is another importantly influencing factor; to greater age, greater mineralization.24 When the resin is placed in a cavity, polymerization-induced contraction can be decreased by placing the material in small increments, while combining this with a modified light-polymerization technique.
When conducting a comparison with other light-polymerization techniques, the present study revealed a shrinkage decrease of 10 to 46% when compared to the technique of not polymerizing through the tooth. These results are similar to those obtained when using «soft start» polymerization technique used by Lim13 (19-30%).
Obici19 using Z100 and P60 resins, conducted a comparative study using continuous irradiation technique and «soft start» technique. He found that Z100 exhibited 36% reduction and P60 a 25% reduction when comparing «soft start» technique with the continuous method. Both the aforementioned resins possessed Bis-GMA as main component of their formula, such is the case of Prime-Dent® resin, used in the present study, therefore there is a common point between Obici's study and the present one.
Polymerization through the tooth is presented as an alternative which offers significant shrinkage reductions which are similar to those reported in other research projects that used the «soft start» technique.
Light-polymerization through the tooth is affected by the thickness of the cavity wall, therefore it is necessary to use an intra-oral gauge in order to ensure that minimum thickness is at least 2-3mm.
Figure 1 shows the influence of dental tissue thickness, in it, it can be seen that group D exhibited lesser contraction (4mm) followed by group C.
Figure 2 shows that control group was the group with greater curing depth (with no interposed dental lamina); it was followed by group A (1mm thickness). Nevertheless, these groups exhibited the greatest contraction (2.553 and 2.301%).
When relating both properties and trying to find a balance between them (lesser contraction and greater curing depth) the following was found:
- 1.
According to ADA's norm 27,23 the minimum acceptable value for curing depth is 1mm. Therefore, groups A, B and C met this requirement.
- 2.
When comparing groups A, B and C, Group C (3mm thick) exhibited the lesser shrinkage.
- 3.
Group C exhibited 27% shrinkage reduction when compared to direct resin polymerization technique.
Nevertheless, shrinkage reduction decreasing intensity or time of irradiation can result in lesser chain cross-linking and therefore affect the polymer's mechanical properties.
Davidson10 found that when using high light intensity in light-polymerization procedures, mechanic properties and conversion degree are increased, even though once the gelation point is reached, relationship between light intensity and conversion degree is no longer linear.20 Furthermore, relationship between intensity and post-gel chain shrinking is indeed linear. Therefore, high intensities produce greater efforts but not necessarily greater conversion degrees.18,19,25In other words, there is a limit where greater levels of energy do not correspond to significant increments in the conversion degree or in mechanical properties.17 Mehl17 reported that when decreasing distance between the point of the lamp and the resin (increasing intensity) resistance to flexion was increased to a maximum point, to then decrease. Nevertheless, at all points in time it met with requirements established in the ADA 27 norm, which states that minimum value for flexion resistance must be 50MPa.
The aforementioned reasons underline the existing need to conduct additional studies, where all normspecified properties are included in order to ascertain the influence exerted by the thickness of the cavity wall.
It is equally important to keep in mind that resin overexposure to light activation increases the risk of losing marginal adhesion or causing tooth over-heating.26–33
CONCLUSIONSBased on the aforementioned results obtained in the present research work, it can be inferred that we can polymerize Prime Dent® resin through a 2 to 3mm dental wall, by naturally decreasing light intensity (using the tooth as a material that absorbs energy without modifying the strength of the lamp). This produces a curing depth which is accepted by the norm and exhibits low shrinkage values, which in turn decrease post-operative sensitivity in the patient.
Nevertheless, it is necessary to undertake additional studies such as physical, mechanical and onversion degree studies in order to be able to analyze the infl uence exerted by light intensity on the behavior of the material, and, as a secondary objective, conduct the same studies in other resins in order to ascertain whether they might exhibit the same behavior.
Graduate and Research School, National School of Dentistry, National University of Mexico (UNAM).