












Treatment of mild or moderate Class IIrelationshipscan be possible without extraction of bicuspids with a correct diagnosis. Distalization of upper molars may be used for obtaining a correct Class I relationship between molars and cuspids without bicuspidextractions. Currently, this treatment has become more frequent mainly due to new biomaterials and conceptual changes in mechanical forces. Many authors have designed different appliances to achieve this goals.
El tratamiento de las relaciones clase II ligeras o moderadas se puede llevar a cabo sin la necesidad de extracciones de órganos dentarios siempre y cuando el diagnostico sea correcto. La dista- lización de los molares para tratar de conseguir relaciones Clase I molares y caninas disminuyendo la necesidad de realizar exodon- cias, es cada día más frecuente, los avances en biomateriales y los cambios conceptuales relacionados a la rigidez de las mecánicas han hecho posible que en los últimos años, muchos autores hayan diseñado técnicas diferentes para tratar de alcanzar estas metas.
The appliance enamed pendulum was described in 1992 by Dr. James Hilgers as an appliance aimed at correcting certain malocclusions with minimal help from the patient. Since its introduction the pendulum has undergone numerous changes to make it more comfortable for the patient, making its placement and activation easier, simplifying the design, increasing its stability and increasing its efficacy.
An option for creating space or correcting class II relationships in the maxillary arch is to move the molars distally. The use of intraoral appliances has been developed since the 80's1 as an alternative to extraoral2–6 and removableappliances.7–9
Indication or contraindication for molar distalization is given by the patient's characteristics and the degree of movement intensity that needs to be performed. It is important to bear in mind that due to its own characteristics, mouth opening is performed on the condylar axis, so that if we need to distalize one or several molars we must consider the following effects:
- •
Distalization produces a downwards and backwards mandibular rotation, in a clockwise direction.
- •
It increases facial convexity angle.
- •
It increases anterior facial height, particularly the lower third.
- •
Distalization increases the mandibular plane angle with respect to the base skull.
These effects may be extremely favorable in those patients with deep bite but counterproductive in patients with open bite so these factors have to carefully considered when performing distalization. The facial biotype and the patient's cefalometric features are very important as it is more likely that we produce an open bite in a dolichofacial patient with an open goniacangle than in a brachifacial patient with a closedgoniac angle. Careful study of the characteristics and growth patterns in young patients has to be performed when planning the case.
Indications for performing unilateral or bilateral molar distalization are very specific:10
- •
Class I with crowding and slight or non-severe protrusion.
- •
Dental Class II caused by mesialization of the upper molar due to loss of space either by early loss of the temporary second molar or loss of anchorage during some phase of orthodontic treatment.
- •
When deciding on the extraction of the second permanent molar either by caries or by another cause, with anterior crowding and/or ectopic canine.10
The orthodontist depends on the use of traditionally used devices for molar distalization.11–13 This is the reason why the of use intraoral devices is preferred since they are not dependent on the patient's cooperation.
In recent years interest has been placed in the Hilgers Pendulum (Figure 1) and its variants.14–19 The objective of this appliance is to move the teeth bodily minimizing the risk of root resorption. The fundamental problem is that when activating the pendulum, the insertion of the bars in the lingual boxes of the molars causes the molars to be moved within a result radius of the direction of the force of the TMA spring.

The objective of this case report is to present a treatment option for mild or moderate class II molar discrepancies in which the removal teeth is not a choice.
CASE REPORTMale patient, 13 years of age, who attended the clinic of the Orthodontics Department at the Division of Post-graduate Studies and Research of the Faculty of Dentistry.
Facially, the patient was mesofacial, with a convex profile, a slight nasal hump and competent lips (Figure 2A-C).

Intra-oral analysis revealed a molar class I and canine class II on the right side, a class I molar relationship and a canine class I on the left side, a permanent dentition, an overjet of 5mm, a 4mm overbite and a teeth-basal bone discrepancy of -4mm in the lower arch and of -1mm in the upper arch. The upper and lower dental midlines did not match and there was mild upper and lower crowding (Figure 3A-E).

In the orthopantomographyit may be observed that the patient presents 28 erupted teeth, 4 retained teeth (#18, 28.38 and 48) and a crown-root ratio of 1: 3 (Figure 4).

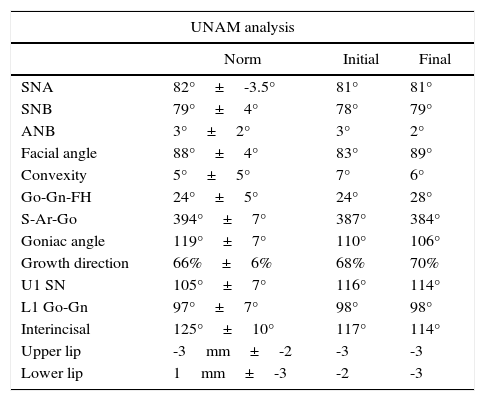
Chepalomterically, the patient was diagnosed as a skeletal class I, proclined and protruded upper incisors, rearward position of the condyle, mildly prominent chin, CCW growth direction (Table IandFigure 5).
Cephalometric data.
| UNAM analysis | |||
|---|---|---|---|
| Norm | Initial | Final | |
| SNA | 82°±-3.5° | 81° | 81° |
| SNB | 79°±4° | 78° | 79° |
| ANB | 3°±2° | 3° | 2° |
| Facial angle | 88°±4° | 83° | 89° |
| Convexity | 5°±5° | 7° | 6° |
| Go-Gn-FH | 24°±5° | 24° | 28° |
| S-Ar-Go | 394°±7° | 387° | 384° |
| Goniac angle | 119°±7° | 110° | 106° |
| Growth direction | 66%±6% | 68% | 70% |
| U1 SN | 105°±7° | 116° | 114° |
| L1 Go-Gn | 97°±7° | 98° | 98° |
| Interincisal | 125°±10° | 117° | 114° |
| Upper lip | -3mm±-2 | -3 | -3 |
| Lower lip | 1mm±-3 | -2 | -3 |

The objectives to be achieved with the treatment plan were: to maintain the profile, maintain molar class I and obtain a bilateralcanine class I, correct overbite and overjet, correct rotations and match the dental midlines.
According to the obtained diagnosisand planned objectives, the treatment plan to perform was: distalization of the upper molars with a pendulum (Figure 6A-C), placement of anchorage (Nance button) (Figure 6-D) no extractions, Edgewise technique 0.017” × 0.025”.
Phase I: alignment and leveling 0.016” ss.
Phase II: midline correction (Figure 7C).
Phase III: bracket repositioning and finishing (Figure 7).
Retention: upper and lower Hawley retainers.


A-D. Molar distalization with a pendulum modified by Dr. Mario Katagiri, Lizie Díaz and Ismael Villa which consists in bands in the first bicuspids with a welded bracket palatally in which a 0.017” × 0.025” stainless steel wire is introduced, circumferential retainers in the second bisupids and TMA springs in the lingual boxes of the upper first molar.
Upon appliance removal a class I molar and canine relationship and centered dental midlines were achieved (Figure 8A-E).

At the end of treatment, Hawley retainers were placed on the upper and lower arches (Figure 9). The cephalometric superimposition shows bodily distalization of the upper molar, retroclination of the upper and lower incisors and rotation of the mandible in a clockwise direction (Figure 10).

 and final tracing (brown). Color image available atwww.medigraphic.com/ortodoncia.")
Superimposition of the initial tracing (blue) and final tracing (brown). Color image available atwww.medigraphic.com/ortodoncia.
The results obtained in this patient suggest that the pendulum is effective in the distalization of upper molars with a distance of 1mm per month using a force of 200 to 250 grams. In the case hereby presented the pendulum was used for 4 months in order to achieve overcorrection of the molar class. The alignment and leveling of the dental arches was performed with round NiTi archwires and subsequently, round stainless steel archwires. Space closure and dental midline correction were achieved with closing loops. Finally, the ideal archwires were placed to perform second and third order movements to provide a correct occlusion. The final treatment time was 3 years and 8 months (Figure 2D-F).
DISCUSSIONThe results obtained in this case report suggest that this pendulum modification is easier to fit and remove from the mouth in comparison with the original pendulum which is welded to bands in the premolars; the modification hereby presented has arms that enter within the bicuspid brackets thus resulting in shorter chair time activation and it is effective for molar distalization with a distance of 1 mm per month.
Byloff and Darendeliler1 reported that the pendulum performs a movement of 1.02mm (+ 0.68mm) per month with an initial strength of 200 to 250 g14,18,19 proving that it is a more effective apparatus in comparison with what was reported by other authors who claim that the use of cervical traction with a force of 250g of each side distalizes molars in 9 to 12 months2,4 and using a force of 680 to 770g on each side, in 6 months.4 With the use of combined traction, high pull and cervical traction, with a force of 1,135 to 1,360g per side, distalization occurs in a period of 6 months depending on patient's cooperation.11
It must be taken into consideration that cervical traction causes more skeletal changes2–4 and that such changes with the pendulum are minimal or none10,15,16,18 as for the intrusion movement that is produced therefore being a good option for clinical use.1,16,18
CONCLUSIONSThe pendulum is a fast and effective method for treating mild or moderate class II malocclusions through distalization of upper molars with dental anchorage thus avoiding premolar extractions.
By the methodology used in this case it was noted that molar distalization was performed in a bodily manner but there was also a slight projection of the anterior teeth which was corrected during closure of the remaining spaces, with which all the objectives were accomplished.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia.