






Serial position effects are observed when a person memorises a series of words exceeding his or her attention span. Cognitively normal individuals recall words at the beginning and end of the list more frequently than those in the middle, which reflects the way that short- and long-term episodic memory works.
ObjectiveTo study the serial position effect in patients with mild cognitive impairment (MCI) compared to subjects with Alzheimer-type dementia (AD) or normal ageing (NA).
Methods30 AD, 25 MCI and 20 NA subjects underwent neurological and neuropsychological assessment. The Rey Auditory Verbal Learning Test (RAVLT) was used to study primacy, middle, and recency effects and delayed recall for each group.
ResultsThe general memory pattern of MCI subjects was very similar to that of AD subjects, and was characterised by reduced learning capacity, rapid forgetfulness and clear recency effect in learning. With regard to delayed recall, however, there were differences in performance; MCI subjects’ ability to recall words at the beginning and middle of the list was similar to that of normal subjects, while their memory of words at the end of the list was poor, as in AD subjects.
ConclusionsRAVLT is a tool permitting us to distinguish between MCI and NA subjects. The recency index for the delayed recall task is a valid indicator for distinguishing between MCI patients and patients with normal ageing.
Los efectos de posición serial son estudiados cuando se memoriza una serie de palabras que excede el span atencional. En sujetos normales son recordadas más frecuentemente las palabras del inicio y final de una lista reflejando el funcionamiento de la memoria episódica a corto y largo plazo.
ObjetivosEstudiar el efecto de principio y el de fin de lista en pacientes con deterioro cognitivo leve (DCL) y compararlo con demencia tipo Alzheimer (DTA) y sujetos con envejecimiento normal (SN).
MétodosFueron evaluados neurológica y neuropsicológicamente 30 pacientes con DTA, 25 con DCL y 20 SN. Se utilizó el Test de aprendizaje auditivo de una lista de palabras de Rey en donde se evaluó el efecto de principio, medio y fin de lista en cada ensayo y su efecto en el recuerdo diferido.
ResultadosLos sujetos con DCL mostraron un patrón general de memoria similar a los sujetos con DTA, caracterizado por una reducción en el aprendizaje, olvido acelerado y un claro efecto de fin de lista en el aprendizaje. A nivel del recuerdo diferido mostraron un patrón diferencial recordando palabras de principio y medio más cercano a los normales pero no recordando las finales de la lista como las DTA.
ConclusionesLa prueba de aprendizaje de una lista de palabras es una herramienta que nos permite discriminar entre pacientes con DCL y SN. El índice de recencia en el recuerdo diferido es un indicador útil para diferenciar el envejecimiento normal de los pacientes con DCL.
The serial position effect is observed when a subject studies a list of items, such as words, exceeding his or her attention span. Cognitively normal subjects recall words at the beginning and at the end of a list more frequently rather than words in the middle. This enhanced recall of words at the beginning of a list is called the primacy effect; better recall of final words is the recency effect. We interpreted these findings using the Atkinson–Shiffrin memory model1 which states that the primacy and recency effects reflect the activity of 2 independent memory systems: long-term memory (LTM) and short-term memory (STM).
Studies have described a stronger recency effect in contrast with a weaker primacy effect in various groups with cognitive impairment. This phenomenon has been reported in different types of amnesia2 as well as in dementia of the Alzheimer's type (DAT).3
Data in cases of mild cognitive impairment (MCI) are more limited and controversial. Bennett et al.4 found similar results in MCI and control groups. Shankle et al.5,6 and Howieson et al.7 reported similar results in MCI and patients with Alzheimer disease (AD) which could be helpful for describing this population.
The purpose of this study is to evaluate serial position effects (beginning, middle, and end of list) in a word-learning task and to examine the involvement of those effects in delayed recall in patients with mild cognitive impairment compared to patients with DAT or to normal control subjects.
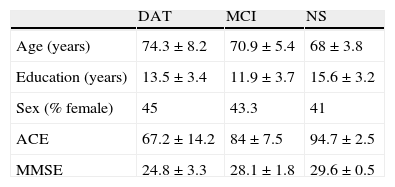
MethodSubjectsNeurological, neuropsychological, and complementary laboratory and neuroimaging tests were performed on a group of 25 patients with amnestic MCI (according to criteria set out by Petersen et al.8); 30 patients with mild DAT (probable diagnosis according to the NINCDS-ADRDA criteria, McKhann et al.9); and 20 normal subjects (NS) from the community. Patients were recruited from cases seen in the department in consecutive order. Table 1 lists demographic data for the different groups of subjects under study.
Demographic data.
| DAT | MCI | NS | |
| Age (years) | 74.3±8.2 | 70.9±5.4 | 68±3.8 |
| Education (years) | 13.5±3.4 | 11.9±3.7 | 15.6±3.2 |
| Sex (% female) | 45 | 43.3 | 41 |
| ACE | 67.2±14.2 | 84±7.5 | 94.7±2.5 |
| MMSE | 24.8±3.3 | 28.1±1.8 | 29.6±0.5 |
All values (except for sex) are expressed as mean±standard deviation.
ACE: Addenbrooke's Cognitive Examination; MMSE: Mini Mental State Exam.
The neuropsychological assessment included the following tests: MMSE (Mini Mental State Exam),10 ACE (Addenbrooke Cognitive Examination),11 BNT (Boston Naming Test),12 Token Test,13 FAB (Frontal Assessment Battery),14,15 Trail Making Test parts A and B,16 Wisconsin card sorting test,17 Rey–Osterrieth complex figure test,18 and the Logical Memory test.19
Serial position studySerial position effects were studied using the Rey Auditory Verbal Learning Test,20 which assesses verbal learning, delayed recall, and recognition. This list includes 15 words that the subject repeats in 5 learning trials. Following those 5 trials, the subject is asked to learn an interference list; immediately after that, he or she must recite the words on the first list. Recall of the words on the first list is also tested 30minutes later.
We examined serial position effects (primacy, middle, and recency). The primacy effect refers to a subject's ability to recall the first words of a list more easily than others, while increased ability to recall the final words of a list is known as the recency effect.21 For purposes of analysing the effects mentioned above, we will also refer to an increased probability of recalling words in the middle of the list as the ‘middle effect’. In this study we considered a primacy effect of 100% for the first 4 words repeated during each of the 5 trials (maximum of 20 words), based on the studies by Drake et al.21 and La Rue et al.22 We also considered a recency effect of 100% for the last 4 words (maximum of 20 words). A ‘middle effect’ of 100% was considered to be recall of the 7 words in the middle of the list (maximum of 35 words). Rather than using only the first learning trial to analyse serial position effect, we used results from all 5 trials and completed the statistical analysis using data obtained as a percentage of the total.
The primacy, middle, and recency effects for the learning and the delayed recall trials were calculated for all 5 trials and per trial. Values were then compared between groups in order to detect any significant differences during the learning phase and measure the potential influence of that phase on delayed recall.
Statistical methodsTwo statistical analyses were completed. In the first analysis, we observed the behaviour of the NS, MCI, and DAT groups by calculating each of the 3 effects (primacy, middle, and recency) for the sum of the 5 trials in the learning phase. Effects were calculated for each group, and performances were compared between different groups.
The Shapiro–Wilk test was used to check for a normal distribution. Where distribution was found to be normal, two-factor analysis of variance (by trial and by group) was applied for repeated measures testing (after angular transformation of data). When a normal data distribution could not be obtained even after transformation, non-parametric Kruskal–Wallis and Friedman methods were used. After rejecting a hypothesis involving more than 2 groups, we evaluated a posteriori pairwise comparisons (Tukey after ANOVA; Conover after non-parametric ANOVA).
A second analysis was performed by examining each trial in the learning phase individually to determine the following: (a) if significant differences in primacy, middle, and recency effects for each of the trials were present between the groups; (b) the behaviour of each effect in each group as trials progressed, and (c) if there were significant differences for each group and each effect between trials 6 and 7.
To analyse differences in mean scores (given as percentages of the total) among the 3 groups, the different trials, and the type of serial position effect (primacy, middle, and recency), we used a general repeated-measures linear model (3-way analysis of variance with repeated measures on 2 factors). In all cases, after analysing the global model, we examined the simple effects for each of the factors (group, trial, and list) for every combination of the other 2 factors. The corresponding mean square of the global variance analysis was used as the estimator of variance. In cases in which there were differences among factors on more than 2 levels, Bautista's method (BSS) was used as an a posteriori test of multiple comparisons. This method, based on forming conglomerates, ensures that homogeneous disjoint sets will be produced.
We used InfoStat (Version 2008, Universidad Nacional de Córdoba, Spain) and SPSS 12.0 (Chicago, USA). In all cases, a probability of type I error of less than 0.05 was considered statistically significant.
ResultsIn the initial analysis of the characteristics of the learning curve in NS, MCI, and DAT patients, subjects with MCI showed a similar profile to that of DAT patients (Fig. 1). In the NS group, all increases in the learning phase were significant, except between trials 4 and 5. In the MCI and DAT groups, only the increase between trials 1 and 2 was significant. For trial 1, we did not observe any significant differences between mean scores in the MCI and SN groups or between the MCI and DAT groups. Beginning in trial 2, MCI group results are significantly worse than NS results and better than those from the DAT group (P<.05). This difference in results increases (P<.01) beginning in trial 3 (Fig. 1).

In the evaluation of serial position effect on the trials, using the sum of the scores from all 5 trials to show the learning curve (Fig. 2), the primacy and middle indexes were significantly different among the 3 groups. This was true for both the learning tasks (P<.01) and the delayed recall trials (P<.01). The recency index differed significantly between the NS group and the patient groups (DAT and MCI), but there were no differences between the MCI and DAT groups.

In the delayed recall trial (Fig. 3), subjects in all groups remembered more words from the beginning and middle of the list than from the end. Only those in the NS group recalled words from all 3 sections of the list; MCI patients only recalled words at the beginning and middle of the list, and not at the end. Primacy and middle indexes were significantly different between the 3 groups (P<.01). The recency index differed significantly between the NS group and the patient groups (MCI or DAT) (P<.05), but there were no differences between the MCI and DAT groups.

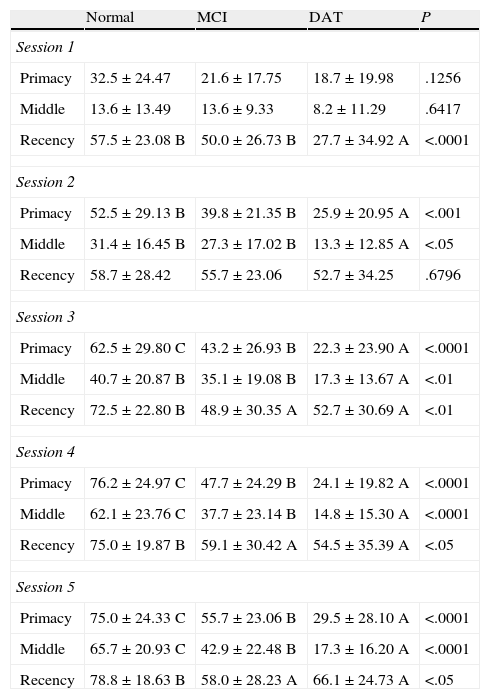
The serial position effect was subsequently analysed for all 5 verbal learning trials (see Table 2).
Comparison of serial position effects over 5 verbal learning trials.
| Normal | MCI | DAT | P | |
| Session 1 | ||||
| Primacy | 32.5±24.47 | 21.6±17.75 | 18.7±19.98 | .1256 |
| Middle | 13.6±13.49 | 13.6±9.33 | 8.2±11.29 | .6417 |
| Recency | 57.5±23.08 B | 50.0±26.73 B | 27.7±34.92 A | <.0001 |
| Session 2 | ||||
| Primacy | 52.5±29.13 B | 39.8±21.35 B | 25.9±20.95 A | <.001 |
| Middle | 31.4±16.45 B | 27.3±17.02 B | 13.3±12.85 A | <.05 |
| Recency | 58.7±28.42 | 55.7±23.06 | 52.7±34.25 | .6796 |
| Session 3 | ||||
| Primacy | 62.5±29.80 C | 43.2±26.93 B | 22.3±23.90 A | <.0001 |
| Middle | 40.7±20.87 B | 35.1±19.08 B | 17.3±13.67 A | <.01 |
| Recency | 72.5±22.80 B | 48.9±30.35 A | 52.7±30.69 A | <.01 |
| Session 4 | ||||
| Primacy | 76.2±24.97 C | 47.7±24.29 B | 24.1±19.82 A | <.0001 |
| Middle | 62.1±23.76 C | 37.7±23.14 B | 14.8±15.30 A | <.0001 |
| Recency | 75.0±19.87 B | 59.1±30.42 A | 54.5±35.39 A | <.05 |
| Session 5 | ||||
| Primacy | 75.0±24.33 C | 55.7±23.06 B | 29.5±28.10 A | <.0001 |
| Middle | 65.7±20.93 C | 42.9±22.48 B | 17.3±16.20 A | <.0001 |
| Recency | 78.8±18.63 B | 58.0±28.23 A | 66.1±24.73 A | <.05 |
All values are expressed as mean±standard deviation. Identical letters on the same horizontal line indicate homogeneous groups.
While trials 1 and 2 do not allow us to draw clinically relevant conclusions, changes may be observed in the MCI group with respect to the NS group in trial 3. The MCI group results start to resemble those of DAT patients, and there are significant differences in the primacy effect in all 3 groups; between the NS and MCI groups vs DAT for the middle effect; and between the NS group vs MCI and DAT for the recency effect. In trials 4 and 5, significant differences in the primacy and middle effects can be observed among all 3 groups. Differences in the recency effect are significant between the NS and the MCI/DAT groups.
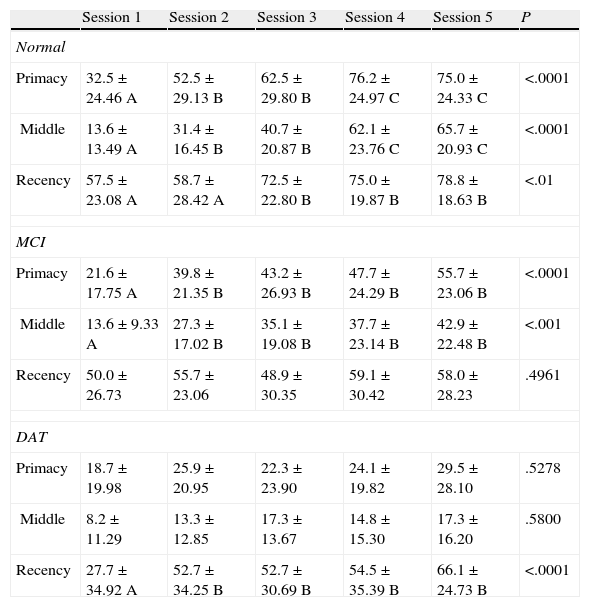
Analysis of learning patterns for each of the 3 groups and for different serial position effects (see Table 3) revealed a progressive learning pattern in the NS group with significant differences apparent in the primacy and middle effects for each successive trial. No significant differences in the recency effect were observed as of trial 3; instead, there is a ceiling effect with no learning progression.
Study of changes in serial position effect over the series of trials in all 3 populations.
| Session 1 | Session 2 | Session 3 | Session 4 | Session 5 | P | |
| Normal | ||||||
| Primacy | 32.5±24.46 A | 52.5±29.13 B | 62.5±29.80 B | 76.2±24.97 C | 75.0±24.33 C | <.0001 |
| Middle | 13.6±13.49 A | 31.4±16.45 B | 40.7±20.87 B | 62.1±23.76 C | 65.7±20.93 C | <.0001 |
| Recency | 57.5±23.08 A | 58.7±28.42 A | 72.5±22.80 B | 75.0±19.87 B | 78.8±18.63 B | <.01 |
| MCI | ||||||
| Primacy | 21.6±17.75 A | 39.8±21.35 B | 43.2±26.93 B | 47.7±24.29 B | 55.7±23.06 B | <.0001 |
| Middle | 13.6±9.33 A | 27.3±17.02 B | 35.1±19.08 B | 37.7±23.14 B | 42.9±22.48 B | <.001 |
| Recency | 50.0±26.73 | 55.7±23.06 | 48.9±30.35 | 59.1±30.42 | 58.0±28.23 | .4961 |
| DAT | ||||||
| Primacy | 18.7±19.98 | 25.9±20.95 | 22.3±23.90 | 24.1±19.82 | 29.5±28.10 | .5278 |
| Middle | 8.2±11.29 | 13.3±12.85 | 17.3±13.67 | 14.8±15.30 | 17.3±16.20 | .5800 |
| Recency | 27.7±34.92 A | 52.7±34.25 B | 52.7±30.69 B | 54.5±35.39 B | 66.1±24.73 B | <.0001 |
All values are expressed as mean±standard deviation. Identical letters on the same horizontal line indicate homogeneous groups.
In patients with MCI, significant differences in the primacy and middle effects were only observed between trial 1 and all other trials; these subjects learned more words in later trials than in trial 1. No significant differences in the recency effect were observed between any 2 different trials. Patients with DAT did not show significant differences among any of the trials with regard to the primacy and middle effects, which may indicate lack of learning. For the recency effect, significant differences are present between trial 1 and the rest of the trials; subjects were able to recall more words in later trials than in trial 1.
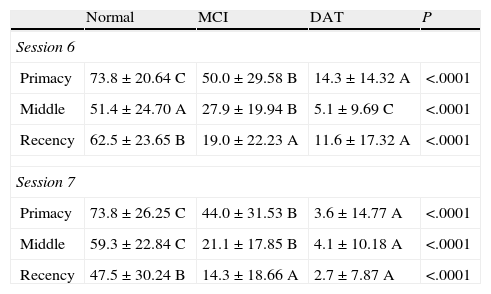
In order to observe in which phase patients with MCI forget words, we compared trials 6 and 7 (Table 4). Results from this comparison showed significant differences in primacy and middle effects among the 3 groups for both trials 6 and 7. Regarding the recency effect, however, differences were only significant between normal subjects and patients.
Study of changes in serial position effect over trials 6 and 7 in all 3 populations.
| Normal | MCI | DAT | P | |
| Session 6 | ||||
| Primacy | 73.8±20.64 C | 50.0±29.58 B | 14.3±14.32 A | <.0001 |
| Middle | 51.4±24.70 A | 27.9±19.94 B | 5.1±9.69 C | <.0001 |
| Recency | 62.5±23.65 B | 19.0±22.23 A | 11.6±17.32 A | <.0001 |
| Session 7 | ||||
| Primacy | 73.8±26.25 C | 44.0±31.53 B | 3.6±14.77 A | <.0001 |
| Middle | 59.3±22.84 C | 21.1±17.85 B | 4.1±10.18 A | <.0001 |
| Recency | 47.5±30.24 B | 14.3±18.66 A | 2.7±7.87 A | <.0001 |
Data given as mean±standard deviation. Identical letters on the same horizontal line indicate homogeneous groups.
Early diagnosis of DAT, especially during the prodromal or MCI stage, is known to be vitally important because drugs intended to slow the course of the disease are now available. MCI, especially amnestic MCI, will progress to Alzheimer disease with a conversion rate of approximately 12% yearly.23
Recent studies using new neuroimaging and CSF biomarker techniques have been shown to improve the specificity of the diagnosis of MCI due to AD. However, use of these techniques is only indicated after doctors have defined the type of memory disorder that may progress to AD. On this topic, numerous studies have shown that deficits in delayed recall24 and lack of benefit from clues in clued recall and recognition tasks25 are the most important characteristics of memory loss in MCI that indicate progression to AD.
Determining whether amnestic disorders in patients with either MCI or DAT are qualitatively or quantitatively different is a crucial step. Doctors also need access to a reliable, valid, and specific tool allowing them to differentiate between NS and MCI.
This study evaluated the serial position effect on the learning curve and on delayed recall in MCI, DAT, and normal subject groups. Results from verbal learning trials in MCI subjects can be plotted as a plane curve resembling the curve shown by the DAT group. It differs from the steep curve seen in results from control subjects. Results from these 3 trials were similar between patients with MCI and those with DAT. When comparing serial position effects across all 5 trials, both patients with MCI and those with DAT were able to recall the last words on the list only by using short-term memory. The words did not pass into long-term memory after additional trials. These results differed from those in the control group in which subjects were able to increase their recall of words at the end of the list by storing them in long-term memory as a result of repeated learning trials.
The recency index from the delayed recall trial shows clear differences between the NS and MCI groups. Individuals in the NS group recalled words from all 3 sections of the list; patients with MCI remembered words from the beginning and middle sections, but not the end. One explanation for this phenomenon could be that normal subjects were able to use long-term memory to retain words from all 3 sections of the list after the 5 learning trials. In contrast, MCI patients, like DAT patients, were unable to retain words from the end of the list; these words could only be recalled using short-term memory and not long-term memory. Patients with DAT did not recall words from all 3 sections.
While normal subjects were able to recall words from each of the 3 sections of the list in the delayed recall trial, those in the MCI group recalled words from the beginning and middle of the list only. Patients with DAT displayed homogeneous lack of recall for all sections.
The profiles of patients with DAT vs MCI are relatively similar during the learning phase. It is possible to distinguish between them, however, if we closely observe how subjects performed on delayed recall trials with regard to the serial position effect for the words they remembered. In initial stages of DAT, neuropathological changes affect the medial temporal region containing the hippocampal formation, parahippocampal gyrus, and entorhinal cortex.26 These areas are critical for episodic memory. Episodic memory loss is therefore a reliable and early clinical marker of DTA, and this has been demonstrated by earlier studies.25 Tierney et al.27 found that delayed recall on the RAVLT can be both helpful and very accurate for predicting probable AD in subjects with memory disorders but no dementia. Furthermore, Estevez-Gonzalez et al.24 reported that the total number of words learned throughout the 5 study trials, a score of 0 on the delayed recall trials (at 6min and at 20min) and a percentage of forgetfulness of 75% are the parameters that allow us to differentiate among normal controls, patients with MCI, and patients with DTA.
Our findings support and complement earlier studies5–7 on the usefulness of examining primacy, middle, and recency effects on the RAVLT in order to discriminate among normal subjects, MCI patients, and AD patients, based on a verbal learning task.
The MCI group's results were poorer than those from the control group for both acquisition and delayed recall of the RAVLT word list, and these subjects showed a substantially reduced ability to acquire information. As predicted, results from the MCI group attested to decreased primacy, middle, and recency effects with respect to normal subjects, while the MCI group did perform better than patients with AD. It is believed that words at the beginning of a list are stored in long-term memory. If the word order remains the same in each of the learning trials, the possibility of a good score increases due to the number of words that have been learned, and the primacy effect should be stronger.
As in patients with DAT, subjects with MCI display a primacy effect that decreases as they study the words on a list. The reduced primacy effect in MCI subjects compared to normal controls is probably caused by a decrease in the individual's ability to add new elements to long-term memory. This is a typical trait in AD. Results observed for the recency effect are important compared to other effects. The general learning curve for patients with MCI was less steep than in normal subjects, but they did perform better than patients with DAT. We also observed that while patients with MCI were able to recall words from the beginning and middle of the list on the delayed recall trial, they could not remember final words.
In summary, the most important results that distinguish between patients with MCI and normal subjects are the decreased primacy effect and the lack of delayed recall of words at the end of the list. MCI may be diagnosed more precisely by using neuropsychological tests that contemplate multiple cognitive markers; results for serial position effect in a learning test such as RAVLT may improve diagnostic accuracy.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Martín ME, et al. Relevancia del efecto de posición serial en el diagnóstico diferencial entre el deterioro cognitivo leve, la demencia de tipo Alzheimer y el envejecimiento normal. Neurología. 2013;28:219–25.
