






Postoperative pain in ambulatory surgery (AS) continues to be a recurrent problem despite anesthetic and surgical advances. Analgesic prescription and follow-up by patients at home may be a determining factor. Our objective was to evaluate analgesic prescription and its impact on the intensity of postoperative pain at 24&#¿;h and 7 days in an AS unit.
MethodsRetrospective cohort study of patients undergoing AS. Anthropometric data, ASA classification, surgery, anesthesia, analgesic prescription and postoperative pain. A telephone call was made by nurses to evaluate the DAP at 24&#¿;h and one week after surgery.
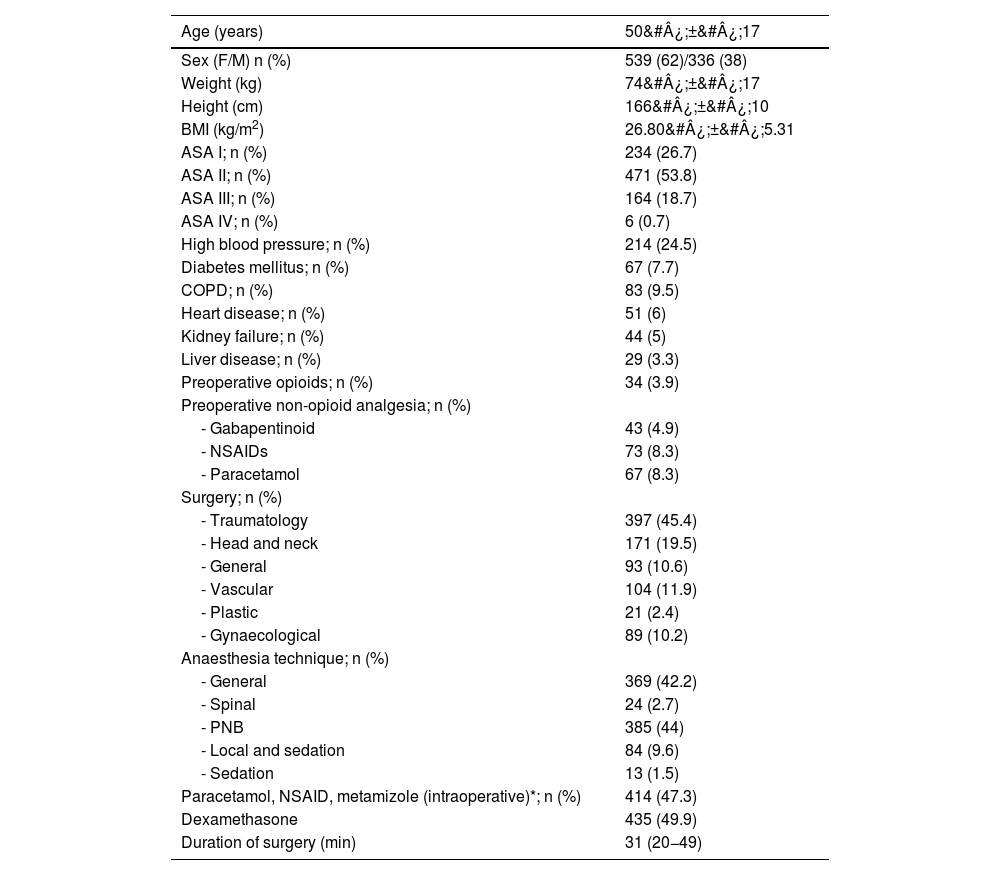
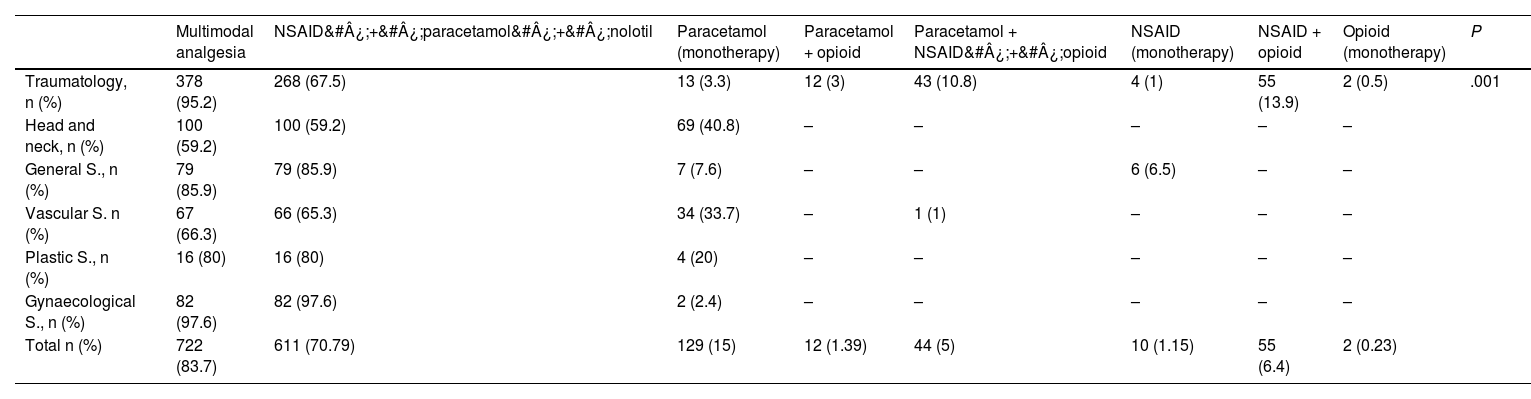
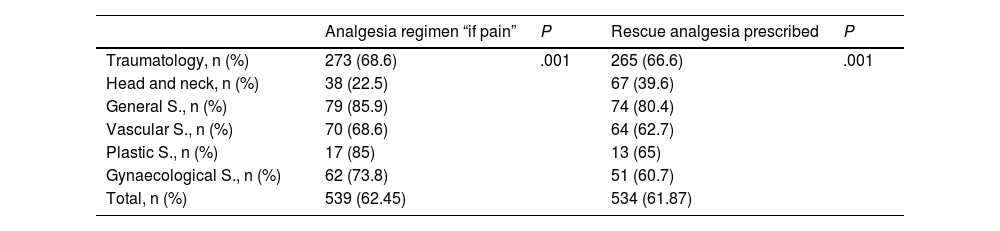
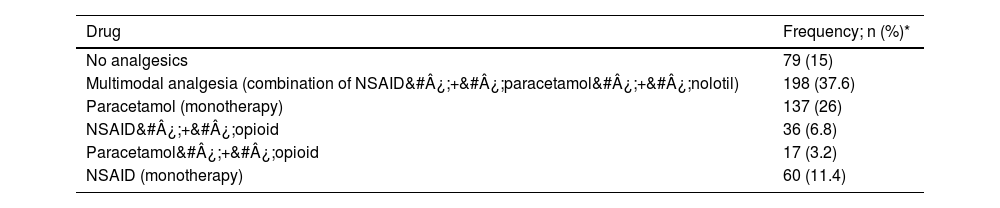
ResultsA total of 875 patients, 62% women, aged 50&#¿;±&#¿;17 years, were studied. Orthopedic (45.4%); head and neck (19.5%); general (10.6%); vascular (11.9%); plastic (2.4%) and gynecological (10.2%) surgery was performed. Multimodal analgesia was prescribed: 83.7%, combination of nonsteroidal anti-inflammatory drug (NSAID)&#¿;+&#¿;paracetamol&#¿;+&#¿;metamizole: 70.79%; opioid&#¿;+&#¿;paracetamol or NSAID or in monotherapy:13.1%; monotherapy with paracetamol (15%) or NSAID (1.15%). Some 62.45% were prescribed “if pain” and 61.87% had rescue analgesia. At 24&#¿;h the median (IQR) of pain on the self-assessing verbal scale was 3 (2–5) and at one week 2 (0–4). The presence of moderate-severe pain was 46% at 24&#¿;h and 31% at one week after surgery.
ConclusionsOur results show great variability in analgesic prescription with insufficient control of postoperative pain in ambulatory surgery. Although the multimodal analgesic strategy has been widely used, opioid prescription has been insufficient in surgeries associated with moderate to severe pain.
El dolor agudo postoperatorio (DAP) en cirugía mayor ambulatoria (CMA) sigue siendo un problema recurrente a pesar de los avances anestésicos y quirúrgicos. La prescripción analgésica y seguimiento por los pacientes en domicilio puede ser un factor determinante. Nuestro objetivo fue evaluar la prescripción analgésica y su impacto en el DAP a las 24&#¿;h y 7 días en una unidad de CMA.
MétodosEstudio de cohortes retrospectivo de pacientes intervenidos en CMA. Se recogieron datos antropométricos, clasificación ASA, cirugía, anestesia, y prescripción analgésica. Se realizó llamada telefónica por enfermería para evaluar el DAP a las 24&#¿;h y a la semana de la cirugía.
ResultadosSe estudiaron 875 pacientes, 62% mujeres con edad media de 50&#¿;±&#¿;17 años. Se realizó cirugía ortopédica (45,4%); de cabeza y cuello (19,5%); general (10,6%); vascular (11,9%); plástica (2,4%) y ginecológica (10,2%). Se prescribió analgesia multimodal: 83,7%, combinación de antiinflamatorio no esteroideo (AINE)+ paracetamol&#¿;+&#¿;metamizol:70,79%; opioides 13% (asociados a paracetamol/AINE o en monoterapia); sólo paracetamol (15%) o AINE (1,15%). Un 62,45% recibió prescripción «si dolor» y 61,87% analgesia de rescate. A las 24&#¿;h la mediana (RIQ) de DAP en la escala numérica verbal (ENV) fue de 3 (2–5) y a la semana de 2 (0–4). Presentaron dolor moderado-intenso el 46% a las 24&#¿;h y el 31% a la semana de la cirugía.
ConclusionesExiste una gran variabilidad en la prescripción analgésica con un insuficiente control del DAP en CMA. La analgésica multimodal ha sido ampliamente utilizada destacando una prescripción de opiáceos insuficiente en cirugías asociadas a dolor moderado-intenso.
