








The objective of this study was to determine the cephalometric discrepancy of some reference planes and angles in relation to the natural head position. 78 patients were admitted at the Orthodontic Service of the Mexico Children's Hospital and 2 lateral X-rays were taken from the skull of each patient. The first radiograph was in natural position. The patient positioned his head in a relaxed way looking into the horizon, with slightly separated legs, arms resting at the sides of the body, lips at rest. The second radiograph (assisted) was taken with the above mentioned parameters and without the olives pressing the external auditory meatus. A 4×8cm to 1.5 m mirror was given to each patient of so that they could look into it with his or her pupils focused in the eye center and a plummet placed on the chassis of the plate (representing the true vertical) plus a profile photograph with the same indications. The measurements in both plates were traced, measured and compared. We considered the random error with a standard deviation of 0.4mm, Houston's.1
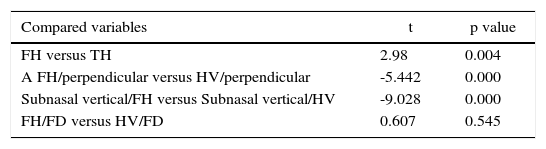
ResultsWe found a statistically significant difference (p=0.004) between the Frankfort plane and the true horizontal and (p < 0.005) between nasion perpendicular to point A and between subnasal vertical to pg’ in relation to the Frankfort plane and to the true horizontal unlike facial depth (p=0.545).
El propósito del estudio es determinar la discrepancia cefalométrica de algunos planos y ángulos de referencia con relación a la posición natural de la cabeza. Seleccionamos los 78 pacientes que ingresaron al Servicio de Ortodoncia del Hospital infantil de México en el 2004, tomamos 2 telerradiografías por cada paciente. La primera con postura natural, el paciente posicionó su cabeza de manera relajada mirando hacia el horizonte, piernas ligeramente separadas, los brazos al costado del cuerpo, labios en reposo. La segunda (asistida) con los mismos parámetros mencionados sin que las olivas presionaran el conducto auditivo externo, adicionándole un espejo de 4×8cm a 1.5 m para que el paciente mire con sus pupilas en el centro del ojo y una plomada colocada sobre el chasis de la placa (representando la vertical verdadera) más una fotografía de perfil con las mismas indicaciones. Se trazaron, midieron y compararon ambas placas. Consideramos el error aleatorio con una desviación estándar de 0.4mm según Houston.1
ResultadosEncontramos diferencias estadísticamente significativas (p=0.004) entre Frankfort y la horizontal verdadera y (p < 0.005) en nasión perpendicular/punto A y vertical a subnasal/pg’ en relación al plano de Frankfort y a la horizontal verdadera a diferencia de la profundidad facial (p=0.545).
The natural head position (NHP) is defined as an innate, physiological and reproducible position of the head obtained when the patient is in a relaxed position, sitting or standing, looking into the horizon or into an external reference point (a mirror, a mark on the wall) at eye level. It is known as the auto balance head position or natural orientation. It is important to distinguish between natural position and natural posture since posture is used to study the relationship between morphology and function, usually defined as a position in which the patient is standing keeping his or her head on its own balance in a non-strained position for a specific activity at some time.2–14
The concept of natural head position is not new. Leonardo da Vinci (1452-1519) and Albrecht Durer (1471-1528) used horizontal and vertical lines on paintings of models positioned in a «natural pose» so that the artistic and scientific replica of human heads was secured. In the XIX century, Von Baer, Wagner and Broca defined the natural posture of the head as the subject's posture when they are standing with their horizontal visual axis.4
Currently, lateral radiographs are one of the most important diagnosis elements and auxiliaries. With them cephalometry, which is a study that measures the skull, the face, maxillary bones and dental positions, is performed and helps the orthodontist in obtaining a more profound knowledge of the structures on which he or she works by visualizing, like in a showcase, what lies beneath the soft tissues.15,16
The Frankfort Horizontal Plane (FHP) is one of the most used planes in cephalometry. It was adopted with the purpose of orienting the skull in a similar way to the natural head position. In cephalometric practice this plane presents two difficulties: a) Problems in locating accurately its two reference points, especially Porion, b) The operator assumesthat the Frankfurt plane is parallel to the true horizontal plane which does not occur in many individuals, there have been observed differences of up to 10 degrees and even more.17 Arnett mentions:18 no one walks with the Frankfort plane parallel to the ground and we can have a patient in natural head position but with the Frankfurt Plane inclined upwards or downwards (Figure 1).

The Frankfort plane and others have been criticized by clinicians and investigators because of their lack of required stability but none of the suggested options has a rigorous certainty.15 Measurements such as Sella-Nasion- Point A, Maxillary Depth, Facial Depth, etc. do not correlate or correspond to the patient's real malocclusion.2,4,19–26
Sometimes we observe that lateral radiographs show us that the patient's head is inclined upwards or downwards without respecting the Natural Head Position concept thus altering the position of some cephalometric landmarks such as Pogonion, Menton, etc. useful for measuring a protrusion or prognathism (Class III) or a mandibular retrusion that might suggest a skeletal Class II due to mandibular deficiency and the real appreciation of the patient's profile is lost.
Every time there is doubt regarding the correct position of the head in the lateral radiograph there is the possibility of controlling this problem by using the profile photograph.2,20,25
Every successful treatment is related directly to a correct diagnosis, the correct position of the lateral radiograph will help us obtain a reliable diagnosis for the precise application of the therapeutic measures.
The importance of this study lies in comparing two methods for taking lateral radiographs so that the clinician is able to obtain or achieve precise and reliable cephalometric tracings, increasing the reliability of cephalometry and thus obtaining a better diagnosis.
MethodsThe design of this study was transverse and comparative.
All 9 to 15-year-old patients that attended during 2004 to the Orthodontic Service were selected, being a total of 78 patients (sample available in the 2004 annual records) (Figure 2).

Two lateral head films were taken by the same operator (radiology technician) to each one of the 78 patients with the Soreedex cephalostat from the Orthodontic Service of the Children's Hospital of Mexico Federico Gomez, taking into consideration the following:
The first radiograph (natural posture) was taken asking the patient to position his or her head inside the cephalostat in a relaxed manner, looking into the horizon, legs slightly spread, arms at the sides of the body, lips at rest (Figure 3).

The second radiograph (assisted) was taken with a Natural Head Position. The patient was asked to position his or her head inside the cephalostat without the olives pressuring the hearing meatus or the auricular cartilage, we placed the patient sideways and in a natural position, at eye level we placed at 1.5 m a 4×8cm mirror so that the patient could observe his or her pupils at the center of the mirror. We also placed a lead chain over the radiographic plate's chassis thus obtaining a true vertical reference and we marked the tip of the nose and the soft pogonion (Figure 4).

Subsequently we took a photograph to confirm and obtain more precise data of the NHP taking under consideration the same indications for the radiograph at NHP. In front of the patient a lead chain was placed and so we obtained a true vertical line in the photograph and we traced a line from the tip of the nose to the soft pogonion. Then we continued that line until it reached the true vertical line, forming an angle which we transferred to the radiograph (Figure 5).4,6,16
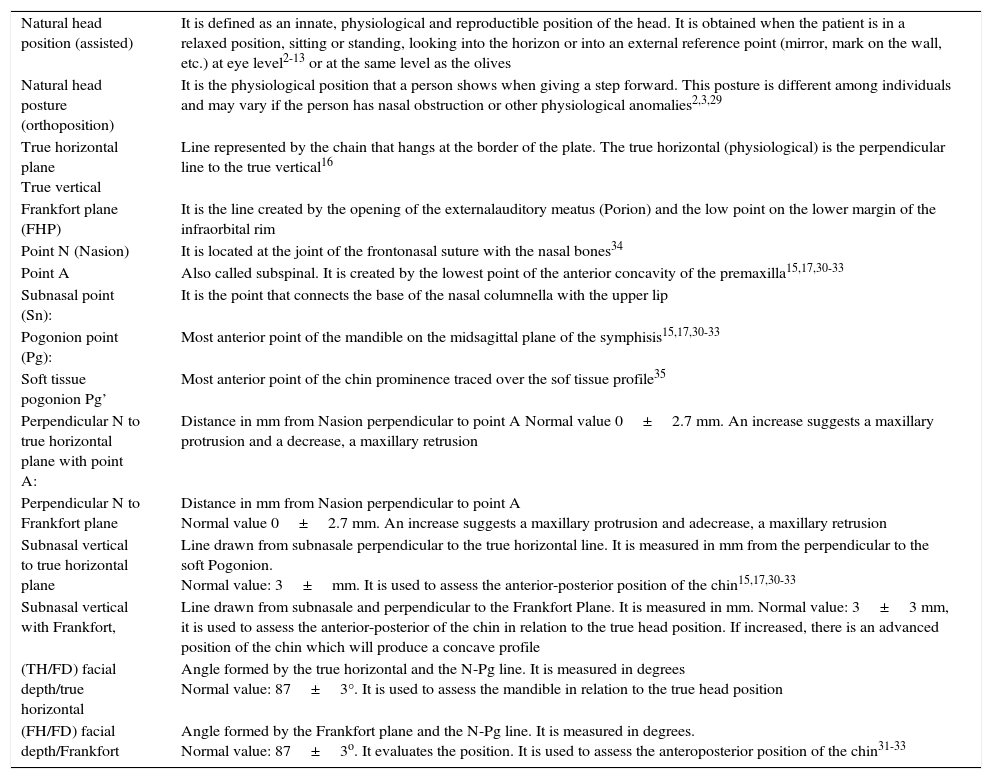
Concepts used in the study.
| Natural head position (assisted) | It is defined as an innate, physiological and reproductible position of the head. It is obtained when the patient is in a relaxed position, sitting or standing, looking into the horizon or into an external reference point (mirror, mark on the wall, etc.) at eye level2-13 or at the same level as the olives |
| Natural head posture (orthoposition) | It is the physiological position that a person shows when giving a step forward. This posture is different among individuals and may vary if the person has nasal obstruction or other physiological anomalies2,3,29 |
| True horizontal plane True vertical | Line represented by the chain that hangs at the border of the plate. The true horizontal (physiological) is the perpendicular line to the true vertical16 |
| Frankfort plane (FHP) | It is the line created by the opening of the externalauditory meatus (Porion) and the low point on the lower margin of the infraorbital rim |
| Point N (Nasion) | It is located at the joint of the frontonasal suture with the nasal bones34 |
| Point A | Also called subspinal. It is created by the lowest point of the anterior concavity of the premaxilla15,17,30-33 |
| Subnasal point (Sn): | It is the point that connects the base of the nasal columnella with the upper lip |
| Pogonion point (Pg): | Most anterior point of the mandible on the midsagittal plane of the symphisis15,17,30-33 |
| Soft tissue pogonion Pg’ | Most anterior point of the chin prominence traced over the sof tissue profile35 |
| Perpendicular N to true horizontal plane with point A: | Distance in mm from Nasion perpendicular to point A Normal value 0±2.7 mm. An increase suggests a maxillary protrusion and a decrease, a maxillary retrusion |
| Perpendicular N to Frankfort plane | Distance in mm from Nasion perpendicular to point A Normal value 0±2.7 mm. An increase suggests a maxillary protrusion and adecrease, a maxillary retrusion |
| Subnasal vertical to true horizontal plane | Line drawn from subnasale perpendicular to the true horizontal line. It is measured in mm from the perpendicular to the soft Pogonion. Normal value: 3±mm. It is used to assess the anterior-posterior position of the chin15,17,30-33 |
| Subnasal vertical with Frankfort, | Line drawn from subnasale and perpendicular to the Frankfort Plane. It is measured in mm. Normal value: 3±3 mm, it is used to assess the anterior-posterior of the chin in relation to the true head position. If increased, there is an advanced position of the chin which will produce a concave profile |
| (TH/FD) facial depth/true horizontal | Angle formed by the true horizontal and the N-Pg line. It is measured in degrees Normal value: 87±3°. It is used to assess the mandible in relation to the true head position |
| (FH/FD) facial depth/Frankfort | Angle formed by the Frankfort plane and the N-Pg line. It is measured in degrees. Normal value: 87±3o. It evaluates the position. It is used to assess the anteroposterior position of the chin31-33 |

The radiographs were taken at 70 KVp to secure the penetration of the bone structures and the recommended exposure time was 1 second.28 The radiographs were then developed with Kodak products. The cephalometric tracing was performed (Figure 6). Prior to the tracing, the observer was calipered by one of the specialists of the department who is considered an expert in the area with vast clinical experience and an opinion leader. The tracing papers were placed over the radiographs and the following cephalometric measurements were compared:
Ethics
In agreement with the Hospital Ethics Committee's Guidelines, the patients were asked to sign an informed consent. A written authorization by the patient's parents was obtained, a photograph of which is published in this paper.
StatisticsMeans and standard deviations of each one of the variables was obtained. Both study groups were compared with a «t» Student test. The random mistake was considered with a standard deviation of 0.4mm. All calculations were performed with the statistical program SPSS 12.0 version.
ResultsWe found statistically significant differences (p=0.004) between Frankfort and the true horizontal and (p < 0.005) in the perpendicular nasion/point A and the subnasal vertical/Pg in relation to the Frankfort plane and the true horizontal line unlike the facial depth (p=0.545).
The average difference between FH and the tue horizontal by gender was 3.18 degrees in female patients and 4.416 degrees in male patients.
DiscussionDue to the significant variation found in the Frankfort plane when used as an intracranial reference, an extracranial line of reference, the true horizontal line has been used.2,5,7,21,36,37 However the minor importance that the specialized text publications have given to an adequate head orientation draws the attention. For the beforehand explained reason we took 146 lateral headfilms, half in natural head posture on and the other half in natural head position with the aim of determining the discrepancy in the cephalometric tracings and finding a statistical relationship.
In the patient's study sample we only found 5 patients in whom Frankfort was parallel to the true horizontal line thus resulting in a non-significant statistical difference.
In our results we found that there is a 3.75 degree difference with a statistical difference of p=0.004 between the Frankfort plane and the true horizontal, result that resembles what investigators such as Cooke mentioned in his study performed on Chinese children where he found a difference of 5.2 degrees in boys and 4degrees in girls.27 Bjerin24 mentions that the difference between FHP and TH is of 4.6 degrees. The result of the present study agrees in relation to gender with a more significant difference in males.
In the study performed by Lundström et al20 on 79 British children, they found statistically significant differences for both genders in the angle formed by the Frankfort plane with the true horizontal line in relation to the natural head position, where the difference was 2.6 degrees less in boys and for girls it was 4.1 degrees. In our global sample the discrepancy was bigger in males with an average difference of 4.416 degrees and 3.18 degrees respectively.
Several investigators2,4,19–23,25,26 have observed that the measurements taken from planes such as SNA, maxillary depth, facial depth, etc. do not reflect the patient's real malocclusion. We found that there is variation between FHP and THL with differences or discrepancies in the studied cephalometric tracings where the subnasal vertical line, perpendicular N to point A was statistically significant (p=0.545) (Table II).
In this study there were 9 patients with lip palatal sequel and 69 non-affected patients diagnosed as «healthy» with an average per diagnosis between FH and the true horizontal line of 3.7464 degrees in healthy patients and 3.7778 degrees in patients with lip-palate sequel.
I specially would like to thank Dr. Alfonso Reyes López, Luis Alberto Gaitán, Guillermo Oropeza and Antonio Fernandez for participating as science counselors and critical reviewers of this study, to the Children's Hospital of Mexico for offering me financial support and material.