



Ages and Stages Questionnaires: Social-Emotional Second Edition or ASQ: SE2 is a set of questionnaires to identify the social-emotional development of children from 6 to 60 months of age and is one of the most reliable measures of social development. This questionnaire has been adapted into several languages, but there is no version in Indonesian. This study aims to adaptation and validation the Ages and Stages Scale Social-Emotional Questionnaires – 2 (ASQ: SE2) for ages 2–5 for Indonesian children.
MethodsResearch procedures based on the guidelines for Translating and Adapting Tests, Second Edition, namely, forward translation, backward translation, and expert judgment to analyze the suitability of the adapted version item with the original version and confirmation through validity and reliability tests. The participants were 350 mothers with children aged 2–5 years. Test validity and reliability with confirmatory factor analysis (CFA).
ResultsThe CFA results of the ASQ: SE2 questionnaire aged 2–5 years obtained all indicators resulted in a loading factor value of >0.3. Construct Reliability (CR) values >0.7 and goodness of fit indicate that, on average, values have met three criteria for fit integrity. ASQ: SE2 for the age group of 2–5 years is declared valid and reliable.
ConclusionsThe ASQ: SE2 questionnaire is suitable to be applied as a measuring tool for screening social-emotional development in Indonesian children aged 2–5 years.
Los cuestionarios Edades y etapas: social-emocional, segunda edición (ASQ:SE2) son un conjunto de herramientas para identificar el desarrollo socioemocional de los niños de seis a 60 meses de edad y es una de las medidas más confiables de desarrollo social. Este instrumento ha sido adaptado a varios idiomas, pero no hay una versión en indonesio. Este estudio tiene como objetivo adaptar y validar los ASQ:SE2 para niños indonesios de dos a cinco años.
MétodosSe emplearon procedimientos de investigación basados en las directrices para la traducción y adaptación de pruebas, segunda edición, a saber, traducción hacia adelante, hacia atrás y el juicio de expertos para analizar la idoneidad del elemento de la versión adaptada en comparación con la original y la confirmación a través de pruebas de validez y fiabilidad. Las participantes fueron 350 madres con niños de dos a cinco años. La validez y fiabilidad de la prueba se valoraron mediante el análisis factorial confirmatorio (CFA).
ResultadosLos resultados del CFA del ASQ:SE2 en infantes de dos a cinco años obtuvieron todos los indicadores que dieron como resultado una cifra de factor de carga de >0,3. Los valores de confiabilidad de constructo (CR) >0,7 y la bondad de ajuste indican que, en promedio, han cumplido con tres criterios para la integridad del ajuste. El ASQ:SE2 para el grupo de edad de dos a cinco años se declara válido y confiable.
ConclusionesEl cuestionario ASQ:SE2 es adecuado para aplicarse como una herramienta de medición para el cribado del desarrollo socioemocional en niños indonesios de dos a cinco años.
Social-emotional development is closely related to the relationship between children with parents.1 The child's socio-emotional development competence has five domains. Children's first stage of socio-emotional development is self-awareness, namely the ability to recognize and understand one's own emotions, thoughts and behavior. Children who have good self-awareness can understand their strengths and weaknesses. The second stage is emotional management, namely the ability to control emotions and channel them in a healthy way. Children who have good emotional management skills can face challenges and failures in a constructive way.2
The third stage of socio-emotional development is self-motivation. This is the ability to set goals and work hard to achieve them. Children who have good self-motivation can overcome obstacles and achieve success. The fourth stage is social skills, namely the skill of interacting with other people in a positive and constructive way. Children who have good social skills can build strong relationships with others. The fifth stage of socio-emotional development is social understanding. This ability is the ability to understand other people's perspectives and empathize with them. Children who have good social understanding can cooperate with others and resolve conflicts peacefully.3–5
On the other hand, aspects of social competence generally mean how a child deals with friends and adults in society.6 Meanwhile, emotional competence is built on several dimensions, including the perception of one's own emotions, the perception of others’ emotions, emotional expressiveness, and emotion management.7 Self-regulation, social awareness, responsible decision-making, and social interaction skills are all part of social-emotional development.8 Socio-emotional competence is essential for cognitive development and learning behavior in childhood, and it influences social behavior and academic achievement.8
Developing socio-emotional competence is critical throughout a child's life and is a foundation for later success.9 Children with high levels of social-emotional competence outperform and complete more tasks. Moreover, they are more successful in their careers, and grow into more successful adults.10 However, children in early age with a lack of socio-emotional competence have a high risk of having negative behaviors.11 An earlier child who lacks empathy, and shows aggressive behavior, will eventually get a rejection by his peers.12 One of the factors influencing early childhood social-emotional competence is the family, where maternal knowledge supports socio-emotional development.13 Greater housing density and family composition play a role in lowering the risk of a child's behavior and socio-emotional development. Furthermore, child growth factors influence children's emotional development and behavior.14
A child's inadequate social-emotional development and behavior becomes a heavy burden for the family and society.15 Clinically delays in social-emotional development and behavioral difficulties often appear at three years.16 Moreover, it also affects psychosocial problems in adulthood.17 Behavioral and social-emotional challenges can also raise the likelihood of developing psychopathology later in life. Furthermore, early social-emotional blockages increase the possibility of school adjustments and poor academic performance. When children feel good about themselves, develop positive relationships with others, and know how to identify, express, and manage emotions, they tend to be better prepared to learn and succeed.9
Early detection of developmental issues or delays in childhood is critical for providing appropriate care.18 A child's socio-emotional skills measured at an early age can predict health and health behaviors. Thus, identifying specific risk indicators of delay in social-emotional development will inform efforts to maximize the effect of mental and academic competencies and children's mental health.19 Screening questionnaires are often used as the first step to briefly evaluating children and identifying children at risk of delays or problems that may require further assessment.20 Assessment of early childhood socio-emotional development consists of several developmental domains, including cognitive development and subdomains of social-emotional development.21
Measuring instruments for infants’ and toddlers’ social-emotional development have been widely developed in the last decade, including Ages and Stages Questionnaires. Those were Brief Infant-Toddler Social and Emotional Assessment months (BITSEA), Child Behavior Checklist 112–5 (CBCL), Infant-Toddler Social and Emotional Assessment (ITSEA), Devereux Early Childhood Assessment for Infants and Toddlers (DECA-I/T), Early Childhood Screening Assessment (ECSA), Greenspan Social-Emotional Growth Chart (SEGC), Merrill-Palmer-Revised Social-Emotional Growth Chart (SEGC), Merrill-P (SEAM). All of those measuring instruments are reliable and acceptable. However, only the Ages and Stages Questionnaires are among the most comprehensive tools and psychometrically sound measures. Social-Emotional – 2 (ASQ: SE2), BITSEA, CBCL, and ITSEA are the others.22
Various Ages and Stages Social-Emotional Questionnaires ASQ: SE2 stands for A Parent-Completed Child Monitoring System for Social-Emotional Behaviors.23 It is a set of questionnaires on the socio-emotional development of children aged 6–60 months that parents/caregivers can self-manage. A questionnaire was developed ASQ: SE2 is a multidimensional socio-emotional developmental screening instrument used to identify children at risk of socio-emotional developmental disorders. If a child gets a risky score, it is necessary to conduct a further assessment for a broader examination of the child's development compared to children of the same age.24 ASQ Questionnaire: SE2 adapted multiple languages, including Brazilian, Chinese, Korean, and Russian25 and Taiwan.26 However, there have been no questionnaire reports in the Indonesian version. Furthermore, Indonesia has no specific screening instrument to identify problems in children's social-emotional development.
ASQ: SE2 was developed in the United States and adapted to Indonesian culture and language. However, there are still some questions that may not be appropriate to Indonesian culture or language. This is because the ASQ: SE2 questionnaire was created based on culture in the United States. ASQ: SE2 is an instrument that can be filled out by parents or child caregivers. In addition, to get accurate results, questionnaire fillers must be literate in using ASQ: SE2. Trained personnel to fill out ASQ: SE2 in Indonesia are still very limited.24 Research needs to be carried out to identify ASQ: SE2 questions that may not be appropriate to Indonesian culture or language. These questions can be adapted to Indonesian culture and language to increase the validity and reliability of ASQ: SE2.15
In Indonesia, there is no specific screening test to assess socio-emotional development for preschool children ages 2–5.7 Development generally, developmental assessments use developmental pre-screening questionnaires (KPSP). At the same time, they measured emotional and mental deviation using the Emotional Behavior Problem Questionnaire.27 Denver Development Screening Test (DDST) or Denver II.28 KPSP and DDST assess child development in general, including motor development (gross and exemplary), language, personal social, and emotional development.
ASQ: SE2 needs to be implemented in Indonesia because in Indonesia, there are still many cases of children with delayed social-emotional development due to stunting. Children with this disorder can experience difficulties in socializing, learning and adapting to their environment. ASQ: SE2 can be used to detect delays in social-emotional development early, so that children can get the right intervention at the right time.
The practical implications of this research can be a reference for health services to use ASQ: SE2 to detect delays in the socio-emotional development of children under five who are affected by stunting. Therefore, adapting to this ASQ: SE2 questionnaire is necessary to pay attention to cultural differences. This study aims to adapt and validate the scale of the Age and Stage Questionnaire: Social-Emotional – 2 (ASQ: SE2) aged 2–5 years.
MethodData collectionData were collected from February to June 2022 after obtaining the ASQ: SE2 instrument aged 2–5 years from expert judgment's conformity and adaptation analysis results. Collected data directly from 350 mothers with children aged 2–5 years in Indonesia using the adapted version of the ASQ: SE2 instrument.
Data measurementASQ: SE2 were age group questionnaires of 24, 30, 36, 48, and 60 months. Several question items between 31 and 36 question items. The questionnaire does not include open-ended questions, so the number of questions is reduced from the original questionnaire. Assessments employ a Likert scale, i.e., frequently, consistently, occasionally, never, and require attention. The item score (Z=0, V=5, X=10, needs attention=5) is assigned to each answer choice. The categorization of child development is calculated based on the value limit of each questionnaire according to age. Cutoff based on age, namely age 24 months, indigo 50, age 30 months’ value 65, age 36 months’ value 75, age 48 value 70, and age 60 months’ value 70.
Based on the International Test Commission (ITC) Guidelines, the steps in the research include; precondition stage, researchers ask permission from the first author of ASQ: SE2, professor Jane Squires via email. Forward translation, the translation process of the ASQ: SE2 questionnaire from English into Indonesian, translated by psychologists who have good English skills and have lived abroad. The expert judgment is reviewing translational results. Example sentence “Is your child's body relaxed?”. Translating “Apakah anak Anda tampak santai?” review results “If what is meant is related to physique, then the translation is not “relaxed,” but “the body is relaxed.” Then another example, the word “tantrum” fixed translated into word “tantrum” and so on. Backward translation, the process is carried out by experts in English. Translators without seeing the original measuring instruments used in the study.
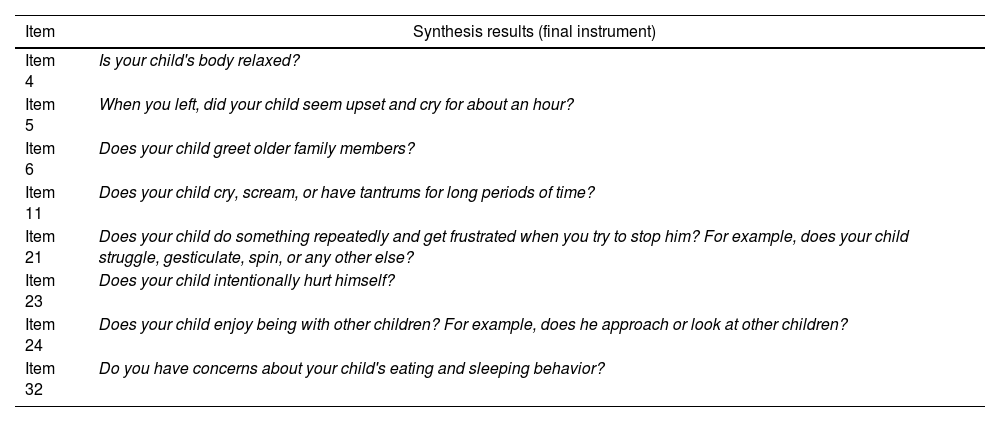
Furthermore, the process synthesis as a final questionnaire by expert judgment as proof of conformity between concept and meaning in items – items of the adapted version with the original version. The expert judgment provides a score of 1–4 for each question based on relevance, the importance of the question (priority), and clarity (clarity). This is done to obtain evidence of the instrument's validity through expert judgment by a specialist child development psychologist. In the expert judgment process, corrections and improvements are made to some items; if there are differences, they are discussed with the translator. Then, a questionnaire is determined that is ready to be used or as a result of synthesis. An example of the final ASQ Questionnaire: SE2 age 24 months can be seen in Table 1.
Final questionnaire Ages and Stages Questionnaires: Social-Emotional Second Edition (ASQ: SE2) age 24 months.
| Item | Synthesis results (final instrument) |
|---|---|
| Item 4 | Is your child's body relaxed? |
| Item 5 | When you left, did your child seem upset and cry for about an hour? |
| Item 6 | Does your child greet older family members? |
| Item 11 | Does your child cry, scream, or have tantrums for long periods of time? |
| Item 21 | Does your child do something repeatedly and get frustrated when you try to stop him? For example, does your child struggle, gesticulate, spin, or any other else? |
| Item 23 | Does your child intentionally hurt himself? |
| Item 24 | Does your child enjoy being with other children? For example, does he approach or look at other children? |
| Item 32 | Do you have concerns about your child's eating and sleeping behavior? |
While translating and adapting the ASQ: SE2 questionnaire, researchers faced several challenges that needed to be overcome. First, uncertainty in translating medical terms requires researchers to ensure the accuracy of interpretation that the lay public can understand, so a competent English expert in health education is chosen. Second, the focus was given to different levels of comprehension to improve questionnaire readability by implementing trials with target groups to ensure accessibility for varying levels of respondents’ understanding.24
Lastly, special attention is paid to translation consistency through the synthesis of results by involving focus group discussions between the research team and linguists. It was to do so to ensure questionnaires are technically accurate, relevant, and understandable to a diverse group of respondents. This combination of strategic approaches aligns with ASQ Questionnaire adoption research.29 The final step is to test the validity and reliability of the construct statistically. Validity and reliability test using confirmatory factor analysis (CFA) with the LISREL program.
Sample of the studyThe participants of this study were mothers with children aged 2–5 years, selected from five Community Health Centers (CHC) in Surabaya City: Jagir, Wonokromo, Wiyung, Kebonsari, and Kalirungkut. The five CHCs were chosen to reflect the community's condition in Surabaya City, East Java Province, Indonesia, where the questionnaire will be used. The total number of samples involved in this study was 350.
This study's participants were mothers who had children aged 2–5 years from 24, 30, 36, 48, and 60 months. The research samples were collected from five public health workers at the Surabaya City Health Office. There were 350 people in attendance. The number of pieces in this study is based on the provisions of valid criteria in the CFA analysis or can be considered good if the loading factor is greater than 0.30, i.e. 350 samples.30
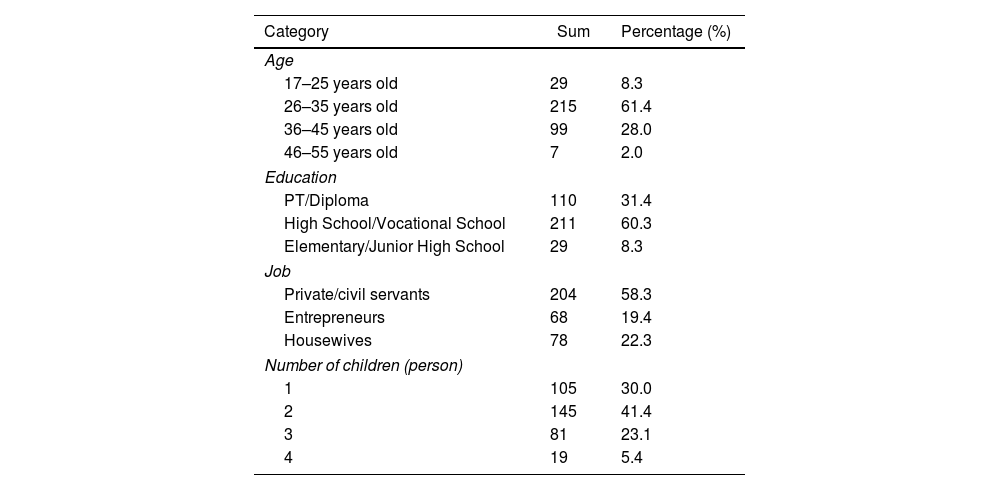
The 350 participants in this study were selected based on inclusion criteria that significantly differentiated samples from non-samples to avoid the risk of non-responsive bias. These criteria are having received parenting education in the digital era, having received material on the psychology of toddler development both at school and at home, understanding the ASQ: SE2 concept and being willing to learn to apply it, having a high level of literacy about child psychology. Respondents filled out a questionnaire, first expressing willingness to participate in the study. The Health Research Ethics Commission, Faculty of Public Health, Diponegoro University, has declared this research protocol ethically feasible (No: 57/EA/KEPK-FKM/2022). Participant demographic data information is in Table 2.
Participant demographic data.
| Category | Sum | Percentage (%) |
|---|---|---|
| Age | ||
| 17–25 years old | 29 | 8.3 |
| 26–35 years old | 215 | 61.4 |
| 36–45 years old | 99 | 28.0 |
| 46–55 years old | 7 | 2.0 |
| Education | ||
| PT/Diploma | 110 | 31.4 |
| High School/Vocational School | 211 | 60.3 |
| Elementary/Junior High School | 29 | 8.3 |
| Job | ||
| Private/civil servants | 204 | 58.3 |
| Entrepreneurs | 68 | 19.4 |
| Housewives | 78 | 22.3 |
| Number of children (person) | ||
| 1 | 105 | 30.0 |
| 2 | 145 | 41.4 |
| 3 | 81 | 23.1 |
| 4 | 19 | 5.4 |
Table 2 shows that the demographic data of participants are generally between 26 and 35 years old (61.4%), with the highest percentage of high school/vocational education level e (60.3%), the highest employment status as a civil servant/private sector (58.3%) and having two children (41.4%).
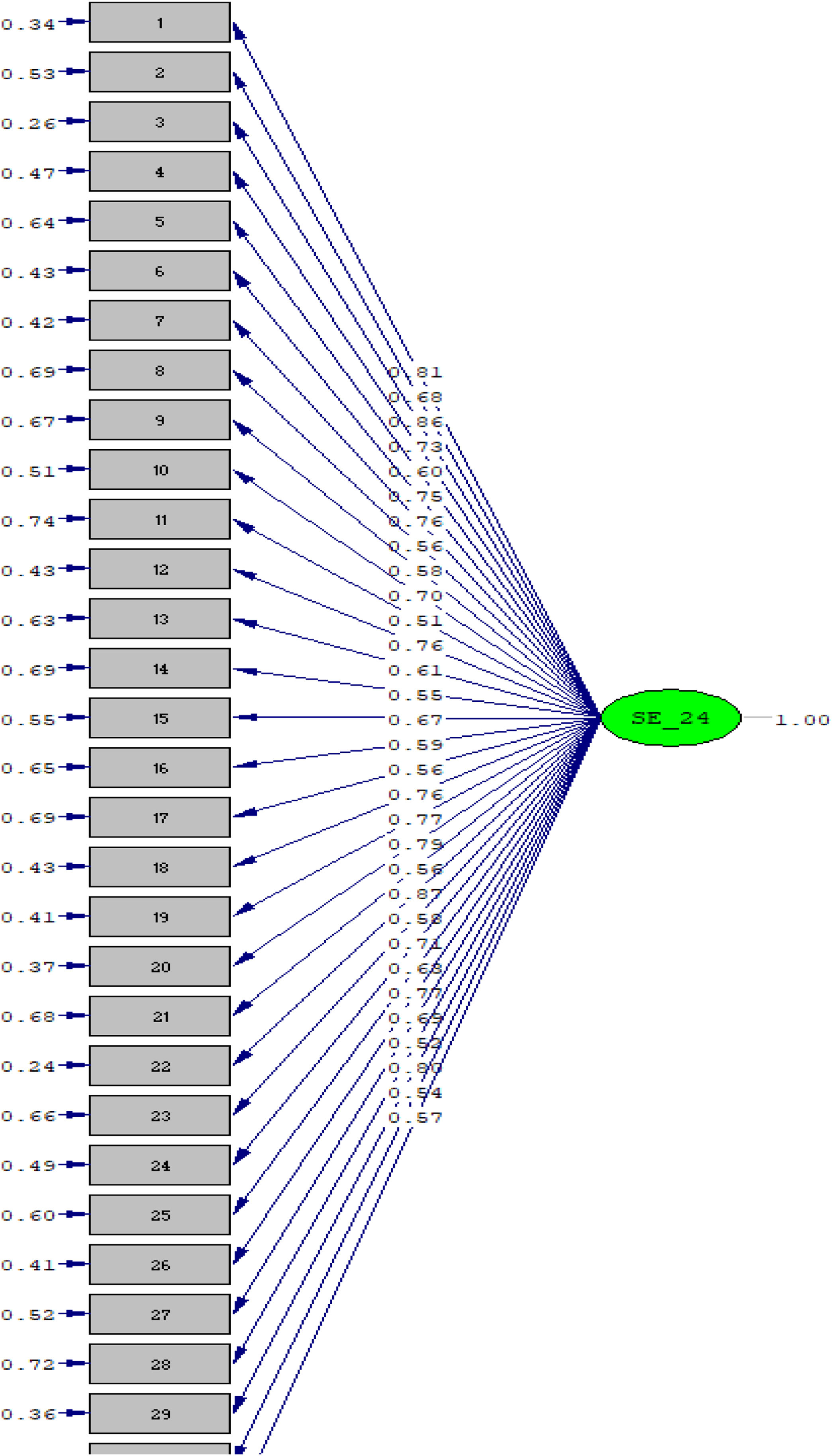
ResultsThe results of the validity test analysis through the calculation of confirmatory factor analysis obtained throughout the questionnaire from each age group obtained a loading factor value greater than 0.5. Indicates that the indicator is valid for measuring instrument construction, or its interpretation could be that the needle is declared valid as a data collection tool—test the validity of the ASQ: SE2 questionnaire for each age group. Examples of validity test results of ASQ Questionnaire validity results: SE2 aged 24 and 30 months are shown in Fig. 1.

Fig. 1 shows that out of 31 question items, the validity test results of all indicators result in a loading factor value greater than 0.5. This suggests that each question has a fairly strong relationship with the latent variable. Three question items score above 0.8, which is question no. 1, 3, and 22, signifies that these questions have a very high contribution to the validity of the instrument at 24 months of age.
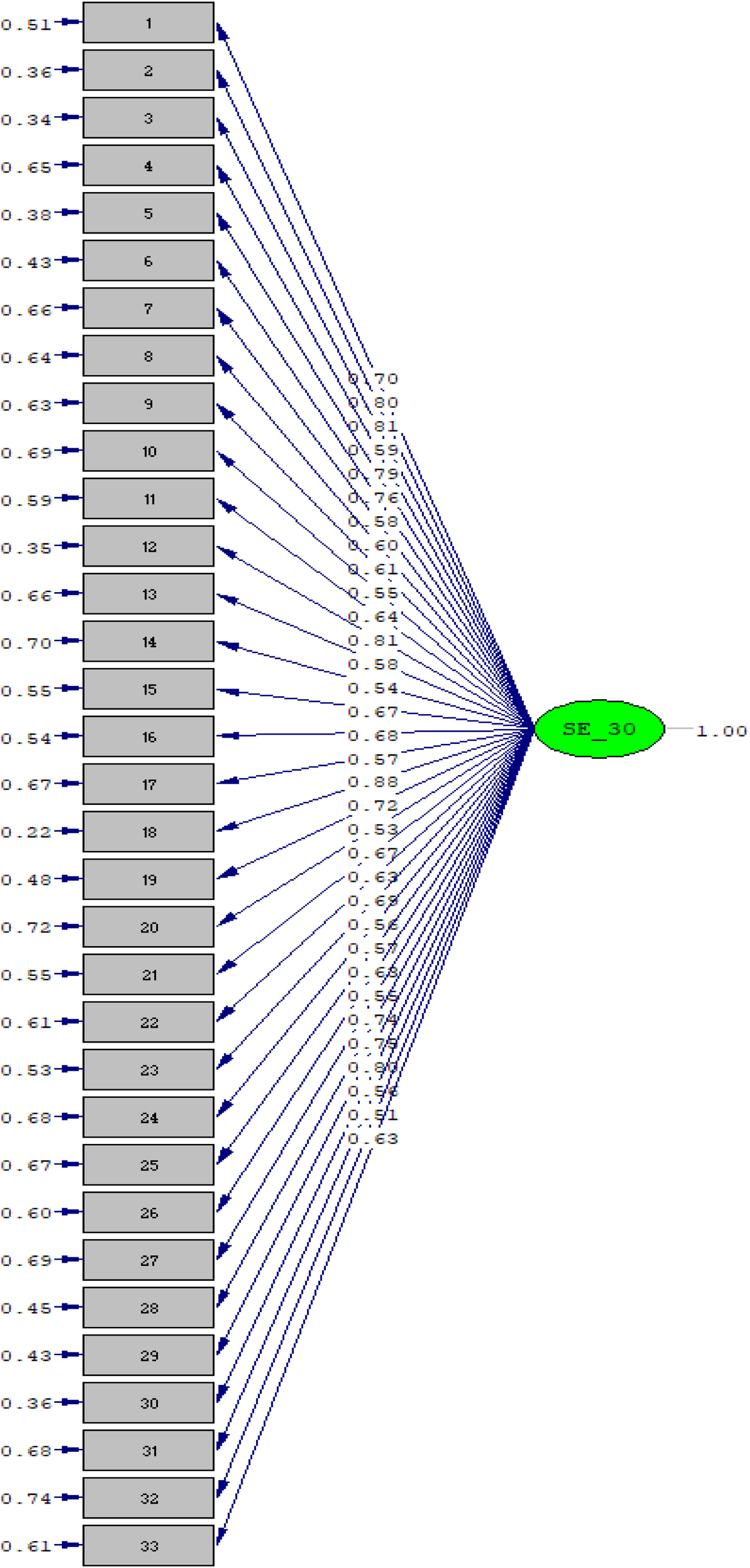
Fig. 2 shows that all indicators of the 33 question items produce a loading factor value greater than 0.5, and those that obtain values above 0.8 are found in question items no. 3, 12, and 18. Furthermore, as well as the results of validity tests in the age groups of 36, 48 and 60 months showed all indicators produced a loading factor value greater than 0.5. In the 36-month age group, there were 35 questions, which obtained scores above 0.8 as many as six questions, namely no. 23, 26, 29, 33, 34, and 35. In the age group of 48 there were 36 questions, which obtained scores above 0.8 in questions no. 3, 4, 14, 27, and 29. While the 60-month age group totaled 36 questions, which obtained scores above 0.8 on questions no. 3, 4, 14, 27, and 29.

Overall, the confirmatory factor analysis (CFA) analysis results in this study show that all indicators have a load factor value above 0.5, meaning that the correlation is quite strong with the measured construct. Loading factor values greater than 0.5 are generally considered strong correlations, while matters less than 0.3 are considered weak. The loading factor value ranges between −1 and 1. The closer the loading factor value is to 1, the stronger the relationship between the measured variable and the latent factor. A low loading factor value (close to 0) indicates that the measured variable does not correctly calculate the construct in question or may display a problem in formulating or interpreting the question.
Table 3 also shows the results of the reliability test analysis on all ASQ: SE2 questionnaires based on age groups of 24, 30, 36, 48, and 60 months, with each variable Construct Reliability (CR) value greater than 0.7 in this study.
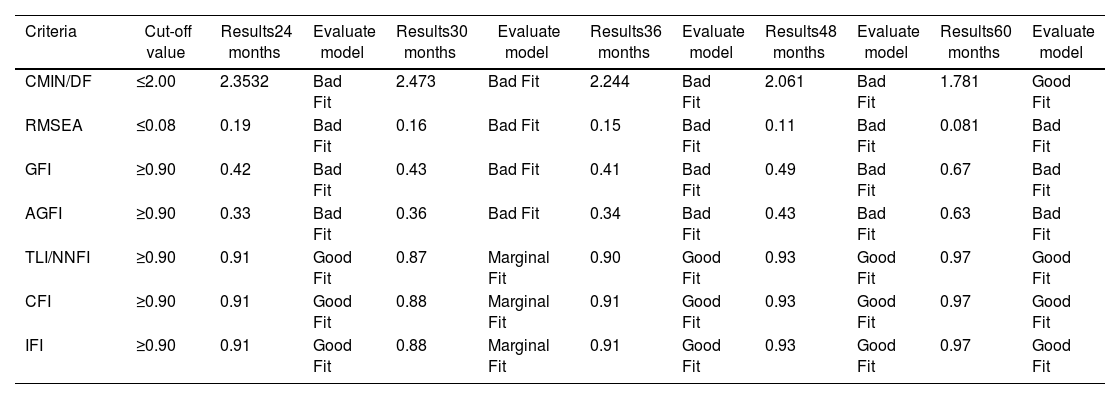
Table 4 shows the results of the analysis or statistics of goodness of fit and fit model criteria in all average age groups show that three goodness of fit criteria have met the cut-off value, namely TLI/NNFI, CFI, and IFI show good results or meet the criteria in some age groups, but not in all. Some results show “Bad Fit,” especially at CMIN/DF values that exceed the cutoff of 2.00 and RMSEA that is greater than 0.08.
The goodness of fit results.
| Criteria | Cut-off value | Results24 months | Evaluate model | Results30 months | Evaluate model | Results36 months | Evaluate model | Results48 months | Evaluate model | Results60 months | Evaluate model |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CMIN/DF | ≤2.00 | 2.3532 | Bad Fit | 2.473 | Bad Fit | 2.244 | Bad Fit | 2.061 | Bad Fit | 1.781 | Good Fit |
| RMSEA | ≤0.08 | 0.19 | Bad Fit | 0.16 | Bad Fit | 0.15 | Bad Fit | 0.11 | Bad Fit | 0.081 | Bad Fit |
| GFI | ≥0.90 | 0.42 | Bad Fit | 0.43 | Bad Fit | 0.41 | Bad Fit | 0.49 | Bad Fit | 0.67 | Bad Fit |
| AGFI | ≥0.90 | 0.33 | Bad Fit | 0.36 | Bad Fit | 0.34 | Bad Fit | 0.43 | Bad Fit | 0.63 | Bad Fit |
| TLI/NNFI | ≥0.90 | 0.91 | Good Fit | 0.87 | Marginal Fit | 0.90 | Good Fit | 0.93 | Good Fit | 0.97 | Good Fit |
| CFI | ≥0.90 | 0.91 | Good Fit | 0.88 | Marginal Fit | 0.91 | Good Fit | 0.93 | Good Fit | 0.97 | Good Fit |
| IFI | ≥0.90 | 0.91 | Good Fit | 0.88 | Marginal Fit | 0.91 | Good Fit | 0.93 | Good Fit | 0.97 | Good Fit |
The adaptation of the ASQ: SE2 questionnaire in Indonesia was carried out to meet the urgent need for socio-emotional screening tests in children aged 2–5 years. This study aims to evaluate the quality of translations and check consistency with the original English version, with the hope of providing a valid monitoring tool for children's social-emotional development for parents living in the city of Surabaya, Indonesia. The sample size meets the valid criteria in CFA analysis with a loading factor of >0.30, which is 350 samples.30 The study had received ethical approval, but parents were given detailed information and written consent before data collection. In addition, using anonymous identities ensures data security and protection of children's privacy.
Respondents mainly consisted of mothers aged between 26 and 35 years, and the characteristics of most respondents being highly educated and working in the private sector or civil servants could also give rise to non-response bias, especially among respondents with low education—secondary education or housewife. Therefore, data was collected by contacting again and compiling appropriate messages for the older age group. In addition, careful sample selection was carried out to ensure equal representation of different age groups to increase the validity of the research results.31–34
ASQ: SE2 questionnaire Adaptation procedure for 2–5-year-olds using International Test Commission (ITC) Guidelines adaptation approach Guidelines for Translating and Adapting Tests (Second Edition).35 In the forward translation stage to Indonesian, there were differences in meaning in some questionnaire question items with the original language of the ASQ: SE2 measuring instrument in each age category. Similarly, the outcomes of backward translation.
The results of the two translators’ forward–backward translations are then reviewed by expert judgment and discussed among the translators to determine the synthesis or final version of the questionnaire, as shown in the questionnaire's final table. Synthesis results on several items based on age categories, namely; (1) age 24 months, items no. 4, 5, 6, 11, 21, 23, 24, and 32. (2) Only item no. 2 is 30 months old. (3) Age 36 months, items 5, 15, 19, 21, and 32. (4) Age 48 months, items no. 4, 8,10, and 22. (5) Age 60 months, items no. 5, 9, 10, 11, and 22.
Synthesis results on several items based on age categories, namely; (1) age 24 months, items no. 4, 5, 6, 11, 21, 23, 24, and 32. (2) Only item no. 2 is 30 months old. (3) Age 36 months, items 5, 15, 19, 21, and 32. (4) Age 48 months, items no. 4, 8,10, and 22. (5) Age 60 months, items no. 5, 9, 10, 11, and 22. The results of the back translation review show differences in understanding and interpretation between statements on the original scale and back translation. The discrepancy highlights the impact of cultural factors on the performance of questions and respondents’ responses to questionnaires. For example, the results of a review of the ASQ: SE2 questionnaire aged 24 months at no. 11, the statement “Does your child cry, scream, or have tantrums for a long time?” showed that there was a significant difference between the meaning of “emotionally upset” and “tantrum,” where tantrum is defined as more than just sadness or emotional discomfort, involves non-adaptive behaviors such as hurting others or oneself.
ASQ Questionnaire: SE2 age 24 months, in Fig. 1, has a good level of validity. There are three questions scored above 0.8 out of 31 with loading factor values ranging from 0.5 to 0.8, namely nos. 1, 3, and 22. These questions describe the child's social-emotional development, which is heavily influenced by adults, and the child's ability to regulate thoughts, actions, and emotions.36 A CR value of 0.963, >0.90, means perfect reliability; this shows that the question is consistent, reliable, and feasible to use as a data collection tool. In the goodness of fit results, there are three good fit criteria, namely TLI/NNFI, CFI, and IFI, which indicates that the evaluation results show a good model.37
ASQ Questionnaire: SE2 age 30 months, Fig. 2 obtained the result that all indicators of 33 question items produced a loading factor value greater than 0.5, and those obtained values above 0.8 were found in question items no. 3, 12, and 18. Questions include the child's attachment to the mother, compliance with the commands, and sleep time of at least 8h. Discipline can already be administered, but the method or methods of disciplining parents with hostility will have an impact on the child's social-emotional development.38 Parental education interventions delivered in the community can benefit a child's socio-emotional development.39 A CR value of 0.963, >0.90, has perfect reliability; this shows that the question is consistent, reliable, and worthy of use as a data collection tool. In the goodness of fit results, there are three marginal fit criteria, namely TLI/NNFI, CFI, and IFI, which means that the evaluation results are in a good model category.
ASQ Questionnaire: SE2 age 36 months, obtained the result that all indicators produced a loading factor value greater than 0.5 for the number of 35 question items, which received a deal more significant than 0.8 were six questions, namely no. 23, 26, 29, 33, 34, and 35. Questions related to the child's alertness, knowing friends and how the child behaves, the adequacy of sleep time, and the anxiety of both the child and the surrounding environment. In this condition, parents can teach toddlers to be separated without difficulty, express feelings, listen and respond to toddlers’ emotions and read stories before going to bed.40 A CR value of 0.976, >0.90, means that reliability is perfect; this shows that the question is consistent, reliable, and worthy of use as a data collection tool. In the goodness of fit results, there are three good fit criteria, namely TLI/NNFI, CFI, and IFI, which means that the evaluation results show a good model.15
ASQ Questionnaire: SE2 age 48 months, obtained results that all indicators produced a loading factor value greater than 0.5, consisting of 36 questions, and CR values above 0.8 were found in questions no. 3, 4, 14, 27, and 29. The five questions describe the child's relationship with friends and people around him and his emotions in expressing happiness and anger. Mistakes in providing treatment to children at this time will impact emotional abuse, developmental delays, emotional neglect, and exposure to violence by people in the surrounding environment other than caregivers.41,42 A CR value of 0.978>0.90, means that reliability is perfect; this indicates that the question is consistent, reliable, and worthy of use as a data collection tool. In the goodness of fit results, there are three good fit criteria, namely TLI/NNFI, CFI, and IFI, which means that the evaluation results show a good model.
The ASQ: SE2 questionnaire aged 60 months, the results were obtained that all indicators produced loading factor values greater than 0.5. The number of question item 36, which received a score above 0.8, is found in question no. 3 and 18 are about the child's closeness or attachment and the delivery of the child's wishes to the parents. The results showed that parental affection and Parental Reflective Functioning (PRF) are related to children's attachment, emotional ability, and psychopathology.43 A CR value of 0.968, >0.90, means that reliability is perfect; this shows that the question is consistent, reliable, and feasible to use as a data collection tool. The goodness of fit results, there are three good fit criteria, namely TLI/NNFI, CFI, and IFI, which means that the evaluation results show a good model.
Overall, it can be concluded that the results of the validity test output path obtained as a whole statement items 33–36 from the ASQ: SE2 questionnaire aged 24–60 months have a good level of validity, i.e., loading factor ≥0.30, so that it can be accepted. Likewise, the reliability test results found that this study's value of Construct Reliability (CR) was more than 0.7. The conclusions of all valid question items in this study are declared consistent, reliable, and feasible to be used as a data collection tool. Likewise, the results of the goodness of fit analysis or statistics, where the fit model criteria in all average age groups show that three goodness of fit criteria has met the cut-off value.21 It means that the evaluation results show a good model so that the ASQ: SE2 questionnaire for the age category, 24, 30, 36, 48 and 60 can be used for detection of socio-emotional development in Indonesia.
The results of the adaptation of ASQ: SE2, a questionnaire designed to assess the socio-emotional development of Indonesian children aged 2–5 years, have positively impacted the early childhood education (ECD) sector. This questionnaire can increase the effectiveness of ECE in identifying children who need additional support and guide the development of appropriate intervention programs. The impact of screening results can help shape more targeted child protection policies. In contrast, parents’ participation in screening allows them to support their children's growth and development at home. Implementation of adaptive outcomes also encourages collaboration between sectors and ensures comprehensive support for children's optimal social-emotional development. Therefore, adapting this research will improve the monitoring of children's stories and provide a basis for improving early childhood education policies and practices in Indonesia.
A similar study was also conducted in China; the results of the validity test of the ASQ: SE2 representative questionnaire were used to detect the social-emotional development of Chinese children.38 ASQ: SE has a high detection rate of social-emotional problems in early childhood. Internationally shows moderate to good sensitivity of 71–85% and excellent specificity of 90–98% in the child's socio-emotional development.29 The ASQ: SE questionnaire only takes 10–15min to complete for the caregiver. The child's total performance score is obtained by adding points from all items on the questionnaire. A higher total score indicates more problems with social-emotional behavior.25
ConclusionsMultiple Ages and Stages ASQ: SE2, a version of the country, has undergone an adaptation process based on the International Test Commission (ITC) Guidelines for Translating and Adapting Tests (Second Edition) measuring instrument adaptation guidelines.
The validity and reliability test results obtained from all question items on the ASQ: SE2 questionnaire based on the age groups of 24 months, 30 months, 36 months, 48 months, and 60 months were consistent, reliable, and reliable. In all average age groups, three goodness of fit criteria (CMIN/DF, RMSEA, GFI, AGFI, TLI/NNFI, CFI, and IFI) met the cut-off value, indicating that the evaluation results revealed a good model. Thus, this model is reasonable and feasible for explaining the relationship between variables used as a screening tool for social-emotional development in an Indonesian population of children aged 2–5 years.
FundingThis research is not supported by any funding source. Allcosts associated with the study are fully borne by the author.
Conflict of interestThe author(s) stated that there are no possible conflicts of interest regarding the research, authorship, and/or publication of this article.
We would like to express our sincere gratitude to all the mothers of 2–5-year-old children who participated in this research. We also extend our heartfelt thanks to the entire team of enumerators, including the interviewers, data entry operators, and data analysts. Their tireless efforts and unwavering commitment have been instrumental in the success of this study. We are truly grateful for their valuable contributions to our research project.
