










Subtrochanteric nonunion is a challenging problem. Several techniques have been employed in the literature to address this problem, yielding varying results. The objective of this review is to present the surgical details of a new technique recently developed, and to analyze the literature about surgical techniques applied to this problem to date.
Materials and methodsThe detailed surgical technique of a new, dynamic system to fix subtrochanteric nonunion is presented. All literature regarding nonunion fixation of subtrochanteric nonunion was revised from 2000 to August 2025. Only papers with 2 or more patients treated by fixation of an aseptic subtrochanteric nonunion were selected. Varus and shortening correction, debridement, use of bone graft, type of device, and immediate weight bearing were searched for and analyzed in every paper.
Results347 papers were fully reviewed. 26 finally met the inclusion criteria. Varus correction was not always necessary, but when required, extramedullary systems achieved better correction. Leg shortening was overlooked by most papers, which accepted the shortening of the involved leg. Most papers use debridement and several types of bone grafts. It seems useful in atrophic nonunion, but not in hypertrophic ones. All devices but one worked in a nondynamic compression way. Most systems do not allow for immediate weight bearing, which is important for elderly people.
ConclusionsThe new dynamic technique for healing of subtrochanteric nonunion fulfills all the requirements to solve this problem: healing, varus and leg length correction, and immediate weight bearing. As few patients have been reported with this technique, a prospective, multicenter study is warranted and currently ongoing.
La pseudoartrosis subtrocantérea es un problema importante y difícil de tratar. Se han empleado varias técnicas en la literatura para abordar este problema, arrojando resultados variables. El objetivo de esta revisión es presentar los detalles quirúrgicos de una nueva técnica recientemente desarrollada y analizar la literatura sobre técnicas quirúrgicas aplicadas a este problema hasta la fecha.
Materiales y métodosSe presenta la técnica quirúrgica detallada de un nuevo sistema dinámico para corregir la pseudoartrosis subtrocantérea. Se ha revisado toda la literatura sobre la fijación de la pseudoartrosis subtrocantérea desde enero de 2000 hasta agosto de 2025. Se seleccionaron artículos con dos o más pacientes tratados mediante fijación de una pseudoartrosis subtrocantérea no infectada. En cada artículo se buscó y analizó la corrección del varo y el acortamiento, el desbridamiento, el uso de injerto óseo, el tipo de dispositivo y la carga inmediata de peso.
ResultadosSe revisaron 347 artículos. Veintiséis finalmente cumplieron con los criterios de inclusión. La corrección del varo no siempre fue necesaria, pero cuando sí lo fue, los sistemas extramedulares lograron una mejor corrección. El acortamiento de la pierna fue pasado por alto por la mayoría de los artículos, que aceptaron el acortamiento de la pierna afectada. La mayoría de los articulos emplean un desbridamiento de la zona y varios tipos de injertos óseos. Esto parece útil en las pseudoartrosis atróficas, pero no en las hipertróficas (que son la inmensa mayoría). Todos los dispositivos empleados en la literatura (excepto uno) funcionaron aplicando compresión no dinámica. La mayoría de los sistemas empleados no permiten la carga de peso inmediata, lo cual es importante para los pacientes mayores.
ConclusionesLa nueva técnica dinámica para tratar la pseudoartrosis subtrocantérea cumple con todos los requisitos para resolver este problema: consolidación, corrección del varo y la longitud de las piernas, y soporte inmediato de peso. Como se han descrito pocos pacientes con esta técnica, es necesario y ya está en marcha un estudio prospectivo multicéntrico.
Hip fractures are very frequent, with over 10 million cases treated yearly worldwide.1
Subtrochanteric fractures are a subtype of hip fractures defined as fractures of the proximal femur that occur within 5cm of the distal extent of the lesser trochanter.2 Overall incidence of these fractures is estimated to be around 15–20 per 100,000 population, accounting for 10–30% of all hip fractures.2,3
This fracture is difficult to treat and is prone to nonunion. It is estimated that, with modern techniques of treatment, about 7–20% of subtrochanteric fractures will develop nonunion.3
The main factors involved in this high rate of nonunion are twofold. First, the high mechanical stress in this zone. The subtrochanteric area bears a very high varus stress in anatomic conditions, which is even higher if a non-anatomical reduction of the fracture (in varus) is achieved when fixation is carried out.3 Second, the high cortical bone composition of this area. The cortical bone has less vascular flow, and its capacity to heal is somewhat less than trabecular bone.3 These two factors make this area more prone to nonunion than neighboring areas, like the intertrochanteric region.3
Many good papers have recently reviewed the treatment of subtrochanteric fracture nonunion.2,4 DeRogatis4 recently published the best review on the treatment of subtrochanteric hip fracture nonunions. In their conclusions, they claimed that study heterogeneity precluded a formal meta-analysis. Many techniques and procedures are mixed in many papers, making it difficult to retrieve clear conclusions.
Every surgical technique comprises many surgical steps. Many of them are possible to combine, and everyone has the potential to enhance or worsen healing.
We have recently reported the results of the first 5 patients with a novel technique that implies a dynamic fixation of the nonunion site, allowing for full correction of varus and leg length discrepancy.5 At the present time, we are following a total of 25 patients, which has allowed us to further refine the surgical technique (here presented).
The objective of this review is to describe the technique in detail and to analyze in the literature several key surgical steps when reconstructing a subtrochanteric nonunion.
Materials and methodsA general view of this technique has just been published by us.5 Some details of that technique were missing in the original article, and others has been added as result of new cases. So, a detailed report of the actual technique is described here.
The bibliographic review was performed according to the principles of de PRISMA ScR requirements.6 The detailed protocol has been revised by all authors. The final protocol was registered prospectively with the Open Science Framework on 23 July 2025 (https://osf.io/2tygw/).
To be included in the review, papers should be centered on the surgical technique to treat subtrochanteric nonunions. Peer-reviewed journal papers were included if they were: published between the period of 2000–2025, written in English or Spanish, involved human participants, and described the surgical technique employed in sufficient detail (at least: implant used, osteotomy or not, bone graft used, postoperative protocol). Case reports and review papers were discarded. Nonunions due to previous surgical osteotomies (not fractures) were also discarded. Pediatric patients (less than 18 years old) were also discarded.
To identify potentially relevant documents, the following bibliographic databases were searched from 2000 to July 2025: PubMed, Embase, Cochrane review databases, and the Google search engine. The search strategies were drafted by consensus between authors. The PubMed (MEDLINE) search was done with the keywords “Subtrochanteric” AND “nonunion” between the years 2000 and July 2025. We also identified reports lacking the aforementioned keywords, but which were found while searching other identified reports. The final search results were exported into Zotero, and duplicates were removed.
A data-charting form was jointly developed by the authors to determine which variables to extract. The reviewers independently charted the data, discussed the results, and continuously updated the data-charting form in an iterative process.
We grouped the studies by the types of surgical procedure involved: implant, graft, osteotomy, reduction, and postoperative treatment. We also summarized the type of settings, populations, and study designs for each group, along with the measures used and broad findings. Where we identified a systematic review, we counted the number of studies included in the review that potentially met our inclusion criteria and noted how many studies had been missed by our search, adding them to it.
Detailed surgical techniquePatient selectionThis technique is intended for non-infected (aseptic) nonunions or loss of fixation (breakage, cut-out, or any other form) of subtrochanteric hip fractures. So, to indicate this technique, all these requirements must have been followed:
- a)
Subtrochanteric: Original fracture line in the area between the upper part of the lesser trochanter and 5cm below the inferior margin of the lesser trochanter.
- b)
Nonunion: More than 6 months with pain on walking and no imaging signs of healing (X-ray or CT). Or loss of fixation: Original implant breakage or loss of original fixation at any time.
- c)
No infection present: C-reactive protein levels should be within normal levels. If a previous surgery was done less than 6 weeks before, two separate samples must show a decreasing value. No other clinical sign of infection (redness, pus, open wound) should be present.
The goal of the surgical technique is to overcorrect the varus deformity to get a final 150° valgus angle at the femoral neck. It is also important that the distal part of the proximal side of the nonunion be in contact with the distal part (diaphyseal bone), to get a dynamic compression from the first postoperative day (Fig. 1).

The plate to use should be a DHS (dynamic hip screw, several trademarks sell it), with at least 6 holes, and an angulation of 135–150°.
A radiographically calibrated image of the proximal femur of the patient should be used. An AP Pelvis X-ray should be taken with both knees in 15° of internal rotation. Over this template, measurements are done.
It is recommended to use a 150° plate for “low” nonunions, and a 135° plate for “high” nonunions (more proximal nonunions). If we use the 150° plate, the cephalic screw should follow the central axis of the femoral neck. Nevertheless, If we use the 135° plate, to get 150° of valgus at the neck, the path for the cephalic screw must be 15° of varus (Fig. 2). The tip of the screw should be as near to the center of the hip as possible. Anyway, a slight downward position of the tip of the screw is possible (as seen in Fig. 1), if necessary, to avoid the same hole as the previous implant.

Lines are drawn as seen in Fig. 2. It is useful to measure the distance of the entry point to de tip of the greater trochanter, or the hole of the previous implant, or any other reference to be seen later on fluoroscopy. That will be the final position in AP view. In the lateral view, the screw should be just in the center.
Patient positionPreoperative antibiotics should be administered, as usual in the hospital (2gr cefazolin in our center). Anesthesia should be given to last at least two hours (mean duration of surgery is 112min).5
Patient is set in a traction table, and the proximal part of the femur is rotated 15° inward. This allows for a perfect AP view of the hip. No traction is given; the traction table is only necessary to hold the limb, to facilitate the approach to the hip, and later, to correct rotation if it was malaligned.
Skin preparation is done as usual, and the patient is draped.
Implant retrieval and surgical approachPrevious material should be retrieved using previous incisions. If a nail is broken inside the bone, some percutaneous techniques can be used to retrieve it.7
The surgical approach is a subvastus lateral approach. Incision is performed just lateral to the greater trochanter, going down for about 15cm (Fig. 3). After skin and subcutaneous tissue are incised, the fascia lata is incised in line with the skin incision. Vastus lateralis is identified and separated from the linea aspera in the posterior part of the femur. A Hohmann retractor is set in order to separate de muscle anteriorly.

Three samples of the nonunion site are taken for microbiological study to rule out infection. If macroscopically signs of infection are detected now (pus, smell, etc.), the technique should be aborted, nonunion debrided, and an external fixator used to provisionally fix de nonunion till infection is solved.
Head preparation: filling the void and insertion of the cephalic screwThere is a void in the previously retrieved cephalic screw of the blade. This void is worth filling to get a better purchase of the new screw. A 40-gr stick of allogenic trabecular bone is prepared as follows: the width of the previous hole is measured, and a trephine is used to get a barrel of the same width (Fig. 4). This is impacted in the hole with an impactor.

As previously planned, the guidewire is inserted in the femoral head as deeply as possible to get into the hard bone of the femoral head. After drilling, a cephalic screw of correct length is inserted.
Decompaction of the nonunion siteThis is a key point. After identification of the nonunion site, a chisel is carefully inserted through the nonunion site. The idea is to decompact both fragments to be able to mobilize them later. Opening the medial space, at least 0.5cm, is quite important. Usually, it is not necessary to break the bone, but if any bar of bone is present, it can be broken with a chisel. Do not separate the periosteal envelope of the zone. It is also paramount not to violate the vascular flow to this area (Fig. 5). No bone graft is added, and no decortication is done.
Over-valguization of the nonunion chisel introduced till medial cortex; (rigth) opening of the medial part of nonunion.")
In this moment, the DHS (of at least 6 holes) is introduced to the previously introduced cephalic screw. To correct the position of the femoral head, the plate should be placed just over the diaphyseal bone. To accomplish this, a Lowman retractor is recommended. Softly, the retractor is tightened, and the plate comes to the diaphyseal bone, reducing the nonunion (Fig. 6).
Final fixation and wound closing
After plate gathering to the femoral shaft, get compression at nonunion site. It is quite important to avoid any distraction applied to the leg. Assure that no traction is given and compress slightly the limb. This is a very important point to assure proper compression and a buttress effect on the medial side of the nonunion. At this point, it maybe necessary to loosen a little bit the lowman retractor to facilitate compression.
Rotation of the limb is now assessed and corrected if necessary. With a lateral view of the proximal femur, the knee (intercondylar axis) should be aligned to get a 15° anteversion of the proximal femur.
Then, 3.5 cortical screws are applied. It is recommended that at least 6 bicortical screws with good purchase be inserted. If a longer plate is applied, the more distal screw can be a monocortical screw to diminish stress at the distal tip of the plate. If any screw is found not to hold properly, it may be useful to apply a wire cerclage over the plate.
Good purchasing is verified by moving the construct under fluoroscopic vision (Fig. 7).

The vastus is left in situ with no stitches. Fascia lata, subcutaneous tissue, and skin are closed in the usual fashion.
Postoperative treatmentImmediate weight-bearing is allowed with crutches on the first postoperative day. No limitation on activities is given.
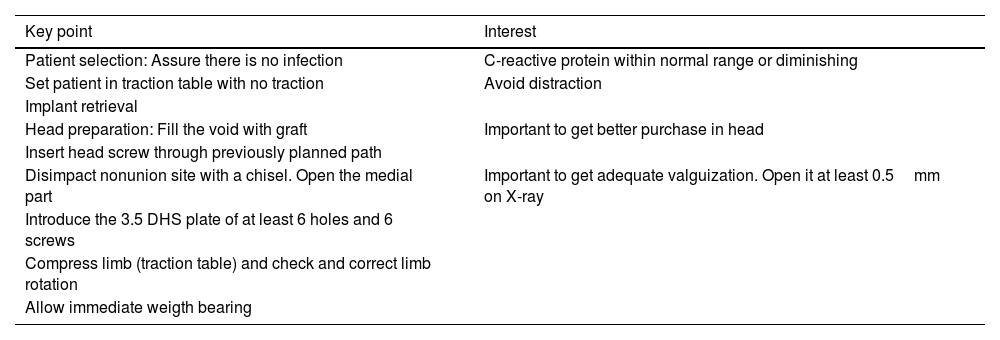
Key points of the surgical technique are given in Table 1.
Key points of surgical technique.
| Key point | Interest |
|---|---|
| Patient selection: Assure there is no infection | C-reactive protein within normal range or diminishing |
| Set patient in traction table with no traction | Avoid distraction |
| Implant retrieval | |
| Head preparation: Fill the void with graft | Important to get better purchase in head |
| Insert head screw through previously planned path | |
| Disimpact nonunion site with a chisel. Open the medial part | Important to get adequate valguization. Open it at least 0.5mm on X-ray |
| Introduce the 3.5 DHS plate of at least 6 holes and 6 screws | |
| Compress limb (traction table) and check and correct limb rotation | |
| Allow immediate weigth bearing |
Searching PubMed retrieved 347 results. A title search discarded 310 results, so 37 titles were available for further review. Review articles were also revised, and 2 citations were added to the search. EMBASE search added no papers to the search. Google search added 1 paper.
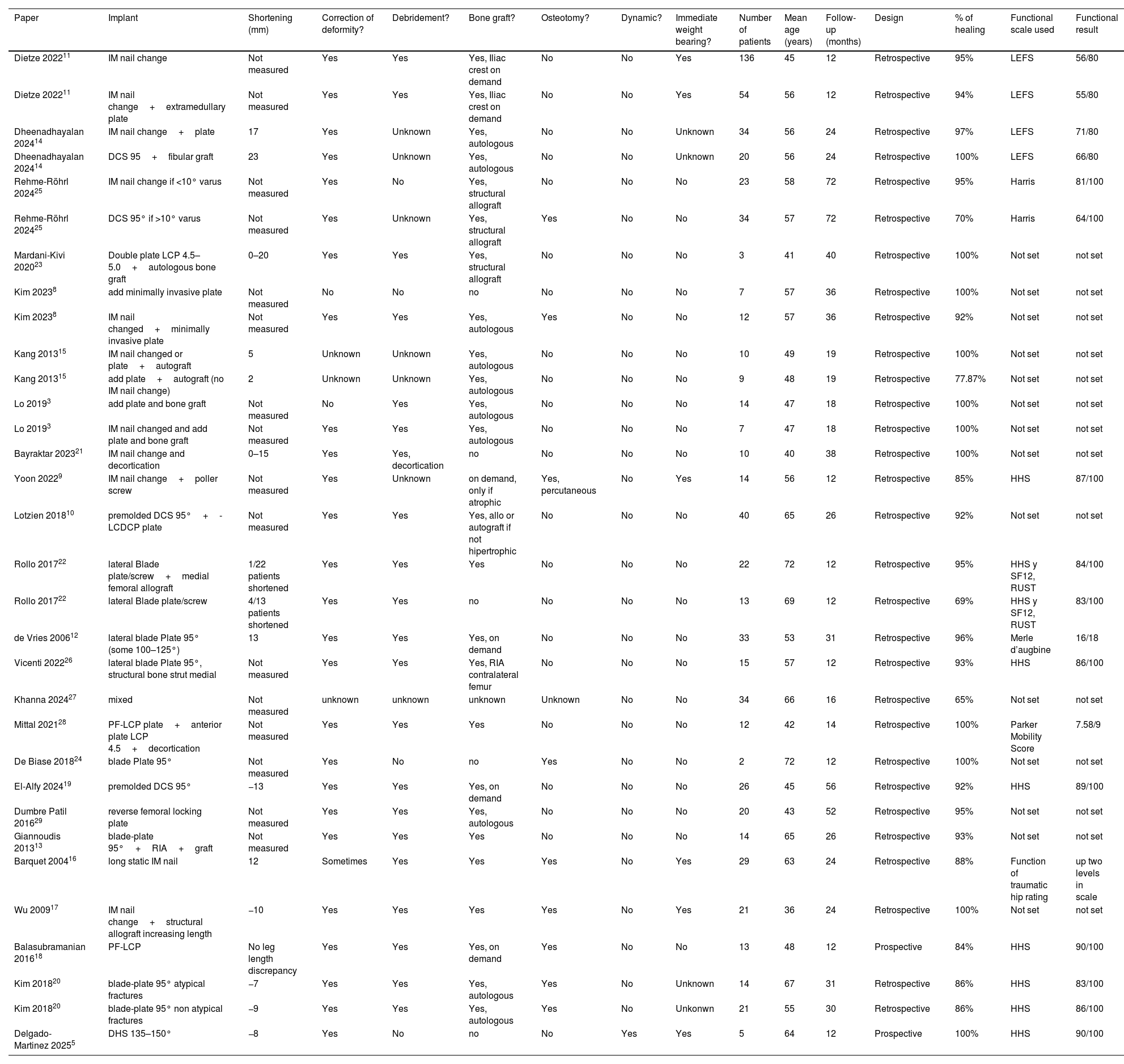
After careful review of full papers, 16 papers were discarded: 2 had mixed results with other pathologies, 4 did not focus on nonunion, 2 were commentaries on papers, and 8 were about femoral neck or shaft nonunion. So, finally, 24 papers were available for full scanning (Table 2).
Summarizes the main results of each paper.
| Paper | Implant | Shortening (mm) | Correction of deformity? | Debridement? | Bone graft? | Osteotomy? | Dynamic? | Immediate weight bearing? | Number of patients | Mean age (years) | Follow-up (months) | Design | % of healing | Functional scale used | Functional result |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dietze 202211 | IM nail change | Not measured | Yes | Yes | Yes, Iliac crest on demand | No | No | Yes | 136 | 45 | 12 | Retrospective | 95% | LEFS | 56/80 |
| Dietze 202211 | IM nail change+extramedullary plate | Not measured | Yes | Yes | Yes, Iliac crest on demand | No | No | Yes | 54 | 56 | 12 | Retrospective | 94% | LEFS | 55/80 |
| Dheenadhayalan 202414 | IM nail change+plate | 17 | Yes | Unknown | Yes, autologous | No | No | Unknown | 34 | 56 | 24 | Retrospective | 97% | LEFS | 71/80 |
| Dheenadhayalan 202414 | DCS 95+fibular graft | 23 | Yes | Unknown | Yes, autologous | No | No | Unknown | 20 | 56 | 24 | Retrospective | 100% | LEFS | 66/80 |
| Rehme-Röhrl 202425 | IM nail change if <10° varus | Not measured | Yes | No | Yes, structural allograft | No | No | No | 23 | 58 | 72 | Retrospective | 95% | Harris | 81/100 |
| Rehme-Röhrl 202425 | DCS 95° if >10° varus | Not measured | Yes | Unknown | Yes, structural allograft | Yes | No | No | 34 | 57 | 72 | Retrospective | 70% | Harris | 64/100 |
| Mardani-Kivi 202023 | Double plate LCP 4.5–5.0+autologous bone graft | 0–20 | Yes | Yes | Yes, structural allograft | No | No | No | 3 | 41 | 40 | Retrospective | 100% | Not set | not set |
| Kim 20238 | add minimally invasive plate | Not measured | No | No | no | No | No | No | 7 | 57 | 36 | Retrospective | 100% | Not set | not set |
| Kim 20238 | IM nail changed+minimally invasive plate | Not measured | Yes | Yes | Yes, autologous | Yes | No | No | 12 | 57 | 36 | Retrospective | 92% | Not set | not set |
| Kang 201315 | IM nail changed or plate+autograft | 5 | Unknown | Unknown | Yes, autologous | No | No | No | 10 | 49 | 19 | Retrospective | 100% | Not set | not set |
| Kang 201315 | add plate+autograft (no IM nail change) | 2 | Unknown | Unknown | Yes, autologous | No | No | No | 9 | 48 | 19 | Retrospective | 77.87% | Not set | not set |
| Lo 20193 | add plate and bone graft | Not measured | No | Yes | Yes, autologous | No | No | No | 14 | 47 | 18 | Retrospective | 100% | Not set | not set |
| Lo 20193 | IM nail changed and add plate and bone graft | Not measured | Yes | Yes | Yes, autologous | No | No | No | 7 | 47 | 18 | Retrospective | 100% | Not set | not set |
| Bayraktar 202321 | IM nail change and decortication | 0–15 | Yes | Yes, decortication | no | No | No | No | 10 | 40 | 38 | Retrospective | 100% | Not set | not set |
| Yoon 20229 | IM nail change+poller screw | Not measured | Yes | Unknown | on demand, only if atrophic | Yes, percutaneous | No | Yes | 14 | 56 | 12 | Retrospective | 85% | HHS | 87/100 |
| Lotzien 201810 | premolded DCS 95°+-LCDCP plate | Not measured | Yes | Yes | Yes, allo or autograft if not hipertrophic | No | No | No | 40 | 65 | 26 | Retrospective | 92% | Not set | not set |
| Rollo 201722 | lateral Blade plate/screw+medial femoral allograft | 1/22 patients shortened | Yes | Yes | Yes | No | No | No | 22 | 72 | 12 | Retrospective | 95% | HHS y SF12, RUST | 84/100 |
| Rollo 201722 | lateral Blade plate/screw | 4/13 patients shortened | Yes | Yes | no | No | No | No | 13 | 69 | 12 | Retrospective | 69% | HHS y SF12, RUST | 83/100 |
| de Vries 200612 | lateral blade Plate 95° (some 100–125°) | 13 | Yes | Yes | Yes, on demand | No | No | No | 33 | 53 | 31 | Retrospective | 96% | Merle d’augbine | 16/18 |
| Vicenti 202226 | lateral blade Plate 95°, structural bone strut medial | Not measured | Yes | Yes | Yes, RIA contralateral femur | No | No | No | 15 | 57 | 12 | Retrospective | 93% | HHS | 86/100 |
| Khanna 202427 | mixed | Not measured | unknown | unknown | unknown | Unknown | No | No | 34 | 66 | 16 | Retrospective | 65% | Not set | not set |
| Mittal 202128 | PF-LCP plate+anterior plate LCP 4.5+decortication | Not measured | Yes | Yes | Yes | No | No | No | 12 | 42 | 14 | Retrospective | 100% | Parker Mobility Score | 7.58/9 |
| De Biase 201824 | blade Plate 95° | Not measured | Yes | No | no | Yes | No | No | 2 | 72 | 12 | Retrospective | 100% | Not set | not set |
| El-Alfy 202419 | premolded DCS 95° | −13 | Yes | Yes | Yes, on demand | No | No | No | 26 | 45 | 56 | Retrospective | 92% | HHS | 89/100 |
| Dumbre Patil 201629 | reverse femoral locking plate | Not measured | Yes | Yes | Yes, autologous | No | No | No | 20 | 43 | 52 | Retrospective | 95% | Not set | not set |
| Giannoudis 201313 | blade-plate 95°+RIA+graft | Not measured | Yes | Yes | Yes | No | No | No | 14 | 65 | 26 | Retrospective | 93% | Not set | not set |
| Barquet 200416 | long static IM nail | 12 | Sometimes | Yes | Yes | Yes | No | Yes | 29 | 63 | 24 | Retrospective | 88% | Function of traumatic hip rating | up two levels in scale |
| Wu 200917 | IM nail change+structural allograft increasing length | −10 | Yes | Yes | Yes | Yes | No | Yes | 21 | 36 | 24 | Retrospective | 100% | Not set | not set |
| Balasubramanian 201618 | PF-LCP | No leg length discrepancy | Yes | Yes | Yes, on demand | Yes | No | No | 13 | 48 | 12 | Prospective | 84% | HHS | 90/100 |
| Kim 201820 | blade-plate 95° atypical fractures | −7 | Yes | Yes | Yes, autologous | Yes | No | Unknown | 14 | 67 | 31 | Retrospective | 86% | HHS | 83/100 |
| Kim 201820 | blade-plate 95° non atypical fractures | −9 | Yes | Yes | Yes, autologous | Yes | No | Unkonwn | 21 | 55 | 30 | Retrospective | 86% | HHS | 86/100 |
| Delgado-Martinez 20255 | DHS 135–150° | −8 | Yes | No | no | No | Yes | Yes | 5 | 64 | 12 | Prospective | 100% | HHS | 90/100 |
The overall quality of the papers was generally poor; 22 were retrospective case-series studies, with an evidence level of IV. Patients included in every study were generally low, between 2–136 (mean 23 patients). Criteria for nonunion were also quite variable, ranging from clinical or radiological criteria of nonunion from one year after fracture to 4 weeks after it.
Varus correctionNearly all papers agree that varus is quite important factor for nonunion. All scanned papers stated that varus was corrected somehow if it was present. Only one paper compared one group just adding a plate (without correction)(7 patients) versus changing nail and adding plate (with correction, 12 patients).8 Healing rates were better for the non-corrected group (100% versus 92%). Nevertheless, it is supposed that those patients were assigned to that group because no varus malalignment was found.
For varus correction, most papers do not perform osteotomy. They perform correction mainly by debridement of the nonunion zone and then valgus alignment of the proximal fragment. Open reduction is the most common system, but one paper performs it percutaneously.9
Many papers do not indicate the degree of correction. Many of them just state that a correction has been made. Most of them try to get the anatomical valgus compared to the contralateral side.9–13 Only the paper with the technique here presented states that an overcorrection to 150° valgus is the objective.5
In summary, there is wide agreement that an anatomical or slightly overcorrected valgus is necessary for good healing.
ShorteningThis is a problem frequently found in clinical practice but, surprisingly, not registered in many papers. Twelve papers present the shortening of the cases before and after revision surgery.5,12,14–23
Most papers accept or even increase the leg length discrepancy. A final shortening of between 11 and 23mm is commonly accepted.12,14–16
Only four papers try to restore or at least diminish this leg-length discrepancy, as follows.
One way to achive this is by inserting bone graft. Wu et al.17 designed a technique in which the nonunion area is distracted, and structural bone autograft from the posterior iliac crest is inserted. Finally, a nail is used to fix it. It is claimed to work fine for leg-length discrepancies of 2–5cm, and a mean of 1cm lengthening is described in their series of 21 patients, with 100% healing.
Other way to achieve lengthening of the shortened leg is through valguization. Kim et al.,20 using a 95° blade plate achieved a lengthening of about 7–9mm just by correcting the valgus angle, and adding bone graft. El-Alfy et al.19 also achieved increased leg length (up to 13mm) through valguization of the proximal femur and adding bone graft. In both cases a static construction was performed. Delgado-Martinez et al.,5 performing a dynamic over valgus correction of the nonunion also achieved a mean leg lengthening of 8mm in their series of 5 patients with 100% healing. No graft is used in his method,5 avoiding the morbidity of the donor zone.
In summary, it is necessary to take into account the leg-length discrepancy and to try to correct it, if possible.
Debridement of nonunionMost papers do perform a debridement, or even a cortical delamination, in order to promote biological healing. It is difficult to ascertain if a nonunion in this zone is atrophic or hypertrophic. Some papers deal only with atrophic nonunions,13 so the debridement and the addition of osteoinductive products (bone graft, RIA, BMPs, and so on) seem warranted. Most of them also use it to get correction of the varus deformity, but at the expense of increasing shortening.12,15,16
Two papers do not perform a debridement of the nonunion zone: De Biase et al.,24 in a case report of just two cases, state that it just opens the nonunion zone, without debridement. Delgado-Martinez et al.,5 in a 5-case prospective study, just opened de nonunion zone, without debridement. In both papers, healing achieves 100%.
In summary, if a nonunion is atrophic, it may be useful to perform debridement. For hyperthophic nonunions, it seems useless.
Bone graftMany types of bone grafts have been used. Autografts are usually preferred when available, due to their better osteogenic properties.13 Most papers use other grafts, mainly allografts, when an autograft is not available. Some papers use structural allografts.23,25 RIA (reamer-irrigator-aspirator) from bone marrow from the same patient has also been used.13,26
Just 4 papers claim not to use bone grafts in any case.5,21,22,24 When comparing healing rates between the groups of patients, there is no clear advantage to using bone grafts. Healing rates in non-grafting papers range from 69 to 100% and grafting papers range from 84 to 100%.
In summary, it seems appropriate to use grafting in atrophic nonunions, but it does not seem so useful in hyperthrophic nonunions.
Device: dynamic or static?Several types of devices have been used to fix the nonunion zone. Most of them work in a static mode.
An intramedullary nail is the most common material used. It is claimed to ream the canal and to use a wider nail, to get better purchase.3,11,14–17,21,25,27 To get some correction of the varus, the medialization of the entry point has been marked as important. Some advancements have been published regarding this item, as the use of poller screws to help the nail maintain the entry point in a medial position (to avoid varus).9
The addition of a plate to the intramedullary nail is another system to enhance fixation.3,11,14 Some papers just add a plate (3.5 or 4.5 locked plate) to the previous fixation if the position is acceptable.3,8,11,14
The second most used implant is a blade plate of 95° or a Dynamic condylar screw (DCS) of 95°.10,12–14,19,22,24–26 It is used to fix the nonunion in a static mode. Some papers bend the plate to achieve some 100–120° of angulation of the Plate.12,19 Union rates range from 67 to 100%, but rates of complications (infections, loss of fixation, and so on) are higher than with the intramedullary nail. Nevertheless, the capacity to correct varus is greater.
Another implant used is the proximal femoral locking compression plate (FP-LCP) Plate.18,28 It is quite similar to the blade plate or DCS, but more screws are anchored to the head of the femur. Similar results to those with the other extramedullary systems have been reported. A proximal femoral locking compression plate placed in reverse has been also used.29
Only one dynamic system has been used in this indication.5 A dynamic sliding hip screw (DHS) of 135–150°. That is the technique presented in this paper. The nonunion zone is opened, the varus deformity overcorrected, and then fixed in a completely dynamic fashion, allowing the patients to bear weight from the first operative day. Even a few patients have been reported,4 results seem promising, with 100% healing and nearly no complications.
In summary, many systems to fix the nonunion have been reported. Intramedullary systems are the most commonly used and present fewer complications, but their capacity to correct varus deformity is limited. Extramedullary systems can be used to enhance or substitute the intramedullary nail, with a higher risk of complications. Extramedullary dynamic devices are the most promising ones.
Immediate weight bearing or not?Immediate weight bearing is important. As most of the patients are elderly, they can get a lot of complications due to long-term rest. Nevertheless, most papers do not allow the patients to immediately engage in full weight-bearing.
Many papers that use intramedullary fixation do promote immediate weight bearing.9,11,16,17 It is considered a stable method of fixation, but not all intramedullary papers allow immediate weight bearing.21
Nevertheless, all papers using extramedullary fixation with a non-dynamic device, do avoid immediate weight bearing, in some cases waiting even 3 months.13,18,19,22,24,26,28 The extramedullary dynamic fixation (DHS) of Delgado-Martinez et al.5 does permit and even enhance immediate weight bearing.
In summary, a device that allows weight bearing must be sought when fixing the subtrochanteric nonunion. Intramedullary devices and Dynamic DHS usually allow for achieving this goal.
ConclusionWe present in detail a new technique for the treatment of subtrochanteric nonunions that can correct any degree of varus, lengthen the leg, and allow immediate weight-bearing.
It has been shown that to achieve healing in a subtrochanteric nonunion, it is paramount to correct varus deformity and to correct leg-length discrepancy. It is also desirable to allow immediate weight bearing.
Many devices and systems have been used, but they can not fulfill all the proposed objectives. The IM nail cannot always correct the varus deformity, and non-dynamic extramedullary devices do not allow immediate weight bearing.
A technique that fully achieve all the requirements in all cases is the new dynamic technique explained here in detail.
Level of evidenceLevel of evidence v.
Author contributionsConceptualization, Delgado-Martinez AD.; methodology, All authors.; validation, all authors.; data curation, Cañada-Oya H and Zarzuela-Jimenez C.; writing—original draft preparation, Delgado-Martinez AD.; writing—review and editing, Rodriguez-Merchan ED.; supervision, Delgado-Martinez AD. All authors have read and agreed to the published version of the manuscript.
Generative IANo Generative IA has been used when preparing this manuscript.
FundingThis research received no external funding.
Conflicts of interestThe authors declare no conflicts of interest.
We thank the Spanish group of investigation into subtrochanteric nonunions for their valuable considerations regarding this paper. The group is formed by: Renovell-Ferrer P; Videla M; Murcia-Asensio A; Olias-Lopez B; Boluda J; Rodrigo A; Romero E; Ferrero F; Aguado H; Carrera I; Hernandez-Hermoso JA; Gómez-Vallejo J; Cano-Porras JR; Parron R; Delgado-Rufino FB. No GenIA has been used in any form for the preparation of this paper.
