





Hip fractures typically affect elderly individuals with multiple comorbidities. Early surgical intervention within the first 48 hours has been shown to improve outcomes. However, when on antiplatelet therapy, surgery is often delayed preventing bleeding complications. This study aims to compare the incidence of perioperative complications, the need for blood transfusions, and the length of hospital stay between two groups of patients: those with delayed surgery more than 72 h due to antiplatelet use and those who had surgery within the first 48 h.
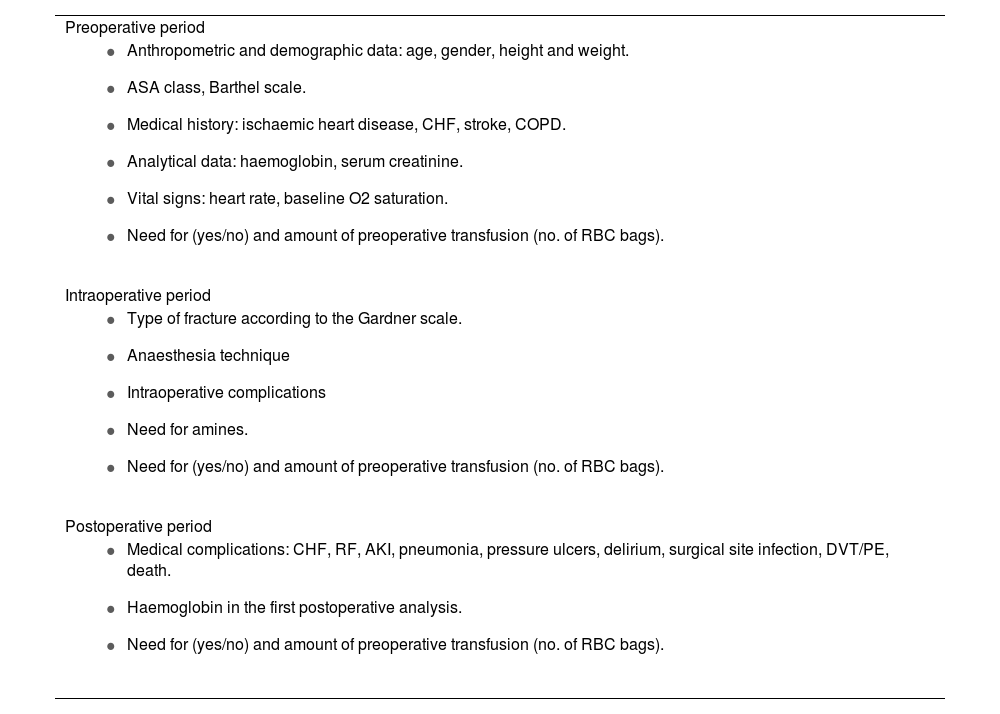
MethodsA retrospective cohort study was conducted on 110 patients who underwent hip fracture surgery between December 2012 and April 2018. Patients who had a delay of more than 72 h in the surgery were selected. A 1:1 randomized sampling was made to obtain a control group with surgery within the first 48 h.
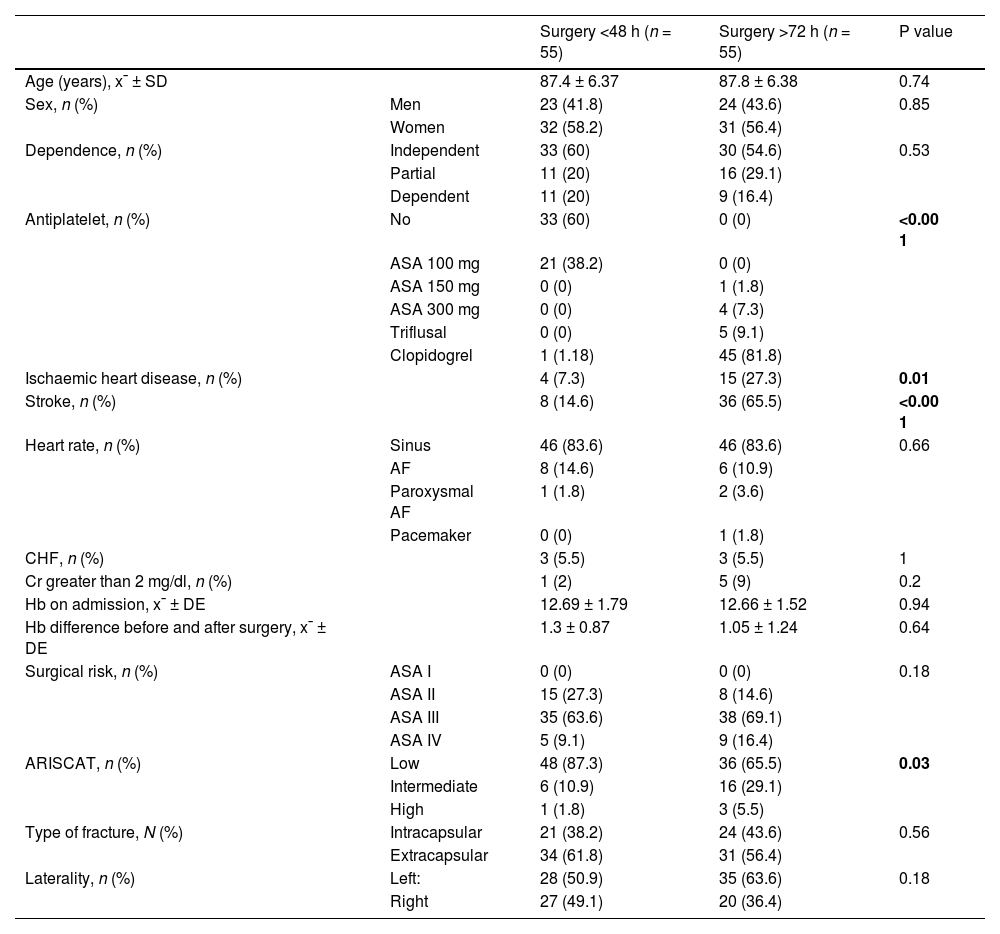
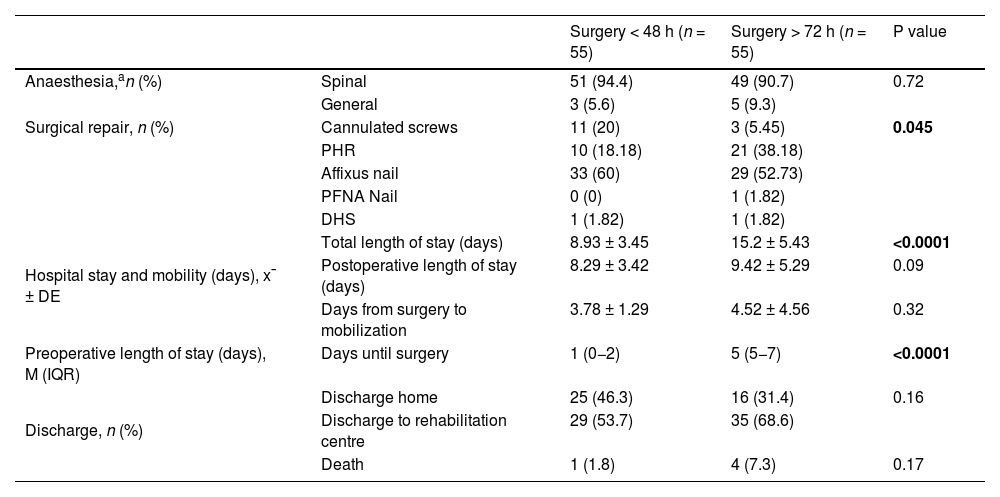
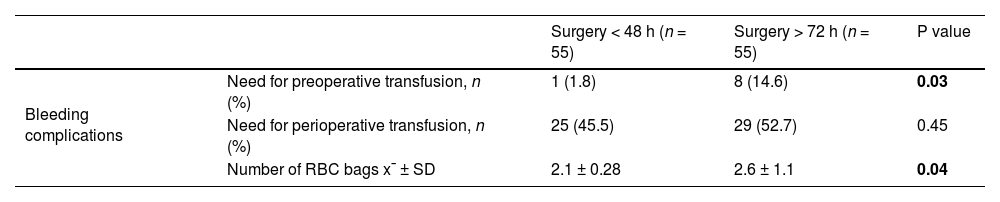
ResultsThe baseline clinical characteristics were similar between the two groups, except for a higher rate of ischemic heart disease, cerebrovascular accidents and use of antiplatelet medication in the delayed surgery group. The early surgery group had a higher rate of acute renal failure (14.6% vs. 1.8%). The rest of the postoperative complications were higher in the delayed group (5.5% vs. 20%). The hospital stay was longer in the delayed group (15.2 vs. 8.93 days), although this difference accounted for the preoperative stay.
ConclusionThis study found that delayed surgery was linked to a higher incidence of medical complications and a longer hospital stay due to the wait time for surgery.
Las fracturas de cadera afectan a pacientes mayores con múltiples comorbilidades. La intervención en las primeras 48 horas desde la fractura, mejora el pronóstico. Sin embargo, en pacientes tratados con antiagregantes, la cirugía se pospone a menudo para evitar complicaciones hemorrágicas. En este estudio se compararon la incidencia de complicaciones perioperatorias, la necesidad de transfusión y la estancia media hospitalaria en pacientes operados dentro de las primeras 48 horas con pacientes retrasados más de 72 horas por la toma de antiagregantes.
MétodosEstudio analítico de cohortes históricas sobre una base de 1447 pacientes intervenidos de fractura de cadera entre diciembre de 2012 y abril de 2018. Se seleccionaron los pacientes con retraso >72 horas por tomar antiagregantes. El grupo control se obtuvo por muestreo aleatorizado 1:1 en pacientes intervenidos antes de 48 h tras la fractura.
ResultadosSe incluyeron 110 pacientes. Las características clínicas basales fueron similares entre los grupos, excepto por una mayor tasa de patología asociada al uso de antiagregantes en el grupo con cirugía retrasada. La estancia hospitalaria fue superior en el grupo con retraso (15.2 vs. 8.93 días). La tasa de Insuficiencia renal aguda fue mayor en el grupo con cirugía precoz (14.6 vs 1.8%), El resto de las complicaciones postoperatorias fue superior en el grupo con retraso (5.5% vs 20%).
ConclusiónLos pacientes con retraso en la cirugía presentaron una mayor tasa de complicaciones médicas y una estancia hospitalaria más prolongada atribuible al tiempo de espera a la cirugía.
