






After a decade since AUDIT LATAM 2012, an executive committee of the International Osteoporosis Foundation of Latin America (LATAM-IOF) updated the data on the epidemiological burden of osteoporosis and fragility fractures in Latin America to generate greater awareness about osteoporosis and prevent fragility fractures.
ObjectiveTo describe the burden of osteoporosis and fragility fractures, their management and treatment, and the availability of health resources in Latin America over a 10-year period.
Materials and methodsA two-phase study was designed. Phase 1 collected demographic data from 2015 to 2019, described the current infrastructure for Healthcare Systems osteoporosis related as well as the related health care policies on osteoporosis. We assessed the availability of diagnosis tools and pharmacological treatment. Phase 2 focused on the incidence of major fragility fractures in men and women aged 50 and over, as well as the costs of these fractures when available.
ResultsNineteen countries completed phase 1. More than 40% of the population is over 50 years-old and life expectancy is on average 75.8 years. The availability of densitometry (DXA) is 0.68 per 100,000 inhabitants. Seven countries have FRAX® calibrated with their own epidemiological data. Bisphosphonates are the primary treatment option for osteoporosis. A larger number of countries have conducted calcium and vitamin D intake surveys. There are 68 active medical and/or patient societies involved in activities related with osteoporosis. Phase 2 included fewer countries, representing a significant gap in osteoporosis information in the region. Our rates of hip fractures are intermediate ranging between 108 and 276.2 per 100,000 inhabitants being the highest in Colombia and the lowest in Mexico. The costs of hip fracture range from USD 4959 to USD 8261.
ConclusionsRegional data from Latin America revealed that healthcare assistance and global awareness has improved in comparison to the 2012 figures. The hip fracture rates in Latin America remains at intermediate levels compared to other regions. There is a scarcity of cost studies, however, high costs of osteoporotic fractures were confirmed to have a negative impact on healthcare systems of the region.
Después de una década desde el AUDIT LATAM 2012, un comité ejecutivo de la International Osteoporosis Foundation de Latinoamérica (LATAM-IOF) actualizó los datos sobre carga epidemiológica de la osteoporosis y las fracturas por fragilidad en Latinoamérica, con el fin de generar mayor conciencia acerca de la osteoporosis y prevenir las fracturas por fragilidad.
ObjetivoDescribir la carga epidemiológica de la osteoporosis y de las fracturas por fragilidad, su manejo y tratamiento, y la disponibilidad de recursos sanitarios en América Latina.
Materiales y métodosSe diseñó un estudio de dos fases. La fase 1 recopiló datos demográficos de 2015 a 2019, describió la infraestructura actual de los sistemas de atención médica relacionados con la osteoporosis, así como las políticas de atención médica de dicha enfermedad. Se evaluó la disponibilidad de herramientas de diagnóstico y tratamiento farmacológico. La fase 2 se centró en la incidencia de fracturas graves por fragilidad en hombres y mujeres de 50 años o más, así como en el costo de estas fracturas cuando estuvo disponible.
ResultadosDiecinueve países completaron la fase 1. Más del 40% de la población tiene más de 50 años y la esperanza de vida es de 75,8 años en promedio. La disponibilidad de densitometría (DXA) es de 0,68 por 100.000 habitantes. Siete países cuentan con FRAX® calibrado con sus propios datos epidemiológicos. Los bifosfonatos son la principal opción de tratamiento para la osteoporosis. Un mayor número de países han realizado encuestas sobre la ingesta de calcio y vitamina D. Existen 68 sociedades médicas o de pacientes activas, involucradas en actividades relacionadas con la osteoporosis. La fase 2 incluyó menos países, lo que representa una brecha significativa en la información sobre osteoporosis en la región. Nuestras tasas de fracturas de cadera son intermedias, y oscilan entre 108 y 276,2 por 100.000 habitantes, siendo las más altas de Colombia y las más bajas de México. Los costos de una fractura de cadera oscilan entre USD 4.959 y USD 8.261.
ConclusionesDatos regionales de América Latina revelaron que la asistencia sanitaria y la conciencia global han mejorado, en comparación con las cifras de 2012. Las tasas de fractura de cadera en América Latina se mantienen en niveles intermedios; se confirma que los altos costos de las fracturas osteoporóticas tienen un impacto negativo en los sistemas de salud de la región.
A decade after the publication of the first white paper about Epidemiology, Costs and Burden of Osteoporosis (OP) in Latin America in 2012 (Audit LATAM 2012),1 an Executive Committee (SteerCo LATAM AUDIT 2021)2 from the Latin-American region of the International Osteoporosis Foundation (LATAM-IOF) decided to update the preceding white paper. We designed and launched a project to review and refresh key indicators regarding the burden and management of OP and fragility fractures (FF) of this region. All countries within the Latin American Region were invited to participate.
Numerous changes have occurred in the Latin American region over the last decade: demographics have shown an aging of the population with a significant increase in life expectancy, changes in the organization and services provided by healthcare systems; additionally the development of more precise tools for the diagnosis, management, and treatment of OP. Some examples are the calibration of FRAX® (Fracture Risk Assessment Tool) as part of numerous Latin American countries, using country specific epidemiological data, the introduction of new diagnostic tools such as TBS (Trabecular Bone Score), REMS (Radiofrequency Echography Multispectometry) and 3D-DXA to the Latin American market, as well as the development of new pharmacological treatments and country-specific guidelines for prevention, diagnosis, and treatment of OP. Additionally, post-fracture care programs have been introduced through the Fracture Liaison Services (FLS).
Having these changes in mind, the objective of a new Audit was to provide updated information on demographic indicators, as well as current epidemiological figures and costs associated with OP and FF. The report also described the available infrastructure and health policies on OP management within the region.
MethodsTo collect the necessary information for this research, the SteerCo LATAM AUDIT 2021 designed two questionnaires. The first one, an 18-item questionnaire, was designed to gather information on demographics, characteristics of each country's Health System, prevention and lifestyle measures, diagnostic methods, availability of pharmacological treatments and patient awareness. The second questionnaire specifically requested data on the incidence of mayor FF from large national databases or large health facilities over a five-year period (2014–2019). The International Classification of Diseases, 10th Revision (ICD-10), was used to identify the fractures (S72.0, S72.1, S72.2, S52.5, S52.6, S42.2, S42.3, S12.0, S12.1, S12.2, S22.0, S22.1, S32.0, and T08). If available, publications were also requested on the direct cost of these fractures considering each event of diagnosis, surgery, hospitalization, treatment and follow-up depending on the country health system, calculated in national money and converted to US dollars at the date of publication for each country that had this information. The average costs of hip fracture management were adjusted to the year 2021 using the purchasing power parity (PPP) index in the countries with available costs information.
Demographic data and indicators, such as life expectancy were gathered from The Economic Commission for Latin America and Caribbean (CEPALSTAT/Comisión Económica para América Latina y el Caribe – Naciones Unidas/[7/1/2022]) and the World Bank (https://datos.bancomundial.org). Using the list of countries included in CEPAL, invitations to participate in the study were sent to all countries within the region to physicians who are experts in osteoporosis and opinion leaders.
The study was set up in two phases:
Phase 1: In October 2020, an invitation letter come with the first questionnaire and was sent to 19 Latin American countries. The objective of this first questionnaire was to gather data on country demographics, population indicators and projections for 2030 and 2050. The questionnaire also sought information about the characteristics of each Healthcare System, the distribution (percentage of the population covered by public and private medical services), and the availability and cost of diagnostic resources for OP, such as DXA, TBS, Vertebral Fracture Assessment (VFA), and other technologies. In the same questionnaire, information regarding the availability of calcium and vitamin D supplementation, fortified foods, and reports of calcium and vitamin D surveys published locally in the past 10 years were requested. Detailed information on available pharmacological treatments for OP (both branded names and generic/biosimilar presentations) was sought. Additionally, details about osteoporosis prevention programs, including interventions focused on lifestyle modifications, were inquired about.
Also, the questionnaire asked information regarding healthcare reimbursement policy of drugs and diagnosis tests like DXA. The number of scientific and patient societies for OP, and any consensus statements, position papers or guidelines developed during this period. Sources of information included various platforms such as governmental databases, private insurance companies, local publications, scientific societies, and country's expert panel.
Phase 2: The second phase aimed to collect information on the incidence of major fractures (hip, wrist, proximal humerus, and vertebra) using the International Classification of Diseases, 10th Revision (ICD-10) coding for individuals over 50 years old, both sexes, for a 5-year period (2015 and 2019). Ideally, this data should come from national databases. Countries without access to national databases were instructed to use data from third-level healthcare institutions. Additionally, the cost of hip or any other FF was requested when available, as well as any local studies or articles published after 2012 on the epidemiology of OP and FF.
An electronic search of the largest electronic databases (PubMed, Scopus, and Latin-American Index) was conducted for the period of 2010–2021 to retrieve all studies published on these topics. A questionnaire and template were also developed specifically to collect data and distributed along with information and instructions (Annex 1. Supplementary data).
For this report, only demographic information and the burden of OP, FF, and FRAX® were included. All other information can be obtained from the original report International Osteoporosis Foundation [IOF], LATAM Audit, 2021).2
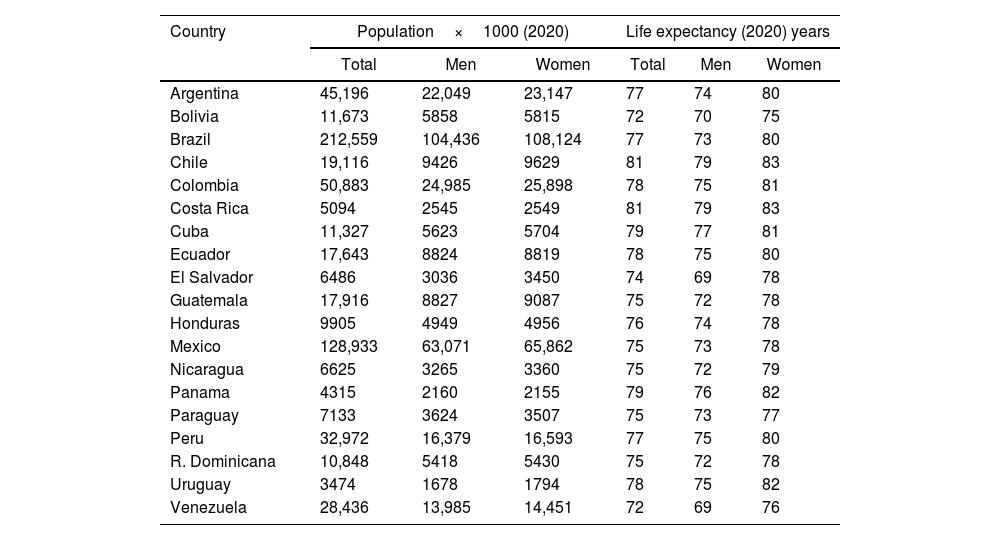
ResultsA total of 19 countries participated in the first phase of the study, including five countries that did not participate from the 2012 edition: El Salvador, Paraguay, the Dominican Republic, Honduras, and Ecuador. The most populous countries in Latin America are Brazil (212.5million) and Mexico (128.9million) while the least are Uruguay (3.4million) and Panama (4.3million) (Table 1). All participant countries showed a significant increase of the proportion of total population over 50 years old with an average increase of 23% across Latin American population. This ranged from 13.3% in Guatemala to 38.6% in Cuba. The countries with over 30% of their population aged over 50 years are Cuba (38.6%) and Uruguay (31.5%). Countries with an increase lesser than 20% include Bolivia (17.9%), Paraguay (17.6%), Nicaragua (16.3%), Honduras (14.2%), and Guatemala (13.3%).
Population and life expectancy in LATAM disaggregated by sex.
| Country | Population×1000 (2020) | Life expectancy (2020) years | ||||
|---|---|---|---|---|---|---|
| Total | Men | Women | Total | Men | Women | |
| Argentina | 45,196 | 22,049 | 23,147 | 77 | 74 | 80 |
| Bolivia | 11,673 | 5858 | 5815 | 72 | 70 | 75 |
| Brazil | 212,559 | 104,436 | 108,124 | 77 | 73 | 80 |
| Chile | 19,116 | 9426 | 9629 | 81 | 79 | 83 |
| Colombia | 50,883 | 24,985 | 25,898 | 78 | 75 | 81 |
| Costa Rica | 5094 | 2545 | 2549 | 81 | 79 | 83 |
| Cuba | 11,327 | 5623 | 5704 | 79 | 77 | 81 |
| Ecuador | 17,643 | 8824 | 8819 | 78 | 75 | 80 |
| El Salvador | 6486 | 3036 | 3450 | 74 | 69 | 78 |
| Guatemala | 17,916 | 8827 | 9087 | 75 | 72 | 78 |
| Honduras | 9905 | 4949 | 4956 | 76 | 74 | 78 |
| Mexico | 128,933 | 63,071 | 65,862 | 75 | 73 | 78 |
| Nicaragua | 6625 | 3265 | 3360 | 75 | 72 | 79 |
| Panama | 4315 | 2160 | 2155 | 79 | 76 | 82 |
| Paraguay | 7133 | 3624 | 3507 | 75 | 73 | 77 |
| Peru | 32,972 | 16,379 | 16,593 | 77 | 75 | 80 |
| R. Dominicana | 10,848 | 5418 | 5430 | 75 | 72 | 78 |
| Uruguay | 3474 | 1678 | 1794 | 78 | 75 | 82 |
| Venezuela | 28,436 | 13,985 | 14,451 | 72 | 69 | 76 |
Data from: CEPALSTAT: Statistical portal of the Economic Commission for Latin America and the Caribbean (ECLAC), and https://datos.bancomundial.org/indicator/SP.URB.TOTL.IN.ZS?locations=CO.
All other countries in the region experienced increases ranging from 20 to 29% for the same age group. Life expectancy in the region has reached an average of 76.5 years, reflecting a mean increase of 1.6 years over the past decade. Most countries have a life expectancy ranging between 72 and 78 years. Only Chile and Costa Rica have a life expectancy above 80 years. On the contrary, Bolivia and Venezuela have the lowest life expectancy at 72 and 74.9 years, respectively (Table 1).
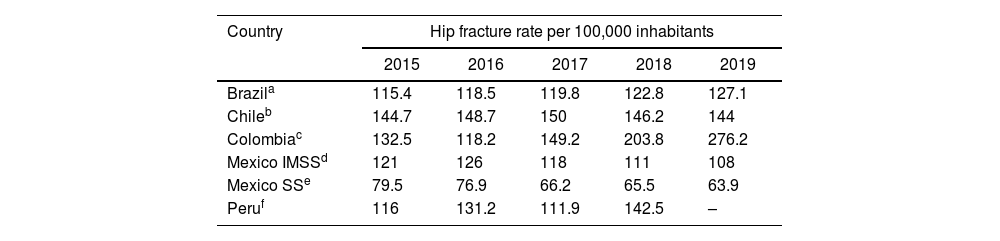
Epidemiology of fragility fractures in the regionOnly 5 countries were able to provide the requested information on major fragility fractures: Brazil, Chile, Colombia, Mexico, and Peru (Table 2).
Epidemiology of FF: Hip fracture rates per 100,000 inhabitants aged ≥50 years, in Brazil, Chile, Colombia, Mexico and Peru.
| Country | Hip fracture rate per 100,000 inhabitants | ||||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | |
| Brazila | 115.4 | 118.5 | 119.8 | 122.8 | 127.1 |
| Chileb | 144.7 | 148.7 | 150 | 146.2 | 144 |
| Colombiac | 132.5 | 118.2 | 149.2 | 203.8 | 276.2 |
| Mexico IMSSd | 121 | 126 | 118 | 111 | 108 |
| Mexico SSe | 79.5 | 76.9 | 66.2 | 65.5 | 63.9 |
| Peruf | 116 | 131.2 | 111.9 | 142.5 | – |
PA Ambulatorial Production: Files from SIA: http://www2.datasus.gov.br/DATASUS/index.php?area=0901&item=1&acao=22&pad=31655.
RD – Reduced Hospital data base: Files from SIH http://www2.datasus.gov.br/DATASUS/index.php?area=0901&item=1&acao=25.
DANE (Departamento Administrativo Nacional de Estadística), SISPRO (Sistema Integral de Información de la Protección Social) & Direccion de Informatica.
The annual of hip fracture rate for Brazil and Colombia trend toward an increase. In Brazil, the observed incidence rate was 115 per 100,000 inhabitants in 2015, with a slight increase of 9% to 117 per 100,000 inhabitants in 2019.
Colombia exhibited a higher increase, rising from 132 in 2015 to 276.2 in 2019, doubling its rates. Chile remains stable around 144 per 100,000 inhabitants in this period.
The Mexican data was obtained from the two largest Healthcare Systems in the country: the Mexican Institute of Social Security (IMMS) and of the Ministry of Health (SS). Data from both systems show an increase in the first three years (2015–2018), but rates dropped in both systems in the last two years. At the IMSS, hip fracture rates decreased from 121 per 100,000 in 2015 to 108 per 100,000 in 2019. A similar trend was observed at the SS, where the rate of hip fractures per 100,000 inhabitants fell from 79.5 in 2015 to 63.92 in 2019. Peru only reported a four-year of follow-up data; the observed rates increased in 18% since 2015–2018. We also recorded data other major fragility fractures (vertebral, proximal humerus, and distal radius) within the same five-year period. Data do not follow a consistent pattern across countries. In Brazil, distal radius fractures are most frequent, followed by proximal humerus fractures, while vertebral fracture incidence is low. Colombia exhibits a high frequency of proximal humerus fractures. For Mexico the data for other mayor FF were obtained only for the SS.
Peru has the lowest incidence of fractures in the region, making its data consistent for this country. There were 4 publications reporting original data on FF: Brazil (2015),3 Colombia (2013)4 and Ecuador (2018)5 and a single publication which includes data from Argentina in 2019 derived from a secondary analysis of old epidemiological studies.6 Publications gathering data from Brazil, Colombia and Ecuador were obtained from national registries or the purpose of calibrating FRAX®. The lowest fracture rates were found in Brazil, while the highest occurred in Colombia (Table 3).
Epidemiological studies on the incidence of fragility fractures in Latin America. Rate per 100,000 inhabitants.
| Country/Year/Author | Incidence | Women | Men |
|---|---|---|---|
| Brazil, 2015 (Zerbini) | 79 | 97 | 54 |
| Colombia, 2013 (Jaller) | 114 | 110 | 82 |
| Ecuador, 2018 (López Gavilanez) | 123 | 166 | 75 |
| Argentina, 2019 (Aziziyeh) | 320 | – | – |
Rate includes all sites of fragility fractures.
During the last decade, few publications on costs of FF were available in Latin America: Argentina (2010),7 Brazil (2014),8 Colombia(2014),9 Chile (2020)10 and Mexico (2013).11 Chile reported only hip fracture costs, whereas all other reports included additional other fracture types.10 Information regarding cost is summarized below:
In Argentina, surgical treatment direct cost of hip fractures varies between USD 3800 and 5500 and includes surgery and 4–7 days of hospitalization depending on whether coverage is provided by the public or private system. The estimated cost per case of nonsurgical vertebral fracture is USD 16,300 and if a vertebroplasty is performed, the cost increases to USD 17,500.7
There are 5 Brazilian publications, all of which cover costs from the perspective of the public sector. All report direct costs of hip fractures and Quality-Adjusted Life Years (QALYs).8,12–15 The cost of a hip fracture treated surgically ranges from USD 2745 to USD 11,911 per event.
Colombia published a study in 2015 that includes estimated costs of the diagnosis and treatment of OP, as well as cost related to hip fractures, distal radius fractures and vertebral fractures, both surgical and nonsurgical treatment. Hip fracture cost of USD 4428.88 per event, surgical vertebral fractures, USD 5855, and distal radius fractures, USD 1196.9
A study published in 2019 in Chile included private and public sector perspectives for direct costs associated with hip fractures. The individual cost of hip fracture treatment in the public system amounted to USD 3919 and USD 9092 in a private hospital.10 Finally, a study published in Mexico in 2013 estimated the yearly direct cost of osteoporosis diagnosis and treatment, as well as the economic impact of hip fractures in 2010 with a forecast for 2020. In 2020, the estimated annual cost for osteoporosis diagnosis and treatments were USD 470 million, while the cost amounted to USD 172 million for osteopenia and USD 364 for hip fractures.11 A more recent estimate of direct costs in Mexico were developed for this AUDIT using the Diagnosis-Related Groups and published by IMSS in 2017, along with the inflation rate to adjust to 2019 costs. According to this report, the estimated direct cost for a hip fracture was USD 7971, USD 3598 for proximal humerus fractures, USD 2771 for vertebral fractures, and USD 2022 for distal radius fractures.11
The average costs of hip fracture management adjusted to the year 2021 using the PPP index in the 5 countries with available costs information are summarized in Fig. 1.
 and the Organization for Economic Co-operation and Development (OECD).")
FRAX® is available in 7 Latin American countries: Argentina, Chile, Brazil, Mexico, Ecuador, Colombia, and Venezuela. Age-adjusted specific thresholds for these countries were developed and published. The intervention threshold is the probability of osteoporotic fracture for a woman with BMI 25.0kg/m2 and a previous fracture, no other clinical risk factors, and no BMD given. The lower assessment is in the case without fracture and risk factors, and the upper assessment was set at 1.2 times the intervention threshold.16 There is an important heterogeneity of the different countries of the region (Fig. 2).
 in both sexes at 65 years of age and previous fracture with a BMI of 24 and with a BMD of the femoral neck of −2.5. Based on specific FRAX® age-adjusted thresholds for Latin American countries. Own elaboration.")
According LATAM AUDIT 2021, all participating countries, except Cuba (where health services are financied exclusively with national government resources) have a mixed health system, whose financing is done between the government, the employer and the employee, with an increase in out-of-pocket spending mainly in Venezuela (64.3%), Guatemala (52.2%) and Paraguay (49.4%) according to data from the International Development Bank (BDI), published in 2021 by the Public Expenditure Observatory of the Center for the Dissemination of Economic Knowledge (CEDICE). The WHO recommends that countries invest at least 6% of their Gross Domestic Product (PIB) in health. The average investment in health in Latin America was 4.2% IN 2014 (Pan American Health Organization-OPS data) and increased of more than 6% in 14 countries in 2018 (CEPAL data).
In the last ten years has been the exponential growth of post-fracture care programs, especially FLS, which experienced an increase of 91% from 2013 to 2021, currently with 105 centers, according to the IOF – Capture the Fracture-Map of Best Practice (www.capturethefracture.org › map-of-best-practice), enrolling a total of 17,025 patients in Latin America.17
DiscussionThe present study gathered information from 19 out of 20 countries that comprised Latin America, which totals 630,534,000 inhabitants representing 98.2% of the region's population and a 10% growth since the 2012 report. Life expectancy has increased slightly by over a year to an average of 76.5 years vs 74.9 years in 2012.1 Our research shows that progress has been made over the past decade in terms of diagnosis and treatment of osteoporosis. However, Latin America primary challenge is to prioritize, and change improve clinical and reimbursement approach to osteoporosis is the lack of access to reliable national data for most of the countries in the region. Only 5/19 countries were able to submit data regarding the number and costs of fractures due to osteoporosis.
According to country data, fragility fractures are going up in Brazil, Colombia, and Peru, possibly in relation to the increase in life expectancy.
As shown in many other countries worldwide in the past decade,18,19 fragility fractures rates are decreasing in Mexico in both major health systems. From 2015 to 2019, fracture incidence rates in Chile fluctuated reaching 150 hip fractures per 100,000 inhabitants going back to the same 2015 rate per 100,000 inhabitants of 144 in 2019 as reported by Health statistics and reporting department of the Chilean Ministry of Health (www.deis.minsal.cl). Trends shown in Mexico are explained by demographic changes in the age of the cohorts in the population; if the population continues to age, in the coming decades this phenomenon will likely reverse20 will require further research to explain such behavior in hip fracture rates. No consistent behavior is observed in the incidence of other fracture types in between these five countries. The implementation of fracture prevention programs is expected to contribute to decreasing fracture rates in the future. Distal radius fractures are the most frequent in Brazil, Chile, Mexico, and Peru, while proximal humerus fractures are most frequent in Colombia (Sistema Integrado de Información de la Protección Social – SISPRO www.sispro.gov.co).1 Vertebral fractures are poorly identified and highly under-registered (only 30% reported according to IOF Compendium of Osteoporosis – Second Edition 2019), though. An intentional search of such fractures through lateral spine X-ray and/or VFA performed by DXA on women and men+65 years old is a recommended clinical practice to be included in national clinical guidelines throughout the region.
As previously stated, the lack of national registries and databases is the most urgent gap Latin American countries need to close. Where available, national databases are hard to access and/or incomplete. Healthcare providers together with osteoporosis-related societies and local experts, should work together on building trustable, accurate and accessible national data sets that measure the size of the problem osteoporosis and fragility fractures would become in the coming years in current rapid population aging scenarios.
The economic, social, and individual impact of osteoporosis and fragility fractures is invisible to healthcare decision makers due to lack of robust data which creates a serious limitation in driving significant policy change regarding the need of prevention campaigns and diagnosis and treatment reimbursement at a country level. As well, only Argentina, Brazil, Chile, Colombia, and Mexico reported implementation of post-fracture care programs such as FLS and/or orthogeriatric units in their hospitals. This is still an important opportunity to identify and treat the most high-risk patients at risk of secondary fractures.
Authors agree that a greater knowledge about the incidence and cost of osteoporosis and fragility fractures would lead to adapt to country specific epidemiology effective diagnosis tools such as the FRAX® algorithm, which is only available in 7 Latin American countries. FRAX® is a single, simple tool that would allow medical professionals to identify high risk patients and make treatment decisions at the primary level of care in a cost-effective manner. But, more importantly, at an early stage and before the first fragility fracture occurs while taking advantage of the wide range of anti-osteoporotic medications are available in most countries, with unequal access though.
The main methodological limitations of this study are the low participation in Phase 2 and difficulty in accessing national data.
One of the main findings of this study is the notable scarcity of data on fractures in numerous countries of the region. This deficiency represents both a methodological limitation for our research and an indicator of a broader public health problem. The absence of reliable records on fracture rates reflects on the one hand, deficiencies in health information systems and, on the other hand, a low prioritization of osteoporosis in the health policies of these countries.
In some countries, knowledge of epidemiological data and costs has already generated greater awareness about osteoporosis and fragility fractures driving government prevention and treatment policies.
ConclusionGiven the increasing high growth in elderly population, osteoporosis, and fragility fracture rates will rise in the Latin American region. Latin American countries should better comply with data collection to further support health policies that promote early diagnosis, treatment optimization and support fracture prevention programs, to avoid the true undesirable burden of osteoporosis which are fragility fractures.
Ethical considerationsThe authors declare that this article does not contain personal information that could identify patients.
FundingResearch and publication of this article was funded by the International Osteoporosis Foundation.
Conflicts of interestPatricia Clark: None.
Claudia Campusano: Honoraria as Speaker from Novartis, Tecnofarma, Adium, Faes-Farma.
Sonia Cerdas Pérez: Honoraria as Speaker from Novo Nordisk, Sanofi, Novartis, Procaps, Asofarma, MSD and Faes-Farma.
Bruno Muzzi Camargos: None.
Adriana Medina Orjuela: Honoraria as Speaker from Amgen, Elli Lily, Faes-Farma.
Contribución de los autoresConceptualización, análisis formal, investigación, metodología, administración de proyectos, supervisión, validación, visualización, redacción (borrador original), redacción (revisión) y edición: A. Medina, C. Campusano, S. Cerdas-Pérez y P. Clark.
Metodología, redacción (borrador original), revisión y edición: M. Calo y S. Wullich.
Investigación, redacción (borrador original) y revisión: B. Muzzi-Camargos.
We would like to thank contributors from each participating country in obtaining specific epidemiological data.
