




The clock drawing test is a neuropsychological screening test that is frequently used in clinical practice.
AimTo evaluate the usefulness of the clock drawing test in the forensic environment. To evaluate 3 methods of correction, and to determine its reliability and validity, and assess its usefulness in judicial processes of modification of legal capacity of a person.
Material and methodsA total of 40 cases were analysed in legal proceedings. A structured clinical interview, and a neurological and psychopathological examination were conducted using the CAMDEX-R test. The Mini-Mental State Examination, the Global Deterioration Scale, and the clock drawing test were administered to the order corrected using the CAMCOG, Manos and Méndez methods. The sample was divided into 3 groups: degenerative, psychiatric, and without pathology.
ResultsThe degenerative group obtained the worst results in the clock drawing test in the 3 correction methods. The reliability and validity of the test were adequate. Patients judged not to be legally capable had a worse performance in the clock drawing test.
ConclusionsThe 3 methods of correction of the clock drawing test are shown to be effective. Evaluating the cost-benefit of the short method is recommended. Patients with a modification of legal capacity ruling showed worse results in the clock drawing test.
El test del reloj es una prueba de cribado neuropsicológico que se utiliza con frecuencia en la práctica clínica.
ObjetivoValorar la utilidad del test del reloj en el ámbito forense. Evaluar 3 métodos de corrección, explorar la fiabilidad y validez, y valorar su utilidad en procesos judiciales de modificación de la capacidad de obrar.
Material y métodosSe analizaron 40 casos incursos en procedimientos judiciales. Se realizó una entrevista clínica estructurada, exploración neurológica y psicopatológica a través de la prueba CAMDEX-R. Se administró el Mini-Mental State Examination, la Global Deterioration Scale y el test del reloj a la orden corregido con los métodos de CAMCOG, Manos y Méndez. La muestra se dividió en 3 grupos: degenerativo, psiquiátrico y sin trastorno.
ResultadosEl grupo degenerativo es el que obtuvo peores resultados en el test del reloj en los 3 métodos de corrección. La fiabilidad y validez de la prueba resultaron adecuadas. Los pacientes incapacitados judicialmente presentaron peor rendimiento en el test del reloj.
ConclusionesLos 3 métodos de corrección del test del reloj se muestran eficaces. Valorando el coste-beneficio, se recomienda el método más breve. Los pacientes con una sentencia de modificación de la capacidad civil presentan peores resultados en el test del reloj.
The clock drawing test (CDT) is a quick and simple neuropsychological test that assesses the cognitive state and different mechanisms involved in the performance of the task, such as constructive praxis, verbal understanding, planning, executive functions and symbolic mental representations.1 It has been used as a screening instrument to assess cognitive impairment in a clinical and research population, but its applicability and usefulness in the forensic field is unknown.1 It was developed by Goodglass and Kaplan2 in a battery of neuropsychological assessments for the evaluation of constructive apraxia and visuospatial agnosia.3 It has been proposed by several authors as a screening test to evaluate cognitive impairment, mainly in the assessment of neurodegenerative diseases, especially in dementias. The CDT has raised interest due to its easy application and brevity, as well as due to the information that can be obtained from its analysis. Several criteria have been proposed for the application and scoring of the CDT,1 such as those of Shulman et al.,4,5 Sunderland et al.,6 Woolf-Klein et al.,7 Méndez et al.,8 Manos and Wu,9 Babins et al.10 and Nyborn et al.,11 although currently there is no universally recognised consensus for its correction. The application of the CDT in legal capacity change procedures (incapacitation) may be useful to assess cognitive function. The reliability and validity of the CDT in the forensic field is unknown.
The main objective of our study was to determine the usefulness of the CDT as a screening test of cognitive impairment in the forensic field.
The objective was threefold. First, to assess the overall result of three correction methods on the basis of cognitive impairment. The Cambridge Cognitive Examination (CAMCOG),12 Méndez and Manos9 methods were chosen. Second, to explore the reliability among evaluators of the three correction methods and to examine the external validity with two criteria: the Mini-Mental State Examination (MMSE)13 and the Global Deterioration Scale (GDS).14 Finally, to assess the usefulness of the CDT in legal processes of changes to legal capacity (incapacitation).
Material and methodSubjectsThe sample was made up of 40 patients, selected by non-probability sampling of consecutive cases attended to at the Medical-Forensic Clinic of the Instituto de Medicina Legal y Ciencias Forenses de Cataluña [Institute of Legal Medicine and Forensic Science of Catalonia]. Patients over the age of 65 years involved in different legal procedures who required an assessment of probable cognitive impairment were included. Patients who presented severe psychic or sensory impairments which prevented them from understanding the tests applied and those who did not have an adequate level of understanding were excluded.
Eleven males (27.5%) and 29 females (72.5%) were included, with a mean age of 78.83 (SD±7.94; range: 65–95 years). The civil status of most of the patients was concentrated in the category of widow (40%), followed by the category of single (32%), married or with a partner (15%) and separated (12%). A total of 7.5% had not been to school, although they knew how to read and write; 37.5% had primary education; 37.5% had the basic baccalaureate; 7.5% had the equivalent of professional training; 5% had the higher baccalaureate and the remaining 5% had university degrees. The majority of participants were involved in legal incapacity procedures. In some cases, the expert opinion was requested by the Public Prosecution Service (42.5%) and, in others, by a court of first instance (37.5%), followed by procedures in courts of investigation and criminal courts (15%), Registry Office (2.5%) and in social courts (2.5%).
MethodA structured clinical interview and a neurological and psychopathological examination were performed for each patient by a forensic internal medicine specialist and a clinical psychologist through various sections of the Revised Cambridge Examination for Mental Disorders of the Elderly (CAMDEX-R).15 The sections used were: Section A. Interview with the patient, which includes assessment of their current state, personal and family history. Section C. Observations of the interviewer, which covers the attitude of the patient, presence of hallucinations, description of their mood, language, attention and others. Section D. Physical examination, which includes blood pressure, pulse, stretch reflexes, presence of hemiparesis, gait, mobility, tremor, visual and auditory impairments, among others. Section F. Pharmacological treatment.
The existence and grade of cognitive impairment was examined using the MMSE13 as a screening instrument for cognitive impairment, with the cut-off point established at 23, and the GDS,14 which stratifies the cognitive and general functional status of the patient into seven grades: one denotes the absence of cognitive abnormality and seven is indicative of very severe cognitive impairment. Similarly, the CDT was administered on request, following the procedures described by Goodglass and Kaplan: Draw the face of a clock, position all the numbers and place the hands at ten past eleven.2 The instructions were repeated the number of times necessary to ensure a correct level of understanding. The CDT administration instructions were the same in each case, as the participants only performed the CDT once. The CDT was not administered in copy format. The CDT was corrected through two independent evaluators following the scoring criteria of the CAMCOG,12,15 Méndez8 and Manos.9 The correction methods were chosen for the following two reasons. First, all three are quantitative correction methods, not like those of Nyborn et al.11 (qualitative method which studies the type of errors), nor like those of Shulman and his group4,5 and Sunderland et al.,6 who use semi-quantitative methods. Second, the methods are different with regard to correction criteria: from only three criteria up to a greater thoroughness with the 20 points proposed by Méndez.8
The CAMCOG correction criteria consist of three items. One point if the circle is correct, one point if the numbers are placed in the correct position and one point if the hands are placed in the correct position.12
The Manos method consists of ten items and is corrected as follows: the number 12 must be at the top. One line is drawn through the centre of the number 12 and the centre of the circle, dividing the circle in half. Then, a second line is drawn at a right angle to the first line through the centre of the circle, dividing it into quarters. Two more lines are drawn through the centre of the circle, dividing it into eighths. One point is given to each of the following numbers which corresponds to the eighths: 1, 2, 4, 5, 7, 8, 10 and 11. Regarding the hands, the authors’ criteria should be followed. One point is given to the short hand which points to number 11 and another point to the hand which points to number 2. No points are awarded for the hands if they are approximately equal in length or for a long hand at 11 and a short hand at 2, nor for hands of any length that point to other numbers. A short hand at number 11 and a long hand at number 3 would be worth one point for the short hand. Numbers drawn outside the circle are scored simply by extending the dividing lines. Marks instead of numbers score no points.9
The Méndez method consists of assessing 20 items grouped into three sections: only five points if one or more hands are present, 12 points if the symbols corresponding to the numbers of the clock are present and three points if an attempt has been made to indicate the time in some way, if the figure is closed and the lines can be classified as part of a closed figure. The full explanation of each of the 20 points is listed in the author's paper.8
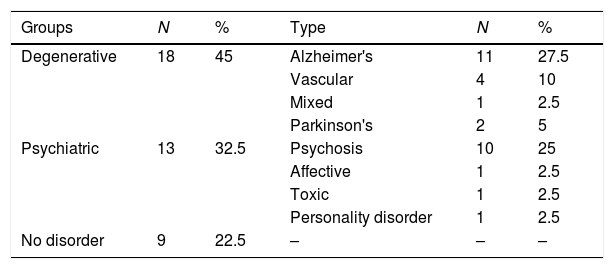
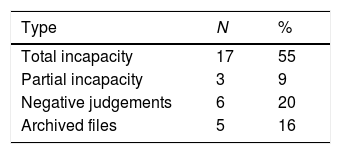
The diagnosis and grade of cognitive impairment was established for each participant by consensus of the investigators and following DSM-IV-TR criteria.16 The sample was divided into three subgroups: group with no disorder, psychiatric disorder and degenerative group, which included Alzheimer's dementia, vascular dementia, mixed dementia and Parkinson's disease. The descriptions of the diagnostic groups are shown in Table 1.
Finally, the judicial files were reviewed to assess the court decision, i.e. the judgement. The judgements of legal incapacity were selected and correlated to the CDT results.
Statistical analysisThe data were analysed by the Statistical Package for the Social Sciences (SPSS), version 14.0 for Windows. Several descriptive statistics were used, including the intraclass correlation coefficient to establish the reliability between observers and Cronbach's α coefficient to establish internal reliability. To calculate the criterion's external validity, Pearson's and Spearman's correlation coefficients were used, depending on whether or not the distribution was normal. For the comparison between groups, the Kruskal–Wallis H, Mann–Whitney U and chi-square (χ2) tests were used. The proposed level of significance was p<0.05.
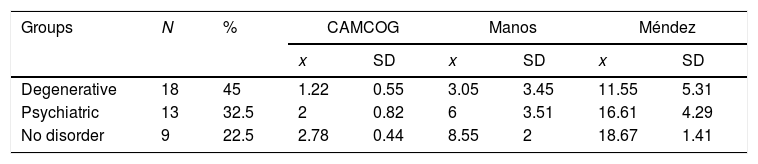
ResultsAssessment of the overall result of the three clock drawing test correction methods on the basis of cognitive impairmentThe descriptive results of the three correction methods in the three comparison groups (degenerative, psychiatric and no disorder) are shown in Table 2. It can be observed that the group with no disorder shows higher mean scores. Fig. 1 shows the CDT images.
 A normal clock drawing test in a subject with no disorder. (B and C) The result of the test in two women (aged 89 and 78) with Alzheimer")
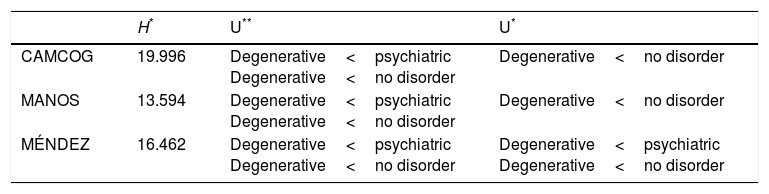
Table 3 shows the differences between the groups and the three correction methods. Greater differences were observed in the degenerative group compared to the other two groups. The no disorder group differs from the other two groups in the three correction methods and, finally, the Méndez method is the only one which differentiates the degenerative and psychiatric groups.
Differences between groups and correction methods.
| H* | U** | U* | |
|---|---|---|---|
| CAMCOG | 19.996 | Degenerative<psychiatric Degenerative<no disorder | Degenerative<no disorder |
| MANOS | 13.594 | Degenerative<psychiatric Degenerative<no disorder | Degenerative<no disorder |
| MÉNDEZ | 16.462 | Degenerative<psychiatric Degenerative<no disorder | Degenerative<psychiatric Degenerative<no disorder |
Kruskal–Wallis H and Mann–Whitney U.
The results show adequate reliability among investigators. The consensus was significant in the Méndez correction method (r=0.980; p<0.01), the Manos correction method (r=0.979; p<0.01) and CAMCOG (0.924; p<0.01). The three methods provide high reliability, with negligible discrepancies between them.
Regarding internal reliability, the three correction methods are shown to be adequate: Méndez (α=0.931), Manos (α=0.925) and CAMCOG (α=0.719). The more complex the correction method is, the higher its internal reliability, possibly due to the presence of a greater number of items. However, the Méndez and Manos methods show the same reliability. The CAMCOG only uses three correction items versus the Manos method which uses 10, and the Méndez method which uses 20.
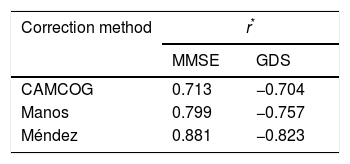
ValidityWith regard to the validity of the external criterion, the results are shown in Table 4. The three CDT correction methods show a high and similar correlation to the MMSE and GDS external criteria. The more exhaustive the correction method is, the greater the correlation with the external criterion.
Validity of external criterion.
| Correction method | r* | |
|---|---|---|
| MMSE | GDS | |
| CAMCOG | 0.713 | −0.704 |
| Manos | 0.799 | −0.757 |
| Méndez | 0.881 | −0.823 |
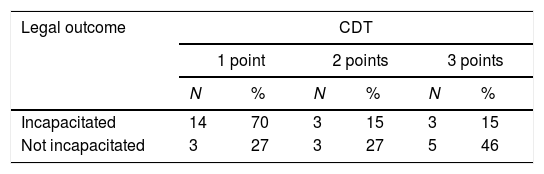
Of the total sample, 80% were involved in legal capacity change procedures. One patient died before the judgement was issued and was excluded. Table 5 shows the final legal outcomes, and it can be observed that total incapacity was established in more than half of the cases versus 9% partial incapacity, and that the remaining cases were negative judgements. The legal capacity judgements in relation to the results of the CDT following the CAMCOG correction are detailed in Table 6. This correction method is shown because it is the most simple and because it demonstrates a validity and reliability similar to the other more complex correction methods. There is a trend that patients declared legally incapacitated provide fewer correct answers than those with a judgement of no changes to their legal capacity (χ2=5.465; p=0.065). The trend is maintained with both the Manos method (χ2=18.623; p=0.029) and the Méndez method (χ2=18.415; p=0.241), although this trend is only significant in the Manos method.
Judgements of legal capacity and CDT (CAMCOG methoda).
| Legal outcome | CDT | |||||
|---|---|---|---|---|---|---|
| 1 point | 2 points | 3 points | ||||
| N | % | N | % | N | % | |
| Incapacitated | 14 | 70 | 3 | 15 | 3 | 15 |
| Not incapacitated | 3 | 27 | 3 | 27 | 5 | 46 |
The CDT has been one of the most used cognitive screening methods due to: its rapid administration; ease of application and correction, as it is a test that can be completed irrespective of language and education level; the good inter-observer and test–retest reliability; its high levels of sensitivity, specificity and predictive validity; and its good correlation with other measuring instruments of cognitive function.1,5,17
The results of our study show that the CDT is useful for evaluating cognitive impairment in forensic samples. The degenerative group presented lower scores than the group with no disorder and the group of psychiatric patients. These results are similar to others in a clinical population.1,17,18 The three methods do not differentiate the comparison groups, except for the degenerative group. Some authors have not found the CDT useful for the diagnosis of mild cognitive impairment. In this regard, in a review of various studies,19 it was observed that in most investigations no differences were found in the mean scores of the CDT between the group with mild cognitive impairment and the group with no impairment. Only two studies endorsed the usefulness of this instrument for screening between the two groups.
Our results showed similar psychometric characteristics among the three correction systems assessed. Consistent with the conclusions of Mainland et al.,1 the three correction methods are similar. Any of the three methods are recommended for assessing time-benefit in the forensic assessment, although the CAMCOG method is the most efficient.
It is very important to have simple, quick to apply and effective instruments in the forensic field to assess the diagnosis and degree of cognitive impairment. Together with the clinical assessment, this can allow us to make considerations and draw conclusions in relation to legal capacity for the management of an individual and his/her wealth. In this study, we have verified the usefulness of the CDT as a simple and effective test to assess cognitive impairment in conjunction with other tests, and to help us make decisions with regard to whether or not to change an individual's legal capacity. Our results indicated that subjects legally declared to have changed legal capacity had a lower score on the CDT.
As limitations of our study, it should be noted that the sample size is small, which may affect the reliability of our results.
In terms of future proposals, it would be interesting to compare the usefulness of the CDT in the forensic field for the diagnosis of cognitive impairment among different types of dementia (Alzheimer's dementia, vascular dementia, mixed dementia, frontotemporal dementia and dementia associated with Parkinson's disease), as has already been done in the clinical field.20 Similarly, it would be interesting to replicate the results with a larger number of samples from legally incapacitated subjects. In addition, it would be interesting to study if the joint use of the CDT with other tests increases the sensitivity and specificity of the diagnoses in the forensic field. It seems that the use of other screening tests, such as the MMSE, are useful in forensic assessment.21
In conclusion, the three correction methods of the CDT were proven to be useful as a screening instrument for evaluating cognitive impairment in the forensic field. The group with no disorder differed from the degenerative and psychiatric groups in the three correction methods. The only method which differentiated the degenerative and psychiatric groups was the Méndez method.
The reliability coefficients among evaluators were high and similar to those obtained in studies with a clinical population. The CDT presented adequate reliability among observers, indicating that it is a test with negligible interference by the evaluator. Internal reliability proved to be adequate in the three methods. The validity of the CDT was adequate with regard to the two external criteria: MMSE and GDS. It has recently been considered that, despite the multiple and various CDT correction methods, the best method is the most simple one.1
The legally incapacitated patients presented worse results in the CDT than those who had a judgement with no change to their legal capacity.
Taking into account the validity and reliability of the CDT in the forensic sample, as well as the ease of application of the test, this may be an extremely useful neuropsychological tool in clinical entities that present with cognitive impairment in initial forensic assessments. Future studies will need to establish sensitivity and specificity criteria in forensic samples and in different clinical entities.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Mohíno Justes S, Pujol Robinat A, Pérez Bouton MP. El test del reloj en la evaluación forense. Rev Esp Med Legal. 2018;44:144–149.