






Evaluate the usefulness of the dental method of Carrea to estimate the height in Mexican population.
Materials and methodsAnalytical, correlational and cross-sectional study in 2 cadaveric Mexican populations. Sample: 56 bodies, 32 of Veracruz and 24 of the Federal District. In each corpse 4 morphometric measurements were performed, of which 5 derivatives were obtained. Statistical analysis: (1) mean and standard deviation (SD) was calculated; (2) for sex, t-Student and Levene tests for comparison of means and SDs were used; (3) to calculate the variability between Federal District and Veracruz, principal component analysis was made; (4) the heights, real, minimum, average and maximum were compared by univariate ANOVA, and (5) a Pearson correlation analysis between actual and minimum heights was performed.
ResultsNo differences were found between the 2 cadavers samples studied, neither between real and minimum height in either group: Federal District, real height (172.08±6.53cm) and minimum height (171.35±7.81cm) (P>.05); Veracruz, real height (167.5±5.77cm) and minimum height (166.50±6.36cm) (P>.05), having that the correlation between real height and the minimum height is advisable for both samples, Federal District (r=.79, P=.000), Veracruz (r=.82, P=.000) and overall (r=.83, P=.000).
ConclusionsThe dental Carrea's method, using the minimum height reference, is an excellent estimate of the actual size in Mexican corpses.
Determinar la efectividad del método odontológico de Carrea para estimar la talla real de cadáveres mexicanos.
Material y métodosEstudio analítico, correlacional y transversal en 2 poblaciones mexicanas cadavéricas. Muestra: 56 cadáveres, 32 de Veracruz y 24 del Distrito Federal. En cada cadáver se realizaron 4 mediciones morfométricas, de las cuales se obtuvieron 5 derivadas. Análisis estadístico: 1) se calcularon media y desviación estándar (DE); 2) para sexo, se utilizaron las pruebas t Student y de Levene para comparación de medias y DE; 3) para calcular la variabilidad entre muestras, se realizó un análisis de componentes principales; 4) las tallas real, mínima, máxima y promedio se compararon mediante un ANOVA unifactorial y 5) se realizó un análisis de correlación de Pearson entre las tallas real y mínima.
ResultadosNo se encontraron diferencias entre las 2 muestras de cadáveres estudiadas ni entre las tallas real y mínima en ninguno de los 2 grupos: Distrito Federal, talla real (172,08±6,53cm) y talla mínima (171,35±7,81cm) (p > 0,05); Veracruz, talla real (167,5±5,77cm) y talla mínima (166,50±6,36cm) (p > 0,05). Se obtuvo que la correlación entre la talla real y la mínima es adecuada tanto para la muestra del Distrito Federal (r=0,79; p=0,000) como para la de Veracruz (r=0,82; p=0,000), así como en conjunto (r=0,83; p=0,000).
ConclusionesEl método odontológico de Carrea, utilizando la talla mínima como referencia, es un excelente estimador de la talla real en cadáveres mexicanos.
The identification of persons is an extremely important task in forensic medicine, and forensic dentistry or odontology is a speciality that plays a key role in this process, particularly in the identification of deceased persons.1
In many cases, forensic identification can be hindered by aspects related to the process of death, particularly when the victims are disfigured to the point that the only biological remains available for study are dental tissues.2 Body identification will require analysing the data or identifying biological characteristics, first to determine if the teeth are human and then to determine the age, sex, and predominant racial identity. Depending on the dental and maxillary features, further information probably can also be provided, for instance, on the individual's real height (T_REAL), illnesses, and lifestyle, making it possible to individualise the subject studied in more detail, thus allowing subsequent identification.1
Real height determination is an important part of forensic medicine and, in particular, of post-mortem identification processes. When the bodies have been significantly destroyed or decomposed due to the passage of time or due to physical and chemical agents, it may be difficult to determine information such as height. In such cases, the individual's identity may be determined more easily by studying the dental tissues, along with the anthropological structures and biological and genetic tests.3
One of the data points sought as part of post-mortem identification techniques is the real height of the individual. This information is essentially obtained through anthropometric techniques used in physical anthropology, although other techniques may also be used for this purpose in forensic odontology.4
In 1920, Juan Ubaldo Carrea and Zelaschi were awarded doctoral degrees in Argentina for their thesis entitled “Odontometric studies”, which describes an odontometric technique to estimate real human height.5 Carrea's index contributed not only to forensic odontology, but his legacy has also influenced prosthodontics, maxillofacial surgery, orthodontics, and oral anaesthetics through the technique that bears his name.6
In South America, tests were later performed on a modified version of the Carrea method. One of these tests consisted of measuring upper primary teeth7 instead of lower permanent teeth, as recommended by the author. This particular study found that real height was correctly estimated in 57.5% of cases with ±5cm and in 97.0% with ±10cm and, therefore, the authors concluded that real height estimation should be supplemented with other methods.7
Carrea's method describes specific measurements of its technique that can be used to obtain 2 measurements: arc and chord. The first corresponds to maximum height (T_MAX) and the second to minimum height (T_MIN), which can be used to obtain the average height (T_AVG).8 To obtain these measurements, the method uses the following formulas:
where

- -
Chord is the distance in mm between the mesial surface of the lower central incisor and the distal surface of the lower canine.
- -
Arc is the sum of the mesiodistal diameters of a lower central incisor, a lower lateral incisor, and a lower canine, all on the same side, in mm.9
In Mexico, body identification is a forensic challenge. An investigation performed by Mexican journalists revealed that a total of 3662 unidentified bodies were sent to state-operated common graves over an 18-month period between January 2012 and July 2013. In the 6-year period from 2006 to 2012, a total of 24,102 persons were sent to common graves.10 It is not uncommon for the only biological material available to be the craniofacial complex, making it necessary to have methodological resources validated in the Mexican population to obtain basic anthropometric measurements for cadaver identification, in which height determination plays an important role. Consequently, the aim of this study was to determine the effectiveness of the Carrea method in estimating the real height of Mexican cadavers.
Materials and methodsWe conducted a cross-sectional, correlational, analytical study between January 2013 and January 2014 at 2 forensic medical services, using 2 measurement techniques (1 odontometric and 1 anthropometric) to obtain 4 morphometric parameters, from which 5 additional parameters were obtained using the Carrea formulas.
SampleFollowing submission of the protocol to the Research and Ethics Committees of the various participating sites, the study was undertaken at 2 locations, namely, the forensic medical service of the Directorate of Expert Services in the city of Xalapa (Veracruz) and the forensic medical service of the Superior Court of Justice in the Federal District. Thirty-two individuals were studied at the first of these sites (27 men and 5 women) and 24 at the second (21 men and 3 women), with a total population of 56 individuals. The selection criterion used was convenience, i.e. non-probability, sampling (consecutive autopsies).
Inclusion criteriaThe study included whole male and female cadavers brought to the forensic medical services during the study periods, whether as a fresh cadaver or with maximum putrefaction and discolouration, that had their 6 lower anterior teeth, or at least 1 central incisor, 1 lateral incisor, and 1 canine on the same side and with incisor wear not higher than Gerasimov grade 3.11
Exclusion criteriaThe study excluded cadavers in a condition of preservation that hindered measurement of the real height, bodies with mutilation or injuries that prevented measurement of the real height, and bodies with mandibular or dental trauma that did not allow dental measurements.
ProcedureThe sex and the age range were determined, with sex determined by identifying the external genitalia during a physical examination of the cadaver. The age range of the adults included was 25–60 years, with the range established from the age registered in the ministry for each cadaver. All cadavers were subject to full forensic examination, and the age of unidentified subjects was estimated by the medical and anthropological staff of the 2 institutions. Once the cadaver's sex and age was established, the following procedures were performed: the lower lip of the cadaver was retracted and, once the side was selected, the calliper was held and the measurements were made. We measured the lower central incisor, lower lateral incisor, and lower canine corresponding to the same side, whether right or left (Fig. 1). A measurement example for the mesiodistal diameter of a lower lateral incisor is shown in Fig. 2. If the dental tissues are not articulated and in their functional anatomical position, the chord measurement cannot be determined; for this reason, Carrea's method establishes a variant, in which the arc result is multiplied by 0.954.8,9 The real height was obtained from the cephalocaudal measurement; for this, the cadaver was placed in dorsal decubitus position to the extent possible, then a wooden wedge was placed at the vertex, parallel to the Frankfurt plane and perpendicular to the longitudinal axis of the body, and another wedge was placed in the plantar region at the heel. Lastly, the distance between the wedges was measured with a measuring tape.12 Each measurement was recorded in the draft manuscript for subsequent electronic storage and analysis using Carrea's method. The measurements were weighted under the decimal metric system, using millimetres for dental measurements and centimetres for heights.


The information was processed using the IBM-SPSS statistical package, version 22. The statistical analyses included the following: (1) the mean and standard deviation (SD) were calculated for each of the 9 measurements (by sex and state); (2) the Student t-tests (comparison of means) and Levene test for homogeneity (comparison of variances) were used for sex; (3) the main components were analysed using the parameters of sex, arc, and chord to calculate variability between cadavers in the Federal District and Veracruz states; (4) the real, minimum, maximum, and average heights were compared by one-factor ANOVA, and (5) a Pearson correlation analysis was performed to compare the real and minimum heights. A p value<0.05 was considered significant.
ResultsA total sample of 56 cadavers was studied: 32 in the state of Veracruz (28 men, 5 women) and 24 in the Federal District (21 men, 3 women). The data collected were grouped by sex, age range, and morphometric values.
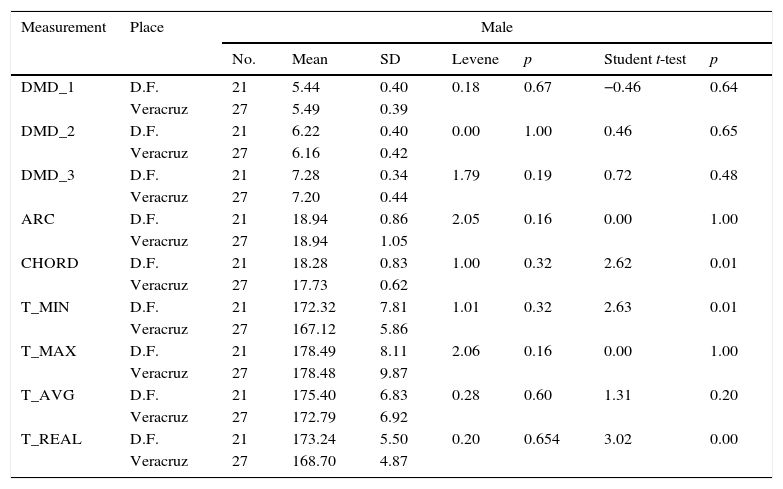
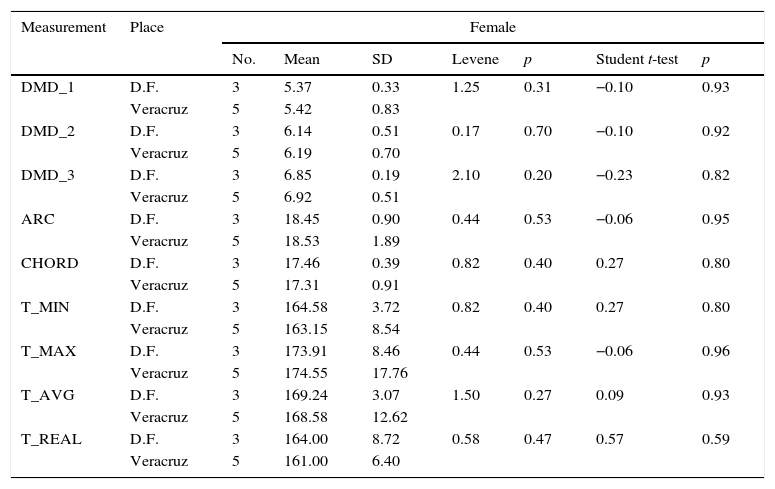
Tables 1 and 2 list the means, SDs, and results obtained from the Levene test for homogeneity and the Student t-test for the variables studied in male and female cadavers.
Distribution and comparison of 9 study parameters in male cadavers using the Levene test for homogeneity and the Student t test.
| Measurement | Place | Male | ||||||
|---|---|---|---|---|---|---|---|---|
| No. | Mean | SD | Levene | p | Student t-test | p | ||
| DMD_1 | D.F. | 21 | 5.44 | 0.40 | 0.18 | 0.67 | −0.46 | 0.64 |
| Veracruz | 27 | 5.49 | 0.39 | |||||
| DMD_2 | D.F. | 21 | 6.22 | 0.40 | 0.00 | 1.00 | 0.46 | 0.65 |
| Veracruz | 27 | 6.16 | 0.42 | |||||
| DMD_3 | D.F. | 21 | 7.28 | 0.34 | 1.79 | 0.19 | 0.72 | 0.48 |
| Veracruz | 27 | 7.20 | 0.44 | |||||
| ARC | D.F. | 21 | 18.94 | 0.86 | 2.05 | 0.16 | 0.00 | 1.00 |
| Veracruz | 27 | 18.94 | 1.05 | |||||
| CHORD | D.F. | 21 | 18.28 | 0.83 | 1.00 | 0.32 | 2.62 | 0.01 |
| Veracruz | 27 | 17.73 | 0.62 | |||||
| T_MIN | D.F. | 21 | 172.32 | 7.81 | 1.01 | 0.32 | 2.63 | 0.01 |
| Veracruz | 27 | 167.12 | 5.86 | |||||
| T_MAX | D.F. | 21 | 178.49 | 8.11 | 2.06 | 0.16 | 0.00 | 1.00 |
| Veracruz | 27 | 178.48 | 9.87 | |||||
| T_AVG | D.F. | 21 | 175.40 | 6.83 | 0.28 | 0.60 | 1.31 | 0.20 |
| Veracruz | 27 | 172.79 | 6.92 | |||||
| T_REAL | D.F. | 21 | 173.24 | 5.50 | 0.20 | 0.654 | 3.02 | 0.00 |
| Veracruz | 27 | 168.70 | 4.87 | |||||
ARC: (DMD_1+DMD_2+DMD_3); CHORD: distance between the mesial edge of the central incisor and the distal border of the lower canine; D.F.: Federal District; DMD_1: mesiodistal diameter of the lower central incisor; DMD_2: mesiodistal diameter of the lower lateral incisor, DMD_3: Mesiodistal diameter of the lower canine; T_MAX: maximum height obtained by the Carrea method; T_MIN: minimum height obtained by the Carrea method; T_AVG: average height between T_MAX and T_MIN; T_REAL: actual height of the sample.
Distribution and comparison of 9 study parameters in female cadavers using the Levene test for homogeneity and the Student t-test.
| Measurement | Place | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| No. | Mean | SD | Levene | p | Student t-test | p | ||
| DMD_1 | D.F. | 3 | 5.37 | 0.33 | 1.25 | 0.31 | −0.10 | 0.93 |
| Veracruz | 5 | 5.42 | 0.83 | |||||
| DMD_2 | D.F. | 3 | 6.14 | 0.51 | 0.17 | 0.70 | −0.10 | 0.92 |
| Veracruz | 5 | 6.19 | 0.70 | |||||
| DMD_3 | D.F. | 3 | 6.85 | 0.19 | 2.10 | 0.20 | −0.23 | 0.82 |
| Veracruz | 5 | 6.92 | 0.51 | |||||
| ARC | D.F. | 3 | 18.45 | 0.90 | 0.44 | 0.53 | −0.06 | 0.95 |
| Veracruz | 5 | 18.53 | 1.89 | |||||
| CHORD | D.F. | 3 | 17.46 | 0.39 | 0.82 | 0.40 | 0.27 | 0.80 |
| Veracruz | 5 | 17.31 | 0.91 | |||||
| T_MIN | D.F. | 3 | 164.58 | 3.72 | 0.82 | 0.40 | 0.27 | 0.80 |
| Veracruz | 5 | 163.15 | 8.54 | |||||
| T_MAX | D.F. | 3 | 173.91 | 8.46 | 0.44 | 0.53 | −0.06 | 0.96 |
| Veracruz | 5 | 174.55 | 17.76 | |||||
| T_AVG | D.F. | 3 | 169.24 | 3.07 | 1.50 | 0.27 | 0.09 | 0.93 |
| Veracruz | 5 | 168.58 | 12.62 | |||||
| T_REAL | D.F. | 3 | 164.00 | 8.72 | 0.58 | 0.47 | 0.57 | 0.59 |
| Veracruz | 5 | 161.00 | 6.40 | |||||
ARC: (DMD_1+DMD_2+DMD_3); CHORD: distance between the mesial edge of the central incisor and the distal border of the lower canine; D.F.: Federal District; DMD_1: mesiodistal diameter of the lower central incisor; DMD_2: mesiodistal diameter of the lower lateral incisor, DMD_3: Mesiodistal diameter of the lower canine; T_MAX: maximum height obtained by the Carrea method; T_MIN: minimum height obtained by the Carrea method; T_AVG: average height between T_MAX and T_MIN; T_REAL: actual height of the sample.
In the multivariable analysis, an analysis of the main components showed no significant differences between the cadaver populations studied according to state (Fig. 3).

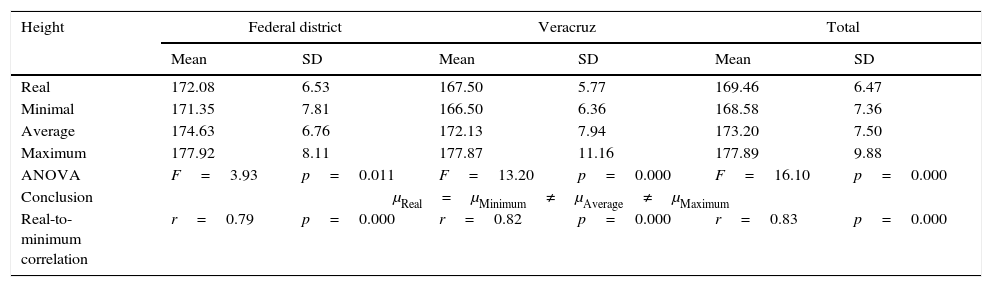
Table 3 contains information on the one-factor ANOVA for the average heights (real, minimum, average, and maximum) and the correlation between the real and minimum heights. A comparison of the real and minimum heights showed no significant differences in either group: 24 cadavers from the Federal District, T_REAL (172.08±6.53cm and T_MIN (171.35±7.81cm); 32 cadavers from Veracruz, T_REAL (167.5±5.77cm) and T_MIN (166.50±6.36cm).
One-factor analysis of variance between the height averages (real, minimum, average, and maximum) and the correlation between the real and minimum heights.
| Height | Federal district | Veracruz | Total | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Real | 172.08 | 6.53 | 167.50 | 5.77 | 169.46 | 6.47 |
| Minimal | 171.35 | 7.81 | 166.50 | 6.36 | 168.58 | 7.36 |
| Average | 174.63 | 6.76 | 172.13 | 7.94 | 173.20 | 7.50 |
| Maximum | 177.92 | 8.11 | 177.87 | 11.16 | 177.89 | 9.88 |
| ANOVA | F=3.93 | p=0.011 | F=13.20 | p=0.000 | F=16.10 | p=0.000 |
| Conclusion | μReal=μMinimum≠μAverage≠μMaximum | |||||
| Real-to-minimum correlation | r=0.79 | p=0.000 | r=0.82 | p=0.000 | r=0.83 | p=0.000 |
Additionally, no differences were observed between male and female cadavers: in the Veracruz group: female, T_REAL (161.00±6.40cm) and T_MIN (163.14±8.53cm); male, T_REAL (168.70±4.87cm) and T_MIN (167.12±5.86cm) and in the Federal District group: female, T_REAL of 164.00±8.71cm, T_MIN of 164.58±3.72cm (p>0.05); male, T_REAL 173.23±5.50cm, T_MIN 172.32±7.81cm (p>0.05).
The data show clear differences between real height and average and maximum heights. However, the correlation between real and minimum heights is adequate for both the Federal District sample (r=0.79; p=0.000) and the Veracruz group (r=0.82; p=0.000), and as a whole (r=0.83; p=0.000).
DiscussionThis study had several limitations. Most likely, the main one is the total number of the sample and the small percentage of women studied. However, in view of the need for a morphometric resource that could be useful to estimate height, particularly in cases in which the whole cadaver is not available or the long bones traditionally used to evaluate the height are missing, it was appropriate to perform this exploratory study in the Mexican population. We used a virtually forgotten approach, Carrea's method.
The study considered 2 populations of Mexican individuals who lived in 2 different geographic regions in our country. From the start, it was important to determine if the phenotypic variability in different parts of the country could influence the results. We are aware that the Mexican population is mestizo, the result of gene mixing between the European (mainly Spanish), American Indian, and African populations,13,14 and that, although there are regions where the phenotype has a stronger European influence, it is generally assumed that the Mexican population is genetically homogeneous. In relation to this point, the statistical tests applied showed no significant differences between the 2 study populations when comparing the 9 morphometric parameters. This is important because the population of the Federal District is composed of a mixture of individuals from other states in the country and individuals born in the city, whereas the individuals studied in Veracruz were mostly natives born in the state. When the usefulness of Carrea's method was evaluated and the values were compared to the real height in both study groups, it was observed that this height was closer to the minimum height and not to the average height, as reported by the author in his technique.8
As described in the ‘Results’ section, there were no significant differences between minimum and real heights in the men or women in either group; however, in this study population, the maximum height and average height values were not useful to estimate the subjects’ real height. This finding is important and again, we believe that genetic and environmental variability had some influence on these results.
The Argentinean population studied by Carrea was mainly of European descent. From 1850 to 1955, Argentina received a large number of European immigrants to a small native population, and recent studies have shown that the European contribution to the Argentinean gene pool is 79.9%, whereas the indigenous contribution is 15.8% and the African, 4.3%.15 This probably explains why that population showed a real height closer to average height, as reported by the author, and not to minimum height, as seen in the results of our study.
Carrea's method has been tested in the Peruvian population, in which a reliability level of 65% was found for the height estimation and in which the correlation between the anterior lower tooth diameters and the individual stature was confirmed.16 However, when making the comparisons, these authors included the real height within the maximum height–minimum height range and, therefore, 65% of their cases had a real height in this range.
This study describes a comparative analysis for each of the heights obtained by Carrea's method (maximum, average, and minimum heights) and the best correlation is seen to correspond to minimum height, regardless of the individual's sex.
In comparing Carrea's method with anthropometric techniques used to estimate real height, it should be mentioned that physical anthropology employs various techniques to determine this value. Authors such as Pearson,17 Trotter and Gleser,18 Belmonte,19 and Menéndez20 are consistent in reporting that the best way to determine real height is to measure the whole skeleton, with a margin of error below 2cm, in accordance with Pearson.17 Based on many studies, however, these authors also agree that it is viable to determine real height by measuring only long bones, in the same way, with a decreased margin of error when longer bones are studied as a whole and an increased margin when only one bone is studied. The study of a femur and another long bone lead to an error range of up to 2.5cm, according to Trotter and Glesser,18 and is as high as 6cm when only the radius is measured.19
ConclusionsIn view of the above, we can conclude: (1) that Carrea's method was suitable in the sample of Mexican individuals studied for estimating real height when minimum height was used as a reference, and (2) this method is a complement to other anthropometric methods and should be tested in other Latin American populations.
Conflict of interestThe authors declare that they have no conflicts of interest in the publication of this article.
To Dr Felipe Edmundo Takajashi Medina, Director of the Instituto de Ciencias Forenses (Institute of Forensic Sciences) of the Superior Court of Justice for the Federal District and to Dr Crosby González Montiel, Director of Expert Services for the State of Veracruz, for allowing the samplings of interest to the research and for assisting with the use of the facilities. To the CONACYT (Consejo Nacional de Ciencia y Tecnología (National Board of Science and Technology) for an academic grant for the master's degree awarded to J.G.G. (Grant No.: 343777).
Grant: J.G.G. received a master's degree grant from CONACYT. Grant No.: 343777.
Please cite this article as: González-Gómez J, Melo-Santiesteban G, Cerda-Flores RM, Calderón-Garcidueñas AL. Evaluación forense comparativa del método odontológico de Carrea para estimar la talla real en cadáveres mexicanos. Rev Esp Med Legal. 2016;42:48–54.