



Parkinson's disease affects the quality of life of the individual with the disease in addition to creating a burden on the caregiver. Factors related to these effects include motor and non-motor aspects of the disease, as well as traits inherent to the caregiver.
MethodsWe evaluated subjects with Parkinson's disease using the following instruments: Quality of Life Questionnaire PDQ-8, Movement Disorders Society Unified Parkinson's Disease Rating Scale part I to IV (MDS-UPDRS), and Hoehn and Yahr staging. The Zarit Burden Inventory was used to assess all primary caregivers. Major demographic and clinical variables were also recorded.
ResultsA total of 250 subjects with Parkinson's disease were included, of whom 201 had a primary caregiver. In the multivariate analysis, predictors of poor quality of life for a subject with Parkinson's disease were the MDS-UPDRS I score (β=.39, P<.001), MDS-UPDRS II score (β=.21, P<.001), and MDS-UPDRS III score (β=.07, P=.004). Regarding caregiver burden, the MDS-UPDRS II score (β=.54, P=.007) was the most influential factor.
ConclusionsThe present study shows a relationship between quality of life for the subject with Parkinson's disease and the caregiver's perceived burden. However, the factors that determine each situation appear to be distinct.
La enfermedad de Parkinson impacta en la calidad de vida del sujeto que la presenta, pero también ocasiona una carga para el cuidador. Los factores relacionados con estos efectos incluyen aspectos motores y no motores de la enfermedad, así como características inherentes al cuidador.
MétodosSe evaluó a sujetos con enfermedad de Parkinson mediante los siguientes instrumentos: cuestionario de calidad de vida PDQ-8, escala unificada de la enfermedad de Parkinson de la Sociedad de Trastornos del Movimiento parte i a iv (MDS-UPDRS) y estadio de Hoehn y Yahr (HY). A los cuidadores primarios, se les aplicó el inventario de carga del cuidador de Zarit. Adicionalmente, se registraron las principales variables demográficas y clínicas.
ResultadosSe incluyó a 250 sujetos con enfermedad de Parkinson, de los cuales 201 contaban con un cuidador primario. En el análisis multivariado los factores predictores de una peor calidad de vida del sujeto con enfermedad de Parkinson fueron la puntuación de la MDS-UPDRS I (β=0,39, P<0,001), puntuación de la MDS-UPDRS II (β=0,21, P<0,001) y puntuación de la MDS-UPDRS III (β=0,07, P=0,004). En lo que respecta a la carga en el cuidador, la puntuación de la MDS-UPDRS II (β=0,54, P=0,007) fue el que más influyó.
ConclusionesEl presente estudio muestra una relación entre la calidad de vida del sujeto con enfermedad de Parkinson y la percepción de carga del cuidador. No obstante, los factores que determinan cada una de estas parecen ser distintos.
Parkinson's disease (PD) is the second most frequent neurodegenerative disease after Alzheimer disease. As PD progresses, quality of life decreases for PD patients due to motor disability and increased non-motor symptoms.1 The increased disability and symptoms in advanced stages of the disease will require a primary caregiver who will assist the patient with some activities of daily living.2
Caregivers play a key role in preserving an acceptable quality of life and some independence for PD patients, and caregiver presence has been reported to decrease morbidity and mortality rates in PD.3 This role is generally filled by a relative, partner, or close friend. As the disease follows its natural course, caring for the patient frequently becomes the caregiver's main activity.4
It is therefore possible to state that the care provided to PD patients is directly related to caregiver burden. Caregiver burden is defined as the extent to which caregivers perceive that their state of health, social life, and economic status have suffered as a result of caring for PD patients.5 Non-motor symptoms including apathy, depression, impulse control disorder, and cognitive impairment, together with motor complications and falls, add to the burden borne by the caregiver.6
The main aim of this study is to analyse the relationship between caregiver burden and PD patients’ quality of life in PD patients, as well as the factors determining these 2 parameters, in a population attended by one of Mexico's centres of reference.
Subjects and methodsWe performed a transversal analytical study which included consecutive patients diagnosed with PD according to criteria published by the United Kingdom Parkinson's Disease Society Brain Bank.7 These patients were attended at the movement disorders clinic at Instituto Nacional de Neurología y Neurocirugía (Mexico) between June 2012 and May 2013. The primary caregiver was defined as the person closest to the PD patient, whether or not the two are related, who assists with daily activities or provides emotional support. An additional requirement was spending at least 10hours a day with the PD patient.8
We recorded the following demographic data: sex, age, level of education, dominant hand, and place of residence for both patients and caregivers. Clinical variables analysed in PD patients included age at onset of non-motor symptoms, age at diagnosis, and years of disease progression. All subjects with PD were assessed using the Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS)9 and the Hoehn and Yahr (HY) staging scale.10
The MDS-UPDRS is a clinical instrument composed of 4 sections. Parts I and II assess the impact of non-motor and motor symptoms, respectively, on experiences of daily living. Part III refers to motor examination and part IV focuses on motor complications. Part I includes a questionnaire assessed by a rater as well as a self-administered questionnaire.
HY stages are used to determine disease severity based on the location of the involvement, functional capacity, postural stability, and gait. PD severity was categorised as mild (HY 1 and 2), moderate (HY 3), or severe (HY 4 and 5).
Patients were also administered the Spanish-language version of the PD quality of life questionnaire (PDQ-8). PDQ-8 is a short form of the PDQ-39. This questionnaire includes 8 items that assess the frequency of different events related to quality of life. Score is obtained by calculating a single summary index extracted from the user manual, where the highest score indicates a poorer quality of life (on a scale of 0-100).11 PDQ-8 was used with permission from Oxford University (United Kingdom).
Meanwhile, caregivers were asked to provide the following sociodemographic data: sex, age, level of education, religion, type of relationship with the patient, and the mean number of years caring for the patient. All caregivers completed the Zarit Caregiver Burden Interview (ZCBI).5 Higher scores (on a scale from 0 to 88) indicate a greater burden perceived by the caregiver. Using this scale, the caregiver experience is classified as ‘without burden’ (below 46 points), ‘mild burden’ (47-55 points), and ‘severe burden’ (higher than 55 points). For the purposes of this study, the caregiver experience was also divided into ‘without burden’ (< 47) and ‘with burden’ (≥ 47).
Both PDQ-8 and ZCBI were administered on an individual basis and in separate physical areas to avoid any information biases caused by the presence of the patient. The study was approved by the local Research Ethics Committee. All participants signed an informed consent form.
Statistical analysisWe used measures of central tendency and dispersion in the descriptive analysis; the t-test or its non-parametric alternative was used as appropriate to compare quantitative variables. Analysis of variance was used to compare quantitative variables between more than 2 groups. The chi-square test was used to compare qualitative variables. The Pearson correlation coefficient was calculated for correlations between PDQ-8 and ZCBI scores. Statistical analysis was completed with SPSS version 17 (SPSS Inc). Two linear regression models were developed, using the PDQ-8 score as the dependent variable in one case, and ZCBI in the other. Independent variables included age, sex, progression time, disease severity, and motor and non-motor scales on the MDS-UPDRS. We ruled out presence of collinearity and interaction by using the variance inflation factor and interaction terms, respectively. Values of P<.05 were considered statistically significant.
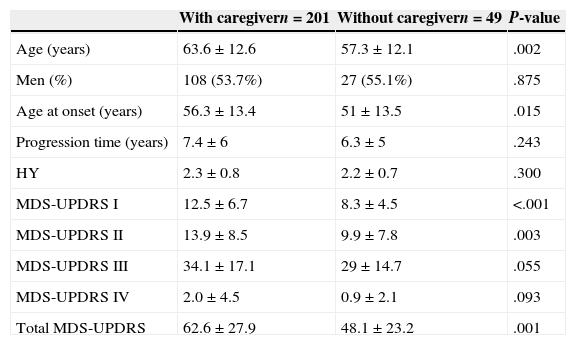
ResultsCharacteristics of PD patients and their caregiversWe interviewed a total of 250 patients with PD; 49 attended the interview without a caregiver, and were therefore excluded from the caregiver burden analysis. Table 1 shows a comparison of PD patients with and without caregivers. The total sample included 201 subjects with PD and their corresponding caregivers. Characteristics of both groups are shown in Table 2. All caregivers were relatives of the PD patients. In 53.2% of all cases (n=107), the caregiver was the patient's partner; 30.3% of the caregivers (n=61) were the patient's son/daughter. Caregivers for 88% of the men with PD were woman; in turn, 44.1% of women with PD were cared for by men. The number of days dedicated to the care of PD patients was higher for patients’ partners than for other relatives (6.8±0.8 vs 5.9±1.5; P>.001).
Comparison of clinical characteristics of PD patients with and without a primary caregiver.
| With caregivern=201 | Without caregivern=49 | P-value | |
|---|---|---|---|
| Age (years) | 63.6±12.6 | 57.3±12.1 | .002 |
| Men (%) | 108 (53.7%) | 27 (55.1%) | .875 |
| Age at onset (years) | 56.3±13.4 | 51±13.5 | .015 |
| Progression time (years) | 7.4±6 | 6.3±5 | .243 |
| HY | 2.3±0.8 | 2.2±0.7 | .300 |
| MDS-UPDRS I | 12.5±6.7 | 8.3±4.5 | <.001 |
| MDS-UPDRS II | 13.9±8.5 | 9.9±7.8 | .003 |
| MDS-UPDRS III | 34.1±17.1 | 29±14.7 | .055 |
| MDS-UPDRS IV | 2.0±4.5 | 0.9±2.1 | .093 |
| Total MDS-UPDRS | 62.6±27.9 | 48.1±23.2 | .001 |
HY: Hoehn and Yahr; MDS-UPDRS: Movement Disorder Society – Sponsored Revision of the Unified Parkinson's Disease Rating Scale.
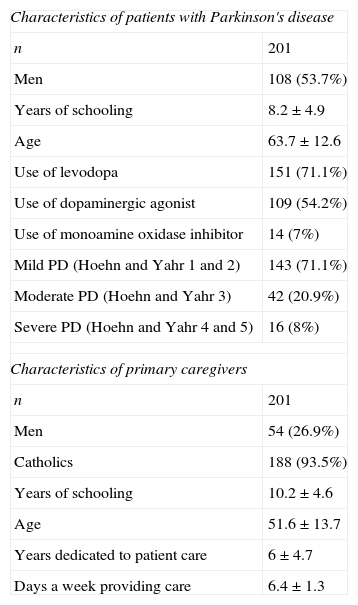
Clinical characteristics of PD patients with a primary caregiver.
| Characteristics of patients with Parkinson's disease | |
| n | 201 |
| Men | 108 (53.7%) |
| Years of schooling | 8.2±4.9 |
| Age | 63.7±12.6 |
| Use of levodopa | 151 (71.1%) |
| Use of dopaminergic agonist | 109 (54.2%) |
| Use of monoamine oxidase inhibitor | 14 (7%) |
| Mild PD (Hoehn and Yahr 1 and 2) | 143 (71.1%) |
| Moderate PD (Hoehn and Yahr 3) | 42 (20.9%) |
| Severe PD (Hoehn and Yahr 4 and 5) | 16 (8%) |
| Characteristics of primary caregivers | |
| n | 201 |
| Men | 54 (26.9%) |
| Catholics | 188 (93.5%) |
| Years of schooling | 10.2±4.6 |
| Age | 51.6±13.7 |
| Years dedicated to patient care | 6±4.7 |
| Days a week providing care | 6.4±1.3 |
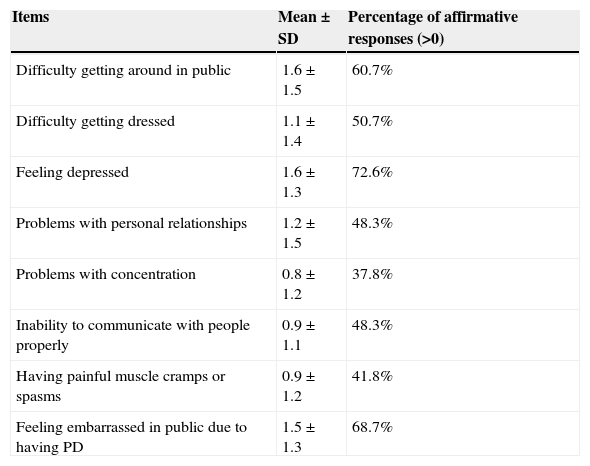
Mean score on the PDQ-8 scale was 29.7±22 (range: 0–100; median: 25). The most frequently cited emotions were depression and feeling embarrassed in public. Table 3 shows the frequency of affirmative responses and the mean score on each item of the PDQ-8.
Frequency and mean score on items on the PDQ-8 scale.
| Items | Mean±SD | Percentage of affirmative responses (>0) |
|---|---|---|
| Difficulty getting around in public | 1.6±1.5 | 60.7% |
| Difficulty getting dressed | 1.1±1.4 | 50.7% |
| Feeling depressed | 1.6±1.3 | 72.6% |
| Problems with personal relationships | 1.2±1.5 | 48.3% |
| Problems with concentration | 0.8±1.2 | 37.8% |
| Inability to communicate with people properly | 0.9±1.1 | 48.3% |
| Having painful muscle cramps or spasms | 0.9±1.2 | 41.8% |
| Feeling embarrassed in public due to having PD | 1.5±1.3 | 68.7% |
SD: standard deviation; PDQ-8: 8-item Parkinson's Disease Questionnaire on quality of life.
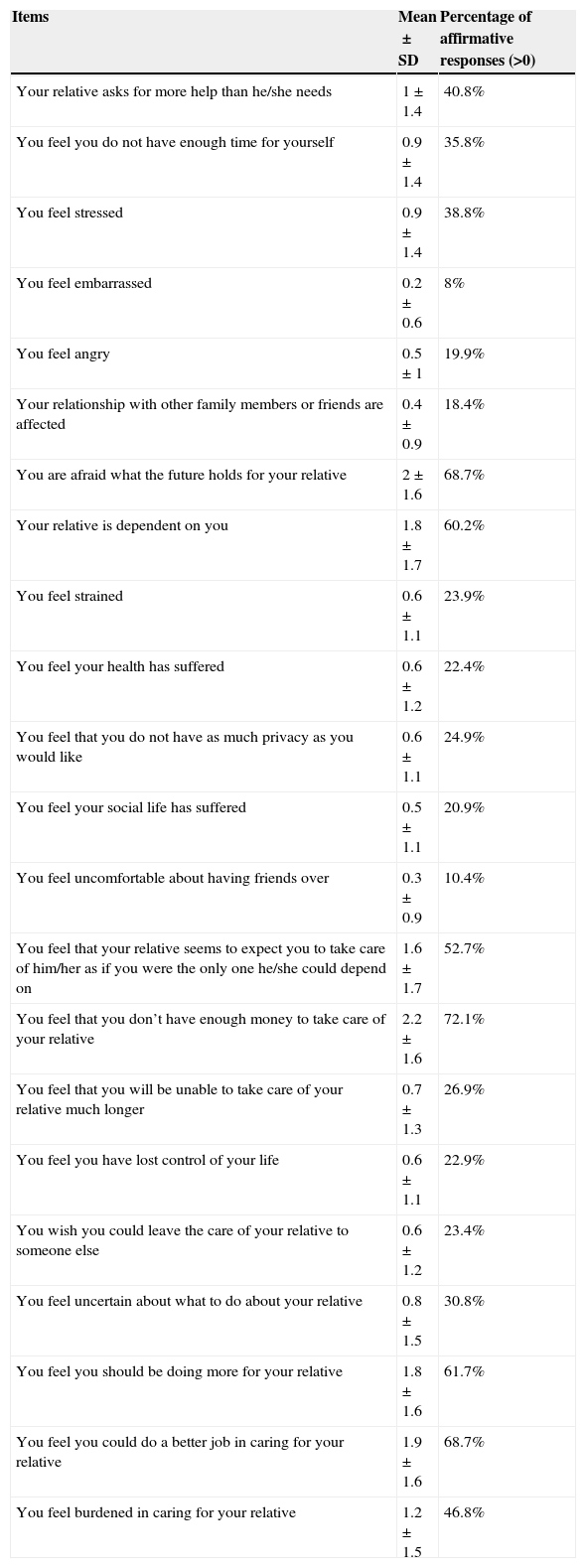
Mean score on the ZCBI scale was 21.5±16.3 (range: 0-85; median: 19). The caregivers’ main concerns were uncertainty about the future and financial difficulties resulting from having to care for PD patients. On the other end, the least common item was feeling ashamed of their caregiving role. Table 4 shows the distribution of affirmative responses for each item on the ZCBI, as well as range and median.
Frequency and distribution of responses to items on the Zarit Caregiver Burden Interview.
| Items | Mean±SD | Percentage of affirmative responses (>0) |
|---|---|---|
| Your relative asks for more help than he/she needs | 1±1.4 | 40.8% |
| You feel you do not have enough time for yourself | 0.9±1.4 | 35.8% |
| You feel stressed | 0.9±1.4 | 38.8% |
| You feel embarrassed | 0.2±0.6 | 8% |
| You feel angry | 0.5±1 | 19.9% |
| Your relationship with other family members or friends are affected | 0.4±0.9 | 18.4% |
| You are afraid what the future holds for your relative | 2±1.6 | 68.7% |
| Your relative is dependent on you | 1.8±1.7 | 60.2% |
| You feel strained | 0.6±1.1 | 23.9% |
| You feel your health has suffered | 0.6±1.2 | 22.4% |
| You feel that you do not have as much privacy as you would like | 0.6±1.1 | 24.9% |
| You feel your social life has suffered | 0.5±1.1 | 20.9% |
| You feel uncomfortable about having friends over | 0.3±0.9 | 10.4% |
| You feel that your relative seems to expect you to take care of him/her as if you were the only one he/she could depend on | 1.6±1.7 | 52.7% |
| You feel that you don’t have enough money to take care of your relative | 2.2±1.6 | 72.1% |
| You feel that you will be unable to take care of your relative much longer | 0.7±1.3 | 26.9% |
| You feel you have lost control of your life | 0.6±1.1 | 22.9% |
| You wish you could leave the care of your relative to someone else | 0.6±1.2 | 23.4% |
| You feel uncertain about what to do about your relative | 0.8±1.5 | 30.8% |
| You feel you should be doing more for your relative | 1.8±1.6 | 61.7% |
| You feel you could do a better job in caring for your relative | 1.9±1.6 | 68.7% |
| You feel burdened in caring for your relative | 1.2±1.5 | 46.8% |
SD: standard deviation.
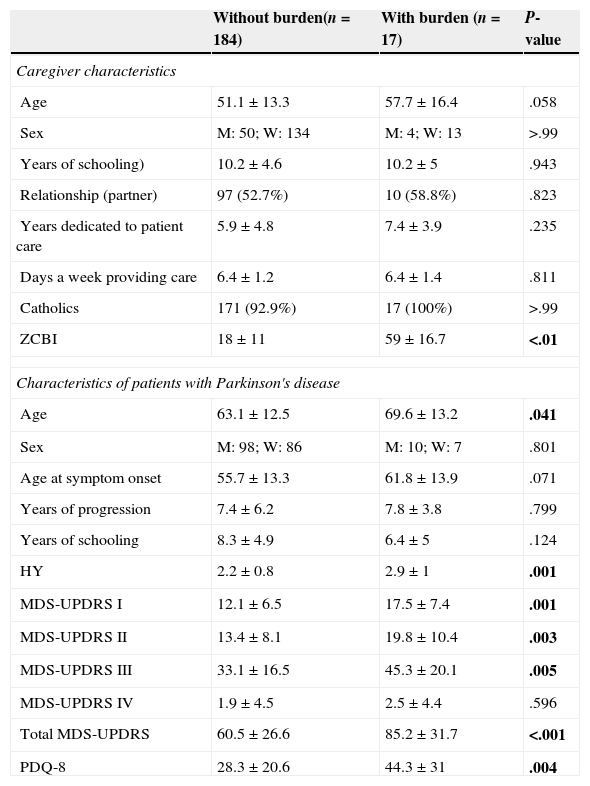
When data were categorised by caregivers’ perceptions, 91.5% reported no burden, 3.5% (n=7) perceived mild burden, and 5% (n=10) perceived high burden. Table 5 shows a comparison of characteristics of the PD patients and their caregivers. Caregivers are grouped by perceived burden (present or absent).
Comparison of characteristics of caregivers and patients with PD regarding burden presence.
| Without burden(n=184) | With burden (n=17) | P-value | |
|---|---|---|---|
| Caregiver characteristics | |||
| Age | 51.1±13.3 | 57.7±16.4 | .058 |
| Sex | M: 50; W: 134 | M: 4; W: 13 | >.99 |
| Years of schooling) | 10.2±4.6 | 10.2±5 | .943 |
| Relationship (partner) | 97 (52.7%) | 10 (58.8%) | .823 |
| Years dedicated to patient care | 5.9±4.8 | 7.4±3.9 | .235 |
| Days a week providing care | 6.4±1.2 | 6.4±1.4 | .811 |
| Catholics | 171 (92.9%) | 17 (100%) | >.99 |
| ZCBI | 18±11 | 59±16.7 | <.01 |
| Characteristics of patients with Parkinson's disease | |||
| Age | 63.1±12.5 | 69.6±13.2 | .041 |
| Sex | M: 98; W: 86 | M: 10; W: 7 | .801 |
| Age at symptom onset | 55.7±13.3 | 61.8±13.9 | .071 |
| Years of progression | 7.4±6.2 | 7.8±3.8 | .799 |
| Years of schooling | 8.3±4.9 | 6.4±5 | .124 |
| HY | 2.2±0.8 | 2.9±1 | .001 |
| MDS-UPDRS I | 12.1±6.5 | 17.5±7.4 | .001 |
| MDS-UPDRS II | 13.4±8.1 | 19.8±10.4 | .003 |
| MDS-UPDRS III | 33.1±16.5 | 45.3±20.1 | .005 |
| MDS-UPDRS IV | 1.9±4.5 | 2.5±4.4 | .596 |
| Total MDS-UPDRS | 60.5±26.6 | 85.2±31.7 | <.001 |
| PDQ-8 | 28.3±20.6 | 44.3±31 | .004 |
M: men; HY: Hoehn and Yahr; W: women; MDS-UPDRS: Movement Disorder Society – Sponsored Revision of the Unified Parkinson's Disease Rating Scale; PDQ-8: 8-item Parkinson's Disease Questionnaire on quality of life; ZCBI: Zarit Caregiver Burden Interview.
Bold-type: statistically significant.
We identified a moderate correlation between the quality of life of PD patients and caregiver burden: poorer quality of life is linked to higher burden for the caregiver (r=.35, P<.001).
Quality of life multivariate analysisThe linear regression analysis showed that the predictors of poorer quality of life for PD patents were scores on the MDS-UPDRS I scale (β=.39, P<.001), scores on the MDS-UPDRS II scale (β=.21, P<.001), and scores on the MDS-UPDRS III scale (β=.07, P<.004). Age, progression time, and severity according to the HY and MDS-UPDRS IV scales were not statistically significant in the model.
Multivariate analysis of caregiver burdenScore on the MDS-UPDRS II scale (β=.54, P<.007) was the only variable affecting perceived burden on the ZCBI.
DiscussionDecreased quality of life of PD patients becomes more pronounced as the disease progresses. Some studies have reported that determinants of poorer quality of life in PD patients include presence of depression, a higher score on the activities of daily life section of the UPDRS, disease severity, and cognitive dysfunction.12,13 Non-motor and motor characteristics of the disease measured with the MDS-UPDRS were the main determinants of quality of life of PD patients in our study. In general terms, part I showed a higher impact on quality of life than part II, which underscores the relevance of neuropsychiatric symptoms, such as depression and cognitive impairment, in patients with PD. A recent study reports that behavioural problems associated with executive function in PD patients explain an important percentage of the burden perceived by caregivers.14 Another study describes that even mild cognitive impairment in PD patients has an impact on caregiver burden.15
Part III of the MDS-UPDRS includes the motor examination performed by a neurologist. As before, a higher score on this subscale points to a poorer quality of life.
Regarding caregiver burden, we should highlight that patients in advanced stages of PD experience more difficulty performing activities of daily life, and therefore require a caregiver. In our study, 80.4% of the patients had a primary caregiver at the time of the evaluation. Researchers have reported that patients in the very early stages of PD, who have less disease severity and minimal difficulty performing activities of daily life, do not generally need a caregiver.16 Most PD patients in our study were in mild to moderate stages of the disease. Comparing patients with and without caregivers revealed no statistically significant differences in severity (HY). However, PD patients with caregivers were older and had higher scores on the MDS-UPDRS regarding motor and non-motor experiences on activities of daily life. Likewise, they had lower scores (approaching significance) on motor examination. These results indicate that limitations on daily life activities, and not only motor status, make it necessary for the patient to have a caregiver. However, we should not rule out the possibility of a selection bias since our study population is relatively young and patients in advanced stages of the disease are scarcely represented. In later stages, non-motor symptoms play a more important part in the burden on the caregiver.
In all cases, the role of the caregiver was occupied by a relative. This situation can be explained by the socioeconomic level of the study population, although other social and cultural characteristics of the Mexican population might also contribute. An important consideration of having a family member as the caregiver is the training that he/she may or may not have received on caring for a PD patient. Studies from other countries have reported that 82.6% of their surveyed primary caregivers have attended some training programme on PD management.17 Mexican associations and support groups providing training to caregivers for this type of patients do not yet have sufficient presence. The impact or burden that the caregiver may feel might be modified by receiving pertinent training.
Other noteworthy features are that 3 of every 4 caregivers were women, the mean age of caregivers in our sample was 52 years, and the mean number of years dedicated to PD patient care was 6 years. Studies from different countries have reported similar sex distributions; however, the mean age in our caregiver sample was nearly 10 years younger than in other samples.6,13 This age difference is significant since these caregivers are of working age but must dedicate most of their time to caring for a relative with PD. Further specific studies on the financial impact of this situation are needed.
The burden perceived by caregivers in our study was measured using the ZCBI, which delivered a score of 22 points. The longitudinal Parkinson's disease patient study (Estudio longitudinal de pacientes con enfermedad de Parkinson, ELEP) included 289 Spanish patient-caregiver pairs and reported a mean score of 18.1±13.9 on the ZCBI.18 A recently published study undertaken in a Brazilian population reported a mean ZCBI score of 20.2 points in 50 patient-caregiver pairs.19
Factors related to an increase in caregiver burden include aspects linked to both the caregiver and the disease itself. Caregiver age has been described as the main determinant, since younger caregivers perceive increased burden.8,13 We did not find any statistically significant differences in our study sample between caregivers with and without burden. The ZCBI item with the highest number of affirmative responses referred to the financial situation; this concern was also reported as one of the main determinants of stress in caregivers interviewed in the framework of the recent Parkinson's UK Members’ Survey.20
On the other hand, factors inherent to PD that affect caregiver burden are disease severity and duration, degree of disability of the PD patient, motor symptoms, falls, and such non-motor symptoms as depression, autonomic dysfunction, pain, and fatigue.21,22 Older age of PD patients, more severe PD according to the HY scale, and higher scores on the MDS-UPDRS were associated with a higher prevalence of burden in our study. With regard to the domains assessed by the MDS-UPDRS, motor experiences of daily living and motor assessment were the most frequently associated with caregiver burden. Only the score on the MDS-UPDRS II had an impact on the degree or intensity of caregiver burden in the multivariate analysis. This seems to indicate that motor aspects rather than non-motor aspects determine caregiver burden in our study population.
One of our study's limitations is that no clinical instruments were used to measure caregivers’ quality of life. Other studies have suggested that caregivers of PD patients also present a poorer quality of life.23 We also highlight the characteristics of our sample, since we included patients with PD from a specific hospital population. We should highlight the scarce presence of patients in advanced stages of the disease, possibly because caregivers cannot bring patients from their homes to the hospital. Therefore, the results observed cannot be generalised.
In conclusion, we observed a relationship between quality of life of PD patients and the burden perceived by the caregiver. However, factors determining these two aspects are very distinct, and neurologists should be aware of this when working to improve quality of life for patients and decrease the burden perceived by the caregiver.
FundingNo funding was necessary for the completion of the study.
Conflict of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Rodríguez-Violante M, Camacho-Ordoñez A, Cervantes-Arriaga A, González-Latapí P, Velázquez-Osuna S. Factores asociados a la calidad de vida de sujetos con enfermedad de Parkinson y a la carga en el cuidador. Neurología. 2015;30:257–263.
