
















At the CEMEV Orthodontics clinic arrive patients who have previously received orthodontic treatment externally and who present different alterations. The objective of this research project was to describe the residual problems that these orthodontic patients have. In order to do this we conducted a review of the clinical records to find the initial diagnosis. 49 clinical charts were reviewed: 75% belonged to female patients with ages between 18 and 30 years. The more frequently found orthodontic problems were: molar class II on the right side, bilateral canine class II, upper midline deviation toward the right in relation to the facial midline and a lower midline deviation to the right, convex profile and upper lip protrusion. It was concluded that most patient's treatment time was two to three years. Dental anomalies were the most frequent problem followed by skeletal issues. Therefore it is important for orthodontic treatment to be performed by a specialist.
A la clínica de ortodoncia del CEMEV llegan pacientes que previamente recibieron tratamiento ortodóncico de manera externa y que presentan distintas alteraciones. El objetivo de este trabajo fue describir los problemas ortodóncicos residuales que tienen estos pacientes. Para ello se realizó una revisión de expedientes clínicos para establecer el diagnóstico con el cual acuden. Se revisaron 49 expedientes 75% género femenino, con edades entre los 18 y 30 años, encontrando con mayor frecuencia los problemas ortodóncios; clase II molar del lado derecho, clase II canina bilateral, desviación de la línea media superior hacia la derecha en relación a la línea media facial y la inferior desviada al lado derecho en relación a la línea media inferior, perfil convexo y proquelia labial superior. Se concluye que los pacientes tuvieron un tratamiento entre los dos años y tres años, siendo las alteraciones dentales las más frecuentes seguidas de las esqueléticas; por ello es importante que el tratamiento sea realizado por un especialista.
Orthodontic treatment is an integral process that includes both skeletal and dental problems and that has as objectives periodontal health, functional occlusion, stability and dentofacial aesthetics.1
The vast majority of patients who seek orthodontic consultation do so purely on the basis of aesthetic needs and less frequently because of functional alterations.2,3
Due to the existing demand of the population for orthodontic treatment there are many dentists without proper training who perform this procedure; therefore their approach is dental only (alignment, leveling and crowding correction) leaving aside or completely ignoring the existence of a problem of skeletal origin.
Mistakes occur mainly due to an omission in the diagnosis and in the worst cases, due to the dentist's total lack of knowledge.4
The Orthodontics Clinic of the Center of Medical Specialties of the State of Veracruz receives a considerable amount of patients who seek orthodontic treatment for the second or more times. One of the main reasons is that their previous treatment was finished with unsatisfactory results.
The present research project aimed to describe the residual orthodontic problens of patients who were treated outside the Orthodontics Clinic of the CEMEV.
METHODSClinical charts of patients with re-treatments belonging to the archive of the Hospital and the Orthodontics Clinic were reviewed. The clinical charts of patients of any age and gender who previusoly received orthodontic treatment outside the clinic of Orthodontics of CEMEV, who had fixed appliances and who wished to continue their treatment were included. The files that did not have orthodontic studies, that were incomplete or belonged to patients who did not accept surgery were excluded.
The variables considered for the recollection sheet were: age, gender, socioeconomic status, previous treatment duration, canine relationship, molar relationship, crossbite, overjet, overbite, facial features and skeletal relationship.
RESULTSForty-nine clinical charts were selected which represented the patients who received treatment outside the Orthodontics Clinic of the CEMEV.
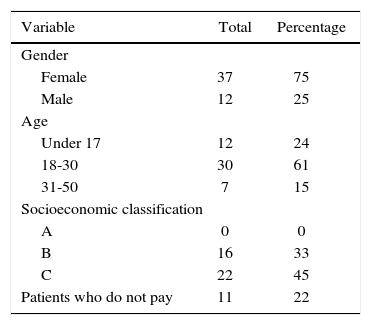
Out of 40 clinical records 75% represented female patients, 61% were between 18 and 30 years old and treatment time was 2 years or less in 67% of the population. The predominant socioeconomic classification was type C (45%) (Table I).
The most frequent intraoral clinical features on the right side were: molar class II with 33% followed by class I with 29%; 27% corresponded to class III and 11% was non- assessable. On the left side, molar class I was predominant with 35%, followed by class II with 27%, class III with 24% and non- assessable molar class was 14 per cent (Figure 1).

In relation to canine class on the right side, 37% were canine class II, canine class I was 28%, 22% were canine class III and 13% were non-assessable. On the left side canine class II was the most frequent likewise with 32%, followed by class I with 28% and 26% for Class III. 14% was non-assessable (Figure 2).

Twenty percent for the sample presented an overjet of less than 2mm, 39% an overjet of 2-3mm; 29%, 3 to 4mm, 10% had more than 4mm and 2% was non- assessable (Figure 3).

Vertical overbite was represented by 18% of deep bites, 14% open bites, 65% with a normal overbite and 3% was non-assessable (Figure 4).

Fifty-five percent did not present cross bite, 20% had an anterior cross bite, 14% a bilateral posterior cross bite and 11% had a unilateral posterior cross bite (Figure 5).

Regarding telescopic bites, they were present in a unilateral form in 2% of the population while 98% did not have one (Figure 6).

Upper dental midline deviation in relation to the facial midline was present in 57% towards the right side, 37% was deviated to the left side, 4% was noncoincident and 2% was non-assessable. Regarding the lower dental midline, 47% was deviated to the right side, 33% was deviated to the left side, 16% did not coincide with the facial midline and 4% was non- assessable (Figure 7).

The most frequently absent teeth were first premolars (63%), incisors (10%), second premolars (6%), a total of 8% for first and second premolars and 13% did not present dental absences (Figure 8).

Based on radiographic analysis it was determined that the predominant skeletal Class was Class I (43%) followed by class II with 39% and lastly, class III with 18% (Figure 9). Likewise, regarding growth direction 41% had vertical growth, 30% neutral and 29% horizontal growth (Figure 10).


Extra oral analysis revealed that 67% of the patients had a convex profile, 12% a straight profile and 27%, a concave profile (Figure 11).

Eighty-two percent presented a good malar projection and 18% had malar projection deficiency (Figure 12).

In Figure 13, 54% presented a neutral smile, 36% a positive smile, 8% gummy smile. 2% of the smiles were non-assessable and no case presented a negative smile.

Finally, regarding upper and lower lip projection: the upper was within normal values in 71% of the cases, 24% presented lip protrusion and in 5% of the cases a retruded upper lip was found. Regarding the lower lip: 37% were within normal values, 35% presented procheilia and in 28% of the cases, retrusion was found (Figure 14).
DISCUSSION
Orthodontics is much more than teeth straightening. It consists in identifying the etiology of the malocclusion, as well as defining the skeletal, dental, facial and functional relationships which play a fundamental role in the diagnosis and treatment plan.5,6
The obtained results are difficult to compare due to the lack of similar studies. What may be found in the literature is the type of malocclusion that certain populations present without specifying if the patients were retreated cases. As the authors Dominguez, Towers and Galvez mentioned in the article «When to refer to an orthodontist»: malocclusion prevalence and the distribution of its different types vary according to race and ethnicity. Skeletal remains that have been found indicate that the current prevalence of malocclusion is higher than that of 1,000 years ago. In Venezuela and the United States the most frequent skeletal class was class I, followed by class II and finally, class III. In Spain the predominant skeletal class was class II.
Other studies that have been conducted to determine parameters for defining the type of malocclusion could not be compared with the present study since they were performed in an ethnic group other than Mexican, for example the study by Dr. Rosenblum in 1995, McNamara in 1981, Karlens in 1994 to mention a few.7 In Mexico the studies that have been conducted focused on the prevalence of malocclusions in the general population, without determining if the patients had previous treatments or not.
Through the results obtained in this research, patients with molar class I on the left side and class II on the right; with canine class II, normal overbite and overjet, vertical growth, good malar projection, without skeletal alterations and with dental extractions mainly of first premolars were determined as noncomplicated clinical cases since they were near or within orthodontic normal values.
Hence the importance of diagnosis not only in orthodontics but also in other specialties in order to prevent, intercept and correct dento-skeletal problems through the use of useful diagnostic items such as x-rays and study models.
This research leads to determine that many questions remain to be answered, including what was the reason for initial consultation? What were the conditions in which the patients began treatment for the first time? Was the initial treatment influenced by economic factors? These questions may be answered through future research and may help the general population and the guild to a better understanding of the current situation of Orthodontics.
CONCLUSIONSIt may be concluded that many of the patients with previous orthodontic treatments who attend the CEMEV are patients in a range of age between 18 and 30 years, with low socio-economic status and whose previous treatment time was 2 years or less. The majority of these patients also had poorly diagnosed dento-skeletal malocclusions followed by a nonsuccessful treatment plan that required the placement of fixed appliances once more in order to resolve the patient's problem.
It was determined that the cases attended by the CEMEV were cases that presented problems mainly at a dental level and in a lower percentage, at a skeletal level that with proper diagnosis and orthodontic therapy could have been adequately solved.
Graduate.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia