





Número especial: Avances y retos en la psiquiatría regional en Latinoamérica
Más datosThe prevalence of mixed dementia (MixD), defined as the coexistence of Alzheimer's disease (AD) and vascular dementia (VaD), is likely to increase as the population ages. The five-word test (5WT) is a neuropsychological test that differentiates between major and mild neurocognitive disorder (NCD). The objective of the study is to validate 5WT for the detection of MixD.
Methods230 participants were evaluated: cognitively healthy (CH) (n=70), mild NCD (n=70), and major NCD (n=90): AD (n=30), VaD (n=30), and MixD (n=30). The Spearman's coefficient, d Sommer and ROC curves were used to determine the construct validity of the 5WT. The linear regression model was performed to determine the association between age and education with 5WT performance.
ResultsThe mean age was 79 ±7.7 years (P≤.001), 58% were female (P=.252), and the mean education was 9 ±5.3 years (P≤.001). Construct validity when comparing 5WT and MMSE was: Spearman's correlation ρ=.830 (P<.001) and d Sommer=.41 (P<.001). The area under the curve in the total weighted score (TWS) for MixD was .985, with 98% sensitivity (95%CI, 0.96-1.00) and 99% specificity (95%CI, 0.94-1.00), PPV of 88% (95%CI, 0.82-0.89), NPV of 100% (95%CI, 0.96-1.00), and cut-off point ≤16/20 (P<.001).
Conclusions5WT is a rapid test with neuropsychological validation for the exploration of cognitive characteristics in major NCD type MixD, regardless of age and education.
Es probable que la prevalencia de la demencia mixta (DMix), definida como la coexistencia de enfermedad de Alzheimer (EA) y demencia vascular (DVa), aumente a medida que la población envejece. El test de 5 palabras (5WT) es una prueba neuropsicológica que diferencia entre el trastorno neurocognitivo (TNC) mayor y el menor. El objetivo del estudio es validar el 5WT para la detección de DMix.
MétodosSe evaluó a 230 participantes cognitivamente sanos (CS) (n=70) y con TNC menor (n=70) y TNC mayor (n=90): EA (n=30), DVa (n=30) y DMix (n=30). Se utilizó el coeficiente rho de Spearman, d Sommer y las curvas ROC para determinar la validez de constructo del 5WT. Se realizó el modelo de regresión lineal para determinar la asociación entre la edad y la educación en el rendimiento del 5WT.
ResultadosLa media de edad fue 79±7,7 años (p ≤ 0,001), el 58% eran mujeres (p=0,252) y la escolaridad media, 9±5,3 años (p ≤ 0,001). La validez de constructo al comparar el 5WT y el MMSE fue: ρ=0,830 (p <0,001) y d Sommer=0,41 (p <0,001). El área bajo la curva en la puntuación total ponderada (PTP) para DMix fue 0,985, con sensibilidad del 98% (IC95%, 0,96-1,00) y especificidad del 99% (IC95%, 0,94-1,00), con un valor predictivo positivo del 88% (IC95%, 0,82-0,89) y un valor predictivo negativo del 100% (IC95%, 0,96-1,00), con un punto de corte ≤ 16/20 (p <0,001).
ConclusionesEl 5WT es una prueba rápida con validación neuropsicológica para la exploración de características cognitivas en el TNC mayor tipo DMix independientemente de la edad y la educación.
Alzheimer's disease (AD) and vascular dementia (VaD) represent the two most frequent types of dementia.1–3 The current diagnosis of neurodegenerative dementias is based on neuropsychological evaluation, neuroimaging studies and biomarkers (β amyloid, phosphorylated tau protein and total), among other proteins.4 Delay et al., in 1962, described for the first time the association of the two types of lesions (vascular and degenerative) in the same patient and called it mixed dementia (MixD).
Chui et al. established that the diagnosis of MixD should be made in the presence of ischemic vascular disease and a second systemic or cerebral disorder (for example, AD, hypothyroidism, Parkinson's disease), which could be causally related to dementia.5 The diagnostic criteria of the National Institute of Neurological Disorders and Strokes - Association Internationale pour la Recherche et l’Enseignement en Neurosciences (NINDS-AIREN)6 for VaD they do not include a category for MixD, so it is recommended to use the term AD with cerebrovascular disease.7,8 Alternatively, the Hachinski ischemic score,9 the International Classification of Diseases (ICD-10), and the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) in their fourth edition, include MixD, although in all cases, they lack specific diagnostic criteria. However, the term MixD is widely recognized and is the most used to refer to the combination of AD and VaD.2,3
The current consideration of cardiovascular risk factors, not only for vascular pathology, but also for neurodegeneration, currently justifies the appearance of combined forms of dementia. The Vascular Impairment of Cognition Classification Consensus Study (VICCCS) proposes in its classification of vascular cognitive impairment, the definition of MixD, which includes phenotypes that represent a combination of vascular and neurodegenerative disease, that is, Vascular Cognitive Impairment - AD or Dementia with Lewy bodies, and as well as other combinations.10
The MixD prevalence range varies markedly between neuropathological studies (0% to 55%), this as a consequence of conceptual differences, as well as due to the diagnostic difficulty due to clinical and neuropsychological evaluation.11,12
Subjects with MixD present focal motor or sensory findings, gait disorder, and depressed mood, however, none of these characteristics is predictive of severity of cognitive impairment.2 In the neuropsychological evaluation, the mixed cognitive profile is characterized by a decrease in verbal fluency, both phonological and semantic, failure to recognize in memory tasks, and specifically, in the clock drawing test, difficulties have been identified for both reproduction and reading, which is explained by the alterations in executive functioning, visuospatial, visuoconstructive abilities and conceptual failures.11 Furthermore, the presence of ischemic lesions on computed tomography or magnetic resonance imaging are key in the diagnosis of individuals with MixD.13–15
The 5-word test (5WT) allows a rapid evaluation of episodic verbal memory.16 In addition, it has proven to be simple and valid for the identification of cognitive disorders, therefore, it can be culturally adapted to a different medium than the one developed and in addition to preserving its methodological qualities for screening for dementia. The 5WT has been shown to have good sensitivity and specificity for assessing episodic memory in patients with AD compared to people with subjective memory complaint.17 Likewise, it is also a useful test to assess executive function in patients with frontotemporal dementia and AD.18 According to these findings in these types of dementia and considering the MixD criteria (cortical and subcortical cognitive profile), it is possible to consider the usefulness of this test in this form of dementia figure 1.

Areas under receiver operating characteristics curves in five word test. Calculation with 95% confidence interval. A: ROC 5WT curve versus MMSE in mild NCD. B: ROC 5WT curve versus MMSE in major NCD type Alzheimer's disease. C: ROC 5WT curve versus MMSE in major NCD type vascular dementia. D: ROC 5WT curve versus MMSE in major NCD type mixed dementia. 5WT: five word test; AUC: area under the ROC curve; MMSE: Mini–Mental State Examination; NCD: neurocognitive disorder; ROC: receiver operating characteristic.
The objective of our study is to validate 5WT for diagnostic screening for MixD, compared to cognitively healthy people (CH), neurocognitive disorder (NCD) type AD and type VaD.
Material and methodsType of study and participantsCross-sectional validation study, which included 230 participants over 60 years of age, from the Memory Disorders Clinic in a tertiary referral hospital in Mexico City in a period from March 2019 to 2020. All the participants signed the informed consent and underwent a clinical and cognitive evaluation by the specialist in geriatrics and/or neurology and neuropsychology. The selection of the participants was non-probabilistic and for convenience. We included all patients diagnosed with major NCD: MixD, AD, VaD. The diagnosis of Alzheimer's disease was established based on the criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association NINCDS/ADRDA,19 and the Clinical Scale of Dementia with CDR of 1 (Mild) or 2 (Moderate). The established criteria of the Diagnostic and Statistical Manual of Mental Disorders version 5 (DSM-5)20 were also used. VaD was established based on the criteria (NINDS/AIREN);6 MixD includes phenotypes representing each combination between vascular and neurodegenerative disease, that is, VaD-AD or AD-VaD according VICCCS criteria for MixD.10
Petersen's criteria were used to establish the diagnosis of Mild NCD21 and the Clinical Scale of Dementia (CDR=0.5).
The comparison group or cognitively healthy (CH) was made up of those who performed cognitively normal, who had no subjective memory complaint, had a result >26 in the MMSE and obtained a CDR=0.
The neuropsychologist who evaluated the cognitive profiles of the patients was an expert who remained blind to the diagnostic category throughout the study.
The neuropsychologist assessing patients’ cognitive profiles was an expert in diagnosing who remained blind to the diagnostic category throughout the study which include neuropsychological function was assessed on the Mini-Mental State Examination (MMSE), which is a simple instrument that allows identifying probable cognitive impairment with a cut-off point ≤24/30;22,23 the clock-drawing test is a widely used screening test that has several scoring methods, both quantitative and qualitative, we use a quantitative method;24 semantic fluency test (temporal lobe function), and phonemic fluency test (frontal lobe function), both are brief tests used to assess cognitive deficit, we have normative parameters according to schooling.25 We also evaluated the number of intrusion and perseveration errors. All the tests used have been validated in older Mexican adults. Function was assessed on the Katz index of independence in activities of daily living (feeding, dressing, continence, toileting, bathing, transferring),26 and the Lawton instrumental activities of daily living scale (ability to handle finances, shopping, mode of transportation, laundry, food preparation, housekeeping, ability to use telephone, and responsibility for own medications).27 Sociodemographic variables such as sex, age, and education, were obtained from the comprehensive geriatric evaluation.
An independent neurologist viewed a simple brain magnetic resonance imaging (MRI) (1.5 T of the General Electric brand, model SIGN HDxt.151), with T1, T2 and FLAIR sequences and used standard neuroimaging terminology for small and large vessel disease to define imaging features (atrophy, leukoencephalopathy, lacunar infarcts, etc.).
The exclusion criteria of the study were: education ≤2 years, deficit in visual and auditory acuity that made it impossible to apply neuropsychological tests, heart, liver, kidney, cancer, or other relevant uncontrolled systemic diseases, as well as presence of severe neurological diseases (toxic, metabolic, infectious), significant depressive symptoms (score on the Yesavage Geriatric Depression Scale >5/15),28 and the presence of a major NCD according to the Clinical Scale of Dementia (CDR) (severe=3.29
5-word testDubois et al. developed 5WT to assess episodic verbal memory in a French population. It was proposed as a simple and rapid test for the detection of memory disorders of neurological origin. It is an immediate and delayed free memory recall test, based on presenting the patient with 5 words and, if necessary, is supported by the use of semantic keys. The same keys are used to control the learning of the 5 words and to provoke recovery, if the free memory is incomplete. It is applied in 2 stages:
1st stage. Immediate learning or recall, which takes place in 3 phases: introducing the written list: “Read this list of 5 words out loud and try to learn them, I’ll ask you later.”
Semantic category link: Which of these words is an animal, … a place, … a transport vehicle, … an article of clothing, … a part of the body?
Semantic category link: Which of these words is an animal, … a place, … a transport vehicle, … an article of clothing, … a part of the body?
Immediate reminder for learning control: 1. Turn the page and say: “Say the words you just read.” 2. For each word not spontaneously remembered, ask “What is the name of… (give the corresponding semantic key)? 3. If you did not remember all the words, show the list and point the finger at each of the missing ones and say “the name of (give semantic category) is… (read the word out loud). 4. Again turn the page and he wonders for each of the words not remembered before: “What was the name of… (give semantic key)?
During the next 5 minutes a non-verbal task is performed (clock drawing, for example), to later advance to the second stage.
2nd stage. Evocation or deferred memory: 2 phases (spontaneous and with semantic keys). The patient is asked: “Could you repeat the 5 words from the list you read a few minutes ago”? Subsequently, he is asked for each word not remembered: “what was the name of…” (give semantic key).
The number of words mentioned spontaneously is reported and recorded, plus those evoked with a semantic key at each stage. For example: Immediate recall, 3+1 (remembered 3 spontaneously and 1 with semantic code), and late recall, 4+1 (recalled 4 spontaneously and the rest with code); therefore the evaluation is reported as 5WT=3+1 and 4+1.30
From 5WT, 3 scores can be estimated: a Free Recall Score (FRS) by adding the Immediate Free Recall (IFR)+Free Deferred Recall (FDR), a Total Recall Score (TRS) by the sum IFR+Recall with Immediate Key (RIK)+FDR+Recall with Deferred Key (RDK) (both scores with a range of 0 to 10) and a Total Weighted Score (TWS) calculated by the following formula: [(IFR×2)+RIK]+[(FDR×2)+RDK] (range 0 to 20). The average time of 5WT application is 2minutes. The 5WT has sensitivity (91%) and specificity (87%) in identifying patients with AD.31
The cultural adaptation of this test was done with linguistic experts from the College of Mexico. Five nouns from the Spanish language (Mexico) with a similar meaning were selected in different regions of the country, with a length of 2 to 3 syllables and starting with different letters of the alphabet. The 5 words belong to different semantic categories (bus, transport; glove, garment; dove, animal; tooth, body part; market, place). The understanding of the chosen words was tested in small groups of volunteer older adults who attended the memory clinic of the study site. This test has been previously validated in Mexico.32
Statistics analysisA descriptive analysis of the sample was performed, registering frequencies, percentages, means±standard deviations (SD) according to the type of variable. For the comparative analysis of the categorical variables, the χ2 test and the Kruskal-Wallis test were used for the continuous variables. Concurrent validity was established by comparing 5WT with MMSE and Spearman's correlation coefficient estimate (rs).
Linear regression model was constructed to determine the discriminative capacity of 5WT of the 3 included groups considering the effect of the age, sex, and level of education of the participants. To establish the precision of the 5WT for the diagnosis of MixD, the area under the curve was estimated, as well as its sensitivity and specificity in each of the contrasting groups. A P-value <.05 was considered statistically significant. Analyzes were performed using SPSS version 20.0 for Windows® (SPSS Inc., USA). The protocol was approved by the institutional ethics committee (REF1158).
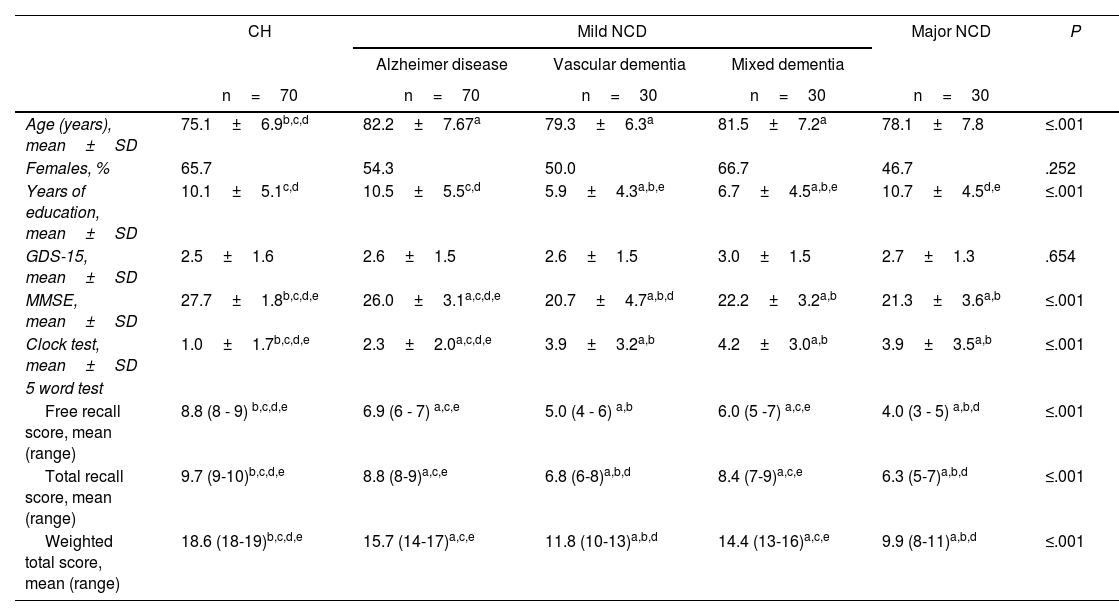
ResultsThe mean age of the participants was 79±7.7 years, 58% were women, and the mean education was 9±5.3 years. CH, 70; mild NCD (n=70) and major NCD (n=90): AD (n=30), VaD (n=30), and MixD (n=30). Table 1 shows the comparative analysis of sociodemographic characteristics and cognitive performance among the participants. Significant differences were found between the participants in the CH group in age, being younger (75±6.1 years) compared to the groups of mild NCD (82±7.6), and major NCD: AD, 79±6.3; VaD, 82±7.2, and MixD, 78±7.8 (P≤.001).
Sociodemographic and cognitive characteristics of the groups.
| CH | Mild NCD | Major NCD | P | |||
|---|---|---|---|---|---|---|
| Alzheimer disease | Vascular dementia | Mixed dementia | ||||
| n=70 | n=70 | n=30 | n=30 | n=30 | ||
| Age (years), mean±SD | 75.1±6.9b,c,d | 82.2±7.67a | 79.3±6.3a | 81.5±7.2a | 78.1±7.8 | ≤.001 |
| Females, % | 65.7 | 54.3 | 50.0 | 66.7 | 46.7 | .252 |
| Years of education, mean±SD | 10.1±5.1c,d | 10.5±5.5c,d | 5.9±4.3a,b,e | 6.7±4.5a,b,e | 10.7±4.5d,e | ≤.001 |
| GDS-15, mean±SD | 2.5±1.6 | 2.6±1.5 | 2.6±1.5 | 3.0±1.5 | 2.7±1.3 | .654 |
| MMSE, mean±SD | 27.7±1.8b,c,d,e | 26.0±3.1a,c,d,e | 20.7±4.7a,b,d | 22.2±3.2a,b | 21.3±3.6a,b | ≤.001 |
| Clock test, mean±SD | 1.0±1.7b,c,d,e | 2.3±2.0a,c,d,e | 3.9±3.2a,b | 4.2±3.0a,b | 3.9±3.5a,b | ≤.001 |
| 5 word test | ||||||
| Free recall score, mean (range) | 8.8 (8 - 9) b,c,d,e | 6.9 (6 - 7) a,c,e | 5.0 (4 - 6) a,b | 6.0 (5 -7) a,c,e | 4.0 (3 - 5) a,b,d | ≤.001 |
| Total recall score, mean (range) | 9.7 (9-10)b,c,d,e | 8.8 (8-9)a,c,e | 6.8 (6-8)a,b,d | 8.4 (7-9)a,c,e | 6.3 (5-7)a,b,d | ≤.001 |
| Weighted total score, mean (range) | 18.6 (18-19)b,c,d,e | 15.7 (14-17)a,c,e | 11.8 (10-13)a,b,d | 14.4 (13-16)a,c,e | 9.9 (8-11)a,b,d | ≤.001 |
CH: cognitively healthy; GDS: Geriatric Depression Scale; MMSE: Mini-Mental State Examination; NCD: neurocognitive disorders.
Different letters indicate differences between groups:
The average education for the CH group was 10.1±5.1 years; for mild NCD, 10.5±5.5, and in the major NCD group: AD, 5.9±4.3; VaD, 6.7±4.5, and MixD, 10.7±4.5 (P≤.001).
Participants with mild NCD and major NCD had worse cognitive performance (P≤.001) compared to the group of CH participants. The mean TWS in the CH group was 18.6 points (range, 18-19); in mild NCD, 15.7 (14-17), and in major NCD: AD, 11.8 (10-13); VaD, 14.4 (13-16), and MixD, 9.9 (8-11) (P≤.001).
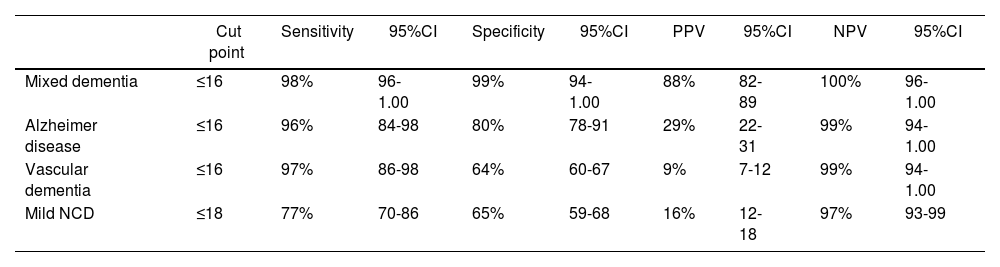
Construct validity when comparing 5WT and MMSE using the Spearman correlation test was ρ=.830 (P<.001) and d Sommer=.41 (P<.001). The area under the curve (AUC) for 5WT in the TWS for the diagnosis of MixD was 0.985 with 98% sensitivity (95%CI, 0.96-1.00) and 99% specificity (95%CI, 0.94-1.00), 88% PPV (95%CI, 0.82-0.89), 100% NPV (95%CI, 0.96-1.00), and a cut-off point ≤16/20 (P<.001). The AD AUC was .920 with 96% sensitivity (95%CI, 0.84-0.99) and 80% specificity (95%CI, 0.78-0.91), 29% PPV (95%CI, 0.22-0.31), 99% NPV (95%CI, 0.94-1.00), and a cut-off point ≤16/20 (P<.001). In VaD, the AUC was .834 with 97% sensitivity (95%CI, 0.86-0.98) and 64% specificity (95%CI, 0.62-0.67), 9% PPV (95%CI, 0.7-0.12), 99% NPV (95%CI, 0.94-1.00), and a cut-off point ≤16/20 (P<.001). Finally, in the mild NCD, the AUC was .784 with 77% sensitivity (95%CI, 0.70-0.86) and 65% specificity (95%CI, 0.59-0.68), 16% PPV (95%CI, 0.12-0.18), 97% NPV (95%CI, 0.93-0.99), and a cut-off point ≤18/20 points (P<.001) (table 2).
Optimum cut points, sensitivity, and specificity.
| Cut point | Sensitivity | 95%CI | Specificity | 95%CI | PPV | 95%CI | NPV | 95%CI | |
|---|---|---|---|---|---|---|---|---|---|
| Mixed dementia | ≤16 | 98% | 96-1.00 | 99% | 94-1.00 | 88% | 82-89 | 100% | 96-1.00 |
| Alzheimer disease | ≤16 | 96% | 84-98 | 80% | 78-91 | 29% | 22-31 | 99% | 94-1.00 |
| Vascular dementia | ≤16 | 97% | 86-98 | 64% | 60-67 | 9% | 7-12 | 99% | 94-1.00 |
| Mild NCD | ≤18 | 77% | 70-86 | 65% | 59-68 | 16% | 12-18 | 97% | 93-99 |
95%CI: 95% confidence interval; NCD: neurocognitive disorder; NPV: negative predictive value; PPV: positive predictive value.
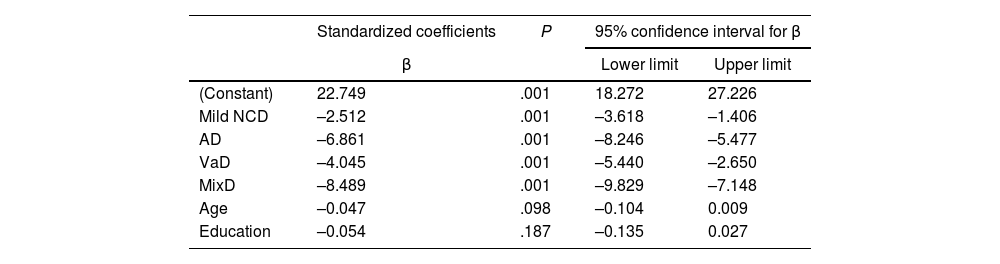
In Table 3, the linear regression model showed that after adjusting for age and education, the TWS inversely discriminates between mild NCD and major NCD predominantly in MixD: mild NCD, β=2.51; AD, β=6.86; VaD, β=4.04; MixD, β=8.48 (P<.001).
Linear regression model adjusted for age and education, between the weighted total score and different groups of NCD.
| Standardized coefficients | P | 95% confidence interval for β | ||
|---|---|---|---|---|
| β | Lower limit | Upper limit | ||
| (Constant) | 22.749 | .001 | 18.272 | 27.226 |
| Mild NCD | –2.512 | .001 | –3.618 | –1.406 |
| AD | –6.861 | .001 | –8.246 | –5.477 |
| VaD | –4.045 | .001 | –5.440 | –2.650 |
| MixD | –8.489 | .001 | –9.829 | –7.148 |
| Age | –0.047 | .098 | –0.104 | 0.009 |
| Education | –0.054 | .187 | –0.135 | 0.027 |
The dependent variable is the total weighted score.
The results of our study demonstrate that the 5WT is a valid and reliable instrument with ideal psychometric properties for MixD screening in older adults. With the cut-off point ≤16, the TWS has a sensitivity of 98%, a specificity of 99%, a PPV of 88% and a PNV of 100%. Furthermore, in our study, 5WT was useful in diagnosing AD-type major NCD, with a cut-off point ≤16 of TWS, with a sensitivity of 98% and specificity of 80%, similar to that reported by Dubois et al. (sensitivity 91% and specificity 87%), Rozzini et al. (97% sensitivity and 94% specificity) and Mormont et al. (reporting 90% sensitivity and 96% specificity).17,33,34 Mormont et al. also studied the precision of the 5WT for the detection of patients with Mild NCD, and reported a sensitivity of 75% and a specificity of 96%, similar to what was observed in our study (77% sensitivity and 65% specificity).32
In the 5WT, the TWS less than or equal to the cut-off point is a good index of alteration in the mechanisms of immediate and delayed spontaneous memory, and without the benefit of semantic clues. In MixD, alterations are identified in each of the phases of episodic memory: learning, storage and recovery, compared to AD, where there is classically a deterioration in “hippocampal” memory, characterized by an alteration in the storage mechanism of the memory. Information and unlike VaD, in which only recovery problems arise, with the benefit of semantic clues.17 Therefore, poor performance in 5WT could represent a functional disconnection of the hippocampus specifically from the neocortical regions.32
In our study, 5WT identifies specific memory mechanisms that are compromised in people with MixD and that other studies have failed to detect. There are few studies that, with different neuropsychological tests, try to define the cognitive profile of MixD, but were unable to find specific difficulties in memory functions. Schmidtke et al. studied in 2002 the neuropsychological profile in AD, VaD and MixD, through the application of 5 tests: memory recall and verbal recognition, naming of objects, semantic fluency and clock reading. The MixD and AD groups were identical with respect to the profile of cognitive scores, except for worse performance in both types of verbal fluency (phonological and semantic) in the MixD group. Another study comparing patients with MixD and VaD reported similar results; worse performance was found on the tests of clock reading and verbal fluency in the MixD group.35
Other studies that have used 5WT report that the difference between MixD is focused on the type of errors (intrusions and perseverations). Moreno et al., in 2015, observed a greater presence of intrusion and perseveration errors when using the 5WT, considering that intrusive errors are associated with semantic performance and memory, making it useful as a complementary test to explore the function of the temporal lobes, since perseverative errors are associated with impaired self-monitoring, working memory, and executive skills, making it useful for exploring frontosubcortical association circuits. Furthermore, this study showed that perseverative errors were more frequent in MixD.13 Another study concluded that the neuropsychological profile of patients with mild to moderate stage MixD is characterized by poorer overall performance, as well as impaired attention and visual construction compared to patients with mild to moderate severity AD.36
One of the strengths of our study is that the 5WT allows us to analyze memory processes in detail (learning, storage, and recovery), which could help to better characterize the major NCD with mixed characteristics in future studies. Furthermore, it confirms that the 5WT is a screening test, easy and quick to apply, and has great utility in daily clinical practice.
Our study has several limitations: the sample size comes from a tertiary level hospital, with a mean schooling of 9 years, and does not reflect the education level of the Mexican population, which compromises its external validity. Second, there may be spectrum bias due to the fact that we do not include patients with different severity conditions of the major NCD mixed type dementia. While the review bias could overestimate the diagnostic capabilities of the test. Finally, it was not possible to assess interobserver and intraobserver reliability, which is also a limitation. More studies are required with a larger number of patients to evaluate the usefulness of 5WT in major NCD in the suspicion of mixed etiology; to know its usefulness at different levels of care and / or in the community, with different ages and schooling.
MixD (coexistence of AD and VaD) is a subtype of major NCD common in the older adult, so it is necessary to carry out more research around the concept of MixD to establish possible clinical criteria that allow its timely diagnosis.
ConclusionsThe 5WT is a valid and reliable screening test for the detection of major NCD especially in MixD, AD, VaD and mild NCD, in a sample of older adults. The 5WT is a quick test for the evaluation of episodic verbal memory, easy to use and with optimal psychometric properties for the exploration of cognitive characteristics in MixD.
FundingThis article did not receive help or assistance from any funding agency.

