



The incidence of neurological and psychiatric diseases and disorders has increased in recent years, and similarly, the number of technological tools facilitating neuropsychological rehabilitation for family members and therapists has also grown. The purpose of this article is to describe some of these tools and indicate the needs they cover.
DevelopmentThis article reviews some currently well-known neuropsychological rehabilitation platforms, compares them, and proposes future lines of work to be considered when developing tools that meet real needs. In this review, we list the main advantages and shortcomings of each of the tools and establish benchmarks for evaluating them. In comparing these platforms, we may observe their advantages on the one hand, and areas needing improvement on the other.
ConclusionsThis review demonstrates that more of these tools are entering the market, but many aspects of neurorehabilitation remain uncovered. Additional studies evaluating these tools’ effectiveness are also needed.
En los últimos años se ha incrementado la incidencia de las enfermedades y trastornos neurológicos y psiquiátricos y con ello la aparición de herramientas tecnológicas que facilitan a los terapeutas y familiares la rehabilitación neuropsicológica. De aquí que sea necesario establecer cuáles son algunas de estas herramientas y qué necesidades cubren.
DesarrolloEl presente artículo revisa algunas de las plataformas de rehabilitación neuropsicológica más conocidas hoy día, comparándolas y proponiendo líneas futuras de trabajo para tener en cuenta en la construcción de herramientas que se adapten a necesidades reales. En esta revisión se han visto las principales ventajas y carencias de cada una de las herramientas y se han establecido unos criterios comparativos para evaluar las mismas. En la comparación de estas plataformas, podemos observar, por una parte, las ventajas que nos ofrece su uso, pero también las carencias que aún tienen.
ConclusionesSe demuestra el crecimiento de estas herramientas en el mercado, pero aún quedan muchos aspectos que cubrir de la neurorrehabilitación y estudios que muestren la eficacia del uso de las mismas.
The technological advances of the past few years have contributed to the increase in new tools intended to facilitate neuropsychological rehabilitation in many types of patients. Cognitive deficit may arise from such diverse causes as head trauma, cerebrovascular disease, or disorders secondary to neurological diseases (Parkinson's disease, multiple sclerosis, Alzheimer disease, etc.). Creating a list of rehabilitation tools and the needs they cover is therefore necessary.
Neuropsychological rehabilitation developed from early models in which management was centred on cognitive, behavioural and emotional alterations caused by brain damage. Basic strategies for neuropsychological rehabilitation were first described by Butfield and Zangwill1,2 in the twentieth century. Some of the principles of neuropsychological rehabilitation are as follows:
- –
Restitution or restoration: based on stimulation and repeated practice of exercises and tasks, the aim is to restore the mechanisms affected by the lesion and optimise performance.
- –
Compensation: refers to the use or support of other preserved cognitive functions to complete the task that had mainly been done by the altered function. The aim is for patients to learn or re-learn how to perform functional activities which are important in daily life.
- –
Substitution: refers to using supporting devices or external mechanisms in order to effectively perform the task.
The current and growing trend is to use a comprehensive rehabilitation strategy in which different cognitive functions will work simultaneously; attention, executive functions, and memory are rehabilitated as a whole as processes used in activities of daily living.3 Focusing on one isolated process without mentioning the others is not easy; processes are interdependent at both the neuroanatomical and functional levels since these functions share several structures and neural circuits. The intervention used will depend on the aetiology of the patient's neurological lesion, the stage of recovery, the general cognitive status, and responses to interventions.
If doctors are to design this type of tools and tasks correctly, they must know how the brain captures information and combines it to elicit cognition, movement, perception, and emotion. Doctors must also be familiar with computerised resources focusing on specific aims that will help patients overcome environmental barriers, and they should understand the reasons for cognitive rehabilitation's profound impact on cognitive performance: plasticity, neurogenesis, and neural models of learning and memory.4,5
Requirements for a cognitive rehabilitation toolA technological tool should fulfil a series of requirements to improve patients’ performance and increase the efficacy of rehabilitation. The materials used should be related to actual activities of daily living and therefore demonstrate ecological validity. This way, therapy results can be extrapolated to other situations which the patient might have to face. Likewise, the material should motivate the patient and be meaningful (familiar pictures and music). It is essential that these materials not resemble laboratory equipment, which is typically complex and not comparable to that found in other contexts. Materials must be adapted to the type of user and level of development (children, adults, and elderly patients), and to the user's cognitive capacities. Any potential motor disabilities or attention deficits should also be considered. These tasks should be presented in an order that will also be followed by the training tools when introducing this working method into other areas of the patient's routine.
These activities should be designed based on evidence and scientific models, without overlooking such parameters as efficacy and validity, and including clinical trial and double-blind single patient studies.6,7 Therefore, knowing how the brain works and aiming tasks at specific cognitive domains is of vital importance.
Basic considerations in a neuropsychological rehabilitation toolCognitive training should be hierarchical and train one or more cognitive capacities,8 since we need more than one cognitive domain to perform any single task. The duration of each session should be customisable and number of sessions should be automatically selected for each patient. Furthermore, therapy should include a series of stages and phases to be mastered (levels) so that the patient can learn and improve. Training is a specifically oriented process and should be always validated by a doctor, although sessions can be directed by therapists and caregivers.
The process should include a variety of stakeholders (patients, caregivers, clinicians) and be adaptable to sensorimotor disabilities and as many neurological and neuropsychiatric diseases and disorders as possible. Scientific studies and models should be based not only on evidence but also on the principles of effectiveness, validity, and consistency,9–11 as well as being extrapolatable and flexible. Models should be adaptable to all types of patients and integrate the maximum number of neuropsychological rehabilitation processes (daily cognitive rehabilitation, psychoeducation, and social skills).
MethodsWe have reviewed the most popular platforms and tools for neuropsychological rehabilitation on the market and searched for information on these products on Internet sites and in published documents and studies. This review lists the main functions and shortcomings of each product and establishes comparison criteria to assess them. We will now describe each of the measurement criteria examined and the scores assigned for each measurement.
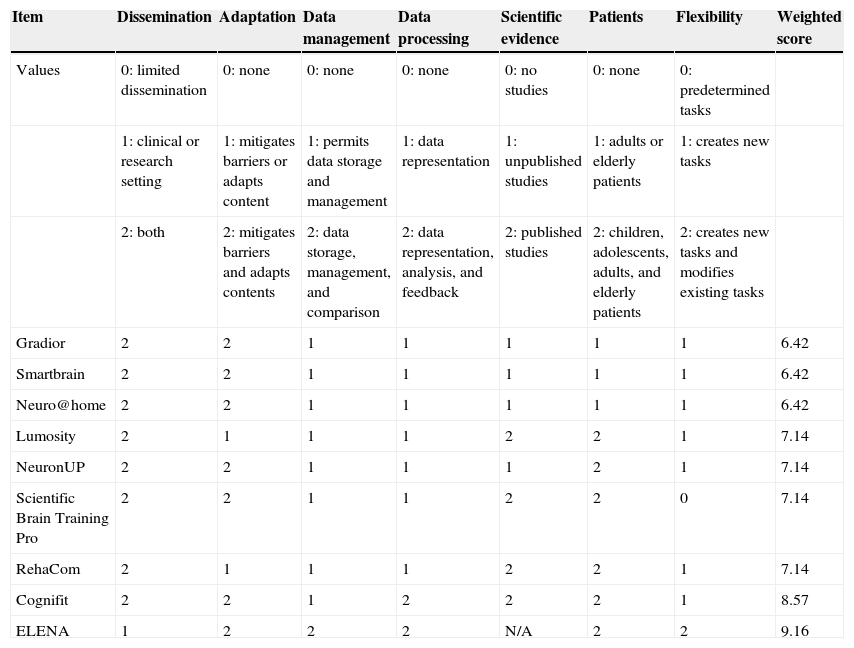
DisseminationThis criterion refers to the platform's market consolidation. Platforms were classified as well-known in clinical settings, that is, used by multiple hospitals as rehabilitation aids, and in research settings when tools have been examined in studies that test their efficacy and validity based on scientific evidence and models. Values listed in Table 1 correspond to limited dissemination (0), clinical or research (1), and clinical and research (2).
Comparison of neuropsychological rehabilitation platforms.
| Item | Dissemination | Adaptation | Data management | Data processing | Scientific evidence | Patients | Flexibility | Weighted score |
|---|---|---|---|---|---|---|---|---|
| Values | 0: limited dissemination | 0: none | 0: none | 0: none | 0: no studies | 0: none | 0: predetermined tasks | |
| 1: clinical or research setting | 1: mitigates barriers or adapts content | 1: permits data storage and management | 1: data representation | 1: unpublished studies | 1: adults or elderly patients | 1: creates new tasks | ||
| 2: both | 2: mitigates barriers and adapts contents | 2: data storage, management, and comparison | 2: data representation, analysis, and feedback | 2: published studies | 2: children, adolescents, adults, and elderly patients | 2: creates new tasks and modifies existing tasks | ||
| Gradior | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 6.42 |
| Smartbrain | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 6.42 |
| Neuro@home | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 6.42 |
| Lumosity | 2 | 1 | 1 | 1 | 2 | 2 | 1 | 7.14 |
| NeuronUP | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 7.14 |
| Scientific Brain Training Pro | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 7.14 |
| RehaCom | 2 | 1 | 1 | 1 | 2 | 2 | 1 | 7.14 |
| Cognifit | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 8.57 |
| ELENA | 1 | 2 | 2 | 2 | N/A | 2 | 2 | 9.16 |
Adaptation is the measure of the tool's ability to mitigate any sensorimotor barriers that may interfere with efficient use of these tools. Patients with motor or visual disabilities may use adapted input devices such as touch screens, mouse joysticks, modified keyboards, specialised switches, trackballs, and USB or PS/2 devices.12 This criterion also includes the possibility of adapting contents to the patient, for example, by presenting familiar and motivating stimuli.13 The possibility of modifying parameters, such as the number and frequency of sessions, language, sound stimuli, images, and individual tasks and intervention programmes in general, is also considered. Values are assigned according to the level of customisation the tool permits for these parameters. Values listed in Table 1 are as follows: none (0), mitigates sensorimotor barriers or permits adaptation of content (1), and mitigates sensorimotor barriers and permits adaptation of content (2).
Data managementThis criterion measures the capacity for storing such patient data as medical history and results from the neuropsychological evaluation, and in a subsequent stage, for storing data reflecting changes in performance over time. We also assessed the tool's ability to compare the patient's outcome with his or her progress over time (intra-individual), as well as to compare an individual's results with normative data (inter-individual). Values shown in Table 1 are assigned as follows: none (0), permits data storage and management (1), and permits data storage, management, and comparison (2).
Data processingData processing refers to the tool's ability to represent and analyse data and provide feedback. Data are displayed in charts showing patient progress throughout the duration of therapy. The analysis includes data processing at the statistical level to check whether learning has taken place. Data are also compared with previous performances by the same patient and by reference groups. Feedback refers to results that provide recommendations for future sessions (maintain, raise, or lower levels). In turn, this information feeds into the system to make it more efficient when searching for tasks and programmes adapted to patient characteristics. Values are assigned according to the tool's ability to perform all of the above operations. Values shown in Table 1 are assigned as follows: none (0), data representation (1), and data representation, analysis, and feedback (2).
Scientific evidenceEvidence takes into account the studies that have examined using the tool in different disorders. These studies necessarily included ecologically valid, extrapolatable tasks, with sufficiently detailed methods and both control and experimental groups that analysed the efficacy of the tool and monitored the duration of any benefits. Values were assigned according to the number of studies conducted.14 Values appearing in Table 1 were assigned as follows: no studies (0), unpublished studies (1); published studies (2).
PatientsWe examined the type of patient at which these interventions are aimed (children, adults, and elderly patients). Values appearing in Table 1 were assigned as follows: none (0); adults or elderly patients (1); and children/adolescents, adults, and elderly patients (2).
FlexibilityThis parameter assesses whether the platform offers the possibility of creating new tasks and modifying existing ones by changing such parameters as number of stimuli, duration of tasks, type of reinforcement, etc. Values are assigned according to the type of task, ranging from predetermined tasks that cannot be modified to the possibility of creating new tasks, and the ability to customise those already created. Table 1 lists the following values: predetermined tasks only (0), creating new tasks (1), and creating new tasks and modifying old ones (2).
Cognitive rehabilitation softwareGradior15 is a multimedia system used in neuropsychological evaluation and rehabilitation. The system uses a PC to run training programmes that promote functional recovery in patients with cognitive impairment. The system is intended to treat dementia, schizophrenia, cerebral palsy, mental retardation, sequelae of head trauma and of all neurological lesions presenting with cognitive impairment. It allows a large number of users to undergo interventions since tasks may be customised to address specific deficits. This system provides an intervention programme with no need for daily interventions by a professional. Progress can be assessed in reports, and new exercises can be introduced.15,16
RehaCom (HASOMED GmbH, 1996) is a computer-assisted therapy system that enables training design and stimulation for several cognitive functions. The system is made up of a core programme and a number of training procedures. The tasks included are designed to allow modifications to session duration, number of stimuli, number of repetitions, response time, type of reinforcement, and the way instructions are presented. Patients can interact with the computer using a range of devices, such as keyboards, special keyboards with larger push-buttons than those on a conventional keyboard, mouse devices, touch screens, and peripheral devices that eliminate barriers to access for patients with sensorimotor impairment. This system permits individual storage of each user's results and provides a graphic representation of outcomes over time.17,18
Smartbrain (Educamigos) is an interactive and multimedia cognitive stimulation programme offered in CD format and designed to achieve several objectives. First of all, it trains basic cognitive capacities. This software is designed to allow professionals to modify the session duration, number of stimuli, response time, number of repetitions, types of reinforcement, and the way instructions are presented. All of these parameters lend flexibility to designing tasks for each user, but the software does not let professionals design new programmes or different stimuli to avoid overlearning or task automation. Level of difficulty is adjusted automatically to fit the progress made by the user. Furthermore, the therapist can adjust other parameters including session duration, weekly frequency of sessions, or language. Therapeutic efficacy of this programme has been proved in a pilot study with Alzheimer patients.19,20
CogniFit Personal Coach, a brain training tool, is aimed at training diverse cognitive functions in the adult population. The tool allows professionals to evaluate cognitive capacities and choose an appropriate treatment in line with their evaluation. Results are subsequently managed and analysed to generate recommendations for the next training cycle. Results for user progress in different areas are stored in a personalised file that permits analysis of improvements or stabilisation of existing deficits.21–23
Scientific Brain Training Pro (Scientific Brain Training) offers a variety of cognitive rehabilitation programmes designed as therapy for neurodegenerative, neuropsychiatric, and neurotraumatic disorders. These programmes use standard and specialised activities consisting of amusing interactive games specifically designed to stimulate key cognitive functions. Every programme presents a specific cognitive stimulation solution that takes into account the needs of patients with specific impairments who can benefit from cognitive therapies. The programmes include a series of cognitive exercises with defined levels of difficulty that are organised sequentially according to a formula or particular algorithm. Each programme has been designed by specialists and validated by scientific research. Patient progress is measured on a predefined scale of exercise levels.24–27
Lumosity is a cognitive training programme which comprises a set of brain games and exercises. Exercises are designed to target particular cognitive areas; a recommended itinerary can be followed or a personalised training programme can be designed instead. It is oriented towards adults or children with disabilities or healthy individuals who wish to improve their cognitive performance. A study in elderly subjects showed that adults can improve their cognitive abilities, such as memory, processing speed, and reasoning, given proper training.28–31
NeuronUP (Psico 360) is a web platform designed for neuropsychological rehabilitation which focuses on functional cognitive impairments secondary to brain damage (acquired or not) or normal ageing (positive ageing). Professionals can customise tasks to stimulate basic cognitive functions and activities of daily living. Activities can be performed with a computer, paper and pencil, or a touch screen, meaning that therapists can adapt them to any user's level. Furthermore, all exercises have different levels to adapt them to the user's functional performance status.32
The neurorehabilitation platform Neuro@Home (FIVAN) is a tool for home-based rehabilitation aimed at cognitive, motor, and functional rehabilitation of diseases of neurological origin, such as stroke, acquired brain damage, and others. This platform uses new technologies. Clinicians can design exercises, monitor results, and remotely manage treatment plans that are personalised for their patients. Furthermore, doctors can gather extremely detailed data on their patients’ activity.33
The ELENA (ELEctronic Neurocognitive stimulAtion) platform (Brain Dynamics) is a multilayer tool that uses technology to design, execute, and monitor neuropsychological rehabilitation. Patients who may be treated with this tool have a wide age range (children, adults, and elderly patients) and they present cognitive impairment due to neurological and psychiatric diseases. Healthy subjects who wish to improve their performance can also use this tool. This programme permits statistical analysis of results and lets data feed back into the system, which then recommends tasks or intervention programmes for the patient. They include a logical mathematical/statistical system providing the necessary quantification and inference of following a reliable and significant model. This statistical information provides a knowledge base that feeds back into the system to recommend the type of intervention for the patient.34 We should highlight that clinical validation of this tool is still pending. If the study had been completed and published, this platform would have had the highest score according to the criteria used in this review.
The comparison of these platforms (Table 1) displays both the advantages they offer and their current shortcomings.
One common advantage is that they can be applied to different user groups, whether healthy or affected by different diseases. Session number and frequency, user language, sound stimuli, images, individual tasks, and intervention programmes in general can all be customised. Likewise, these tools enable us to store patients’ personal and performance data, and compare their outcomes.
However, many aspects must still be improved, such as computer accessibility for people with sensorimotor deficits by means of different interfaces. Not all platforms permit healthcare professionals to create tasks and itineraries that can be customised and categorised according to the patients’ profiles. Another aspect needing improvement is the possibility of comparing our patients’ results to results from other patients with similar characteristics. The possibility of sharing all the materials used in daily practice with other professionals and users should also be considered. This would help enrich contents and increase the validity of these programmes by means of studies that prove their efficacy.
ConclusionsThe use of new technologies in neuropsychological rehabilitation has been increasing over the past few years. This has helped doctors and therapists do their jobs more efficiently by minimising costs and the time required for a therapist to manage, design, and analyse tasks performed by the patient. This tool provides support but it is no substitute for a doctor. Computers cannot replace a therapist's ability to integrate and understand the cognitive, emotional, and social variables contributing to the rehabilitation process. However, computers can provide objective data on patients’ performance on different cognitive tasks and proposed programmes, as well as a complete statistical analysis of results.
This study has reviewed and compared some of the different software tools for neuropsychological rehabilitation that are currently under development or in the marketing process. In general, we can conclude that these tools enable us to adapt tasks to patients with a range of disabilities in most cases. Cognitive training can be adapted to a wide variety of physical limitations and disabilities. Input devices include touch screens, mouse joysticks, modified keyboards, specialised switches, trackballs, and USB or PS/2 devices. These devices let us measure scores, keep records, register response times, make summary calculations of the sessions which are necessary to assess progress, and obtain immediate feedback. The design of intervention programmes is extremely flexible, which gives rise to a very dynamic learning process. They permit adjustment of time, number of stimuli, and a number of other parameters according to the patient's needs. Adaptation of tasks and personalisation options increase patient motivation. The immediate feedback provided to each patient is important; furthermore, the tool can be configured to provide this feedback in the best way possible. Software tools enable monitoring of patient progress and performance, and let us view and record results after each training session.
Meanwhile, it is important to know the limitations of this type of tool to minimise the negative impact of those limitations on results of use. Some variables, such as lack of familiarity with this type of technology, difficulty using it, lack of human contact, lack of process-oriented feedback, and overlooking emotional variables, could interfere with the patient's rehabilitation. These important aspects must be considered when designing these tools.
Future lines of work for these tools should allow for multidisciplinary integration of all professional profiles that contribute to neurorehabilitation (neurologists, neuropsychologists, psychiatrists, geriatric specialists, speech therapists, occupational therapists, etc.). The design of rehabilitation tasks for these tools should also incorporate multiple aspects of these professionals’ areas of expertise. Tasks should be ecologically valid and adaptable to patients’ needs so that they can be applied to other aspects of their lives. They should allow for participation by a maximum number of stakeholders involved in the process (clinicians, patients, and relatives), and be applicable to as many disorders as possible, without forgetting healthy subjects who wish to increase their cognitive capacity. Tools will be more complete if they consider multiple facets of the patient's life; in addition to training cognitive performance, interventions will target aspects of activities of daily living, psychoeducation, and social skills. Many issues in neurorehabilitation must still be dealt with, and studies on the efficacy of these programmes remain scarce.
FundingPart of this project has been financed by the AVANZA TRACTOR project, approved by the Spanish Ministry of Industry, Energy and Tourism, within the framework of the Strategic Action on Telecommunications and Information Society (Avanza Competitividad R+D subprogramme) and financed by the European Regional Development Fund (ERDF).
Conflict of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Guerrero Pertíñez G, García Linares A. Plataformas de rehabilitación neuropsicológica: estado actual y líneas de trabajo. Neurología. 2015;30:359–366.
64th Annual Meeting of the Spanish Society of Neurology (SEN). Technologies applied in neuropsychological rehabilitation: ELENA (ELEctronic Neurocognitive stimulAtion). November 2012.
articles

Neurología (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals