




To determine the prevalence of anxiety, depression and stress on Argentinian university students, their risk factors, concerns and coping skills.
MethodA cross-sectional study was conducted in college students from Argentina, using a survey spread on social networks.
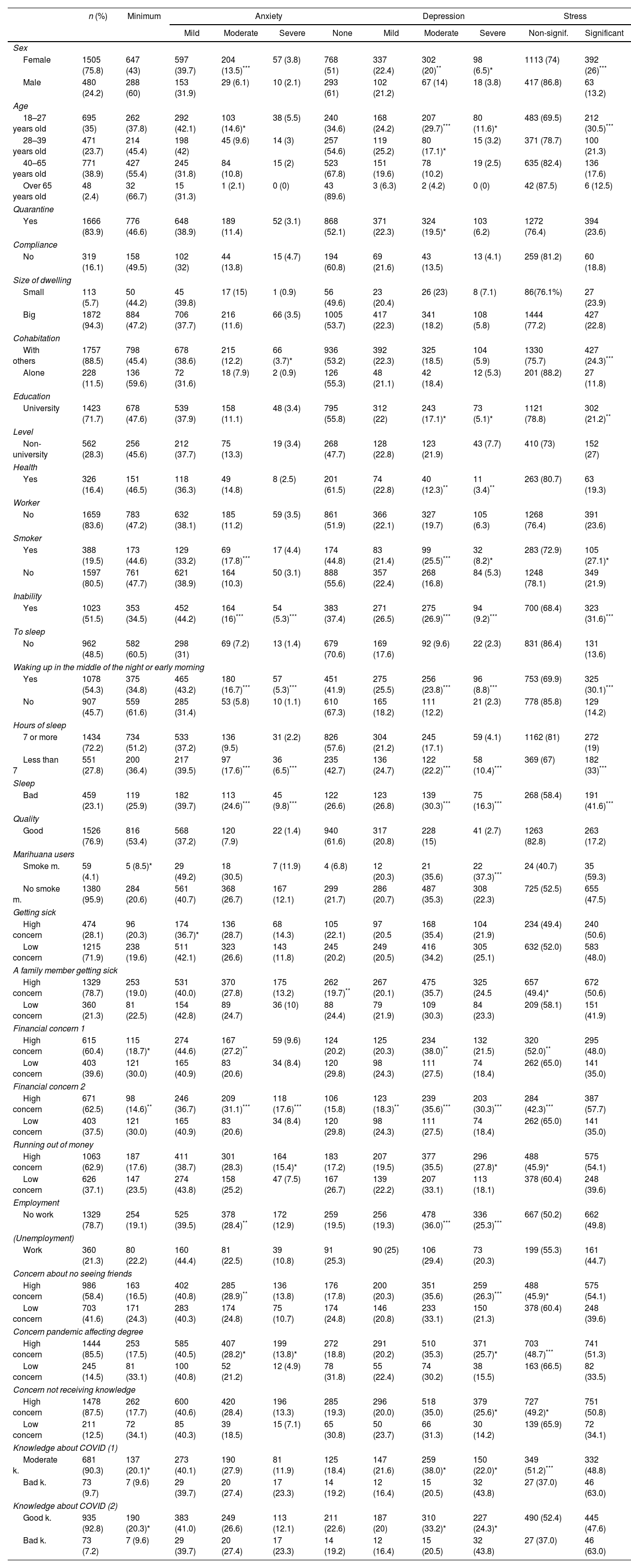
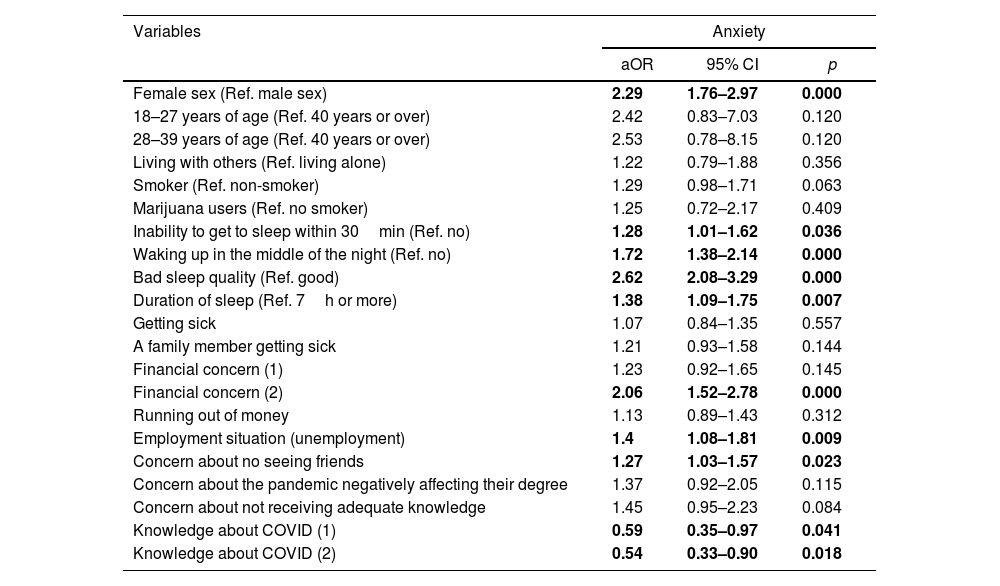
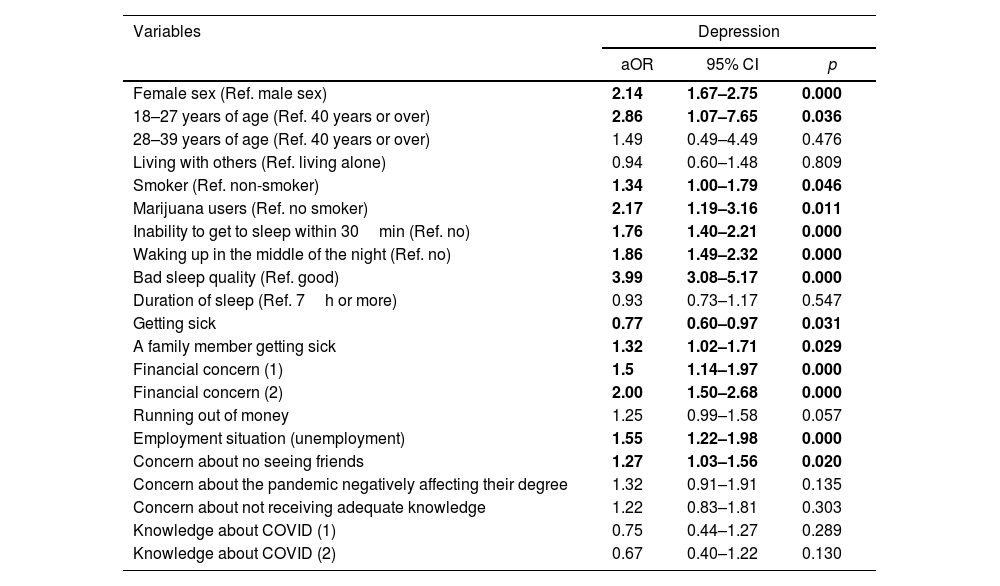
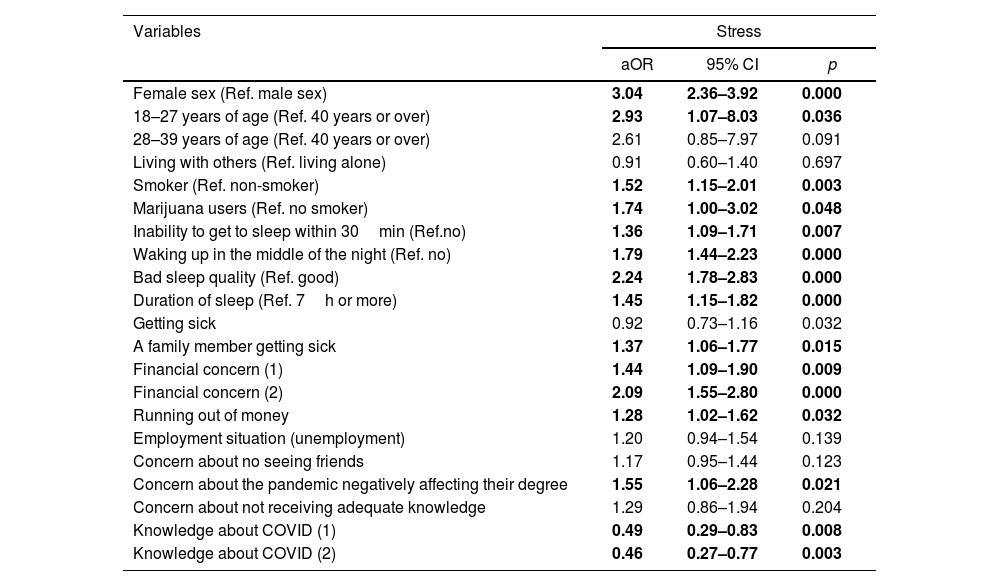
ResultsOf 1711 surveyed students, 40.67% experienced moderate/severe anxiety, 58.03% experienced moderate/severe depression, 48.01% experienced stress and 68.8% reported insomnia. Females (aOR: 2.14; 95% CI: 1.67–2.75), young people (aOR: 2.86; 95%CI: 1.07–7.65), smokers (aOR: 1.34; 95% CI: 1.005–1.79), users of marijuana (aOR: 2.17; 95% CI: 1.19–3.96) and participants with poor sleep quality (aOR: 3.99; 95% CI: 3.08–5.17) were more affected. Economic concerns (aOR: 2.95; 95% CI: 1.50–2.68), unemployment (aOR: 1.55; 95% CI: 1.02–1.56) and concern about not seeing friends (aOR: 1.27; 95% CI: 1.03–1.56) were associated with increased risk of having the conditions mentioned above.
ConclusionsThe psychological impact caused by the long-term confinement is greater on Argentinian university students than on the general population.
Determinar la prevalencia de ansiedad, depresión y estrés en estudiantes universitarios argentinos, los factores de riesgo, sus preocupaciones y métodos de afrontamiento utilizados.
MétodoSe efectuó un estudio transversal en estudiantes universitarios argentinos, utilizando una encuesta diseminada por redes sociales.
ResultadosDe los 1.711 estudiantes encuestados, 40,67% experimentaron ansiedad moderada/severa, 58,03% depresión moderada/severa; 48,01% estrés significativo y 68,8% reportaron insomnio. Las mujeres (razón de probabilidad ajustada [aOR]: 2,14; intervalo de confianza [IC] 95%: 1,67-2,75), la gente más joven (aOR: 2,86; IC 95%: 1,07-7,65), los fumadores (aOR: 1,34; IC 95%: 1,005-1,79), consumidores de marihuana (aOR: 2,17; IC 95%: 1,19-3,96) y los participantes con mala calidad de sueño (aOR: 3,99; IC 95%: 3,08-5,17) estuvieron más afectados. Las preocupaciones económicas (aOR: 2,95; IC 95%: 1,50-2,68), el desempleo (aOR: 1,55; IC 95%: 1,02-1,56) y la preocupación por no ver a sus amigos (aOR: 1,27; IC 95%: 1,03-1,56) estuvieron asociados con mayor riesgo de padecer las condiciones arriba mencionadas.
ConclusionesEl impacto psicológico causado por un confinamiento más prolongado es mayor en estudiantes universitarios argentinos que en la población general.

