






A 55-year-old man presented to the emergency department with jaundice, intense pruritus, choluria, and acholia. The patient had a history of acute pre-B lymphoblastic leukemia (ALL), treated with several lines of chemotherapy, complete cure and subsequent relapse, and finally he received an allogeneic stem cell transplantation in 2018 reaching remission. Physical examination was only notable for intense jaundice, there was no abdominal pain or fever. Laboratory studies showed a total bilirubin level of 13.85mg/dL (NV 0.3–1.9mg/dL) with a direct bilirubin level of 11.80mg/dL (NV 0–0.3mg/dL).
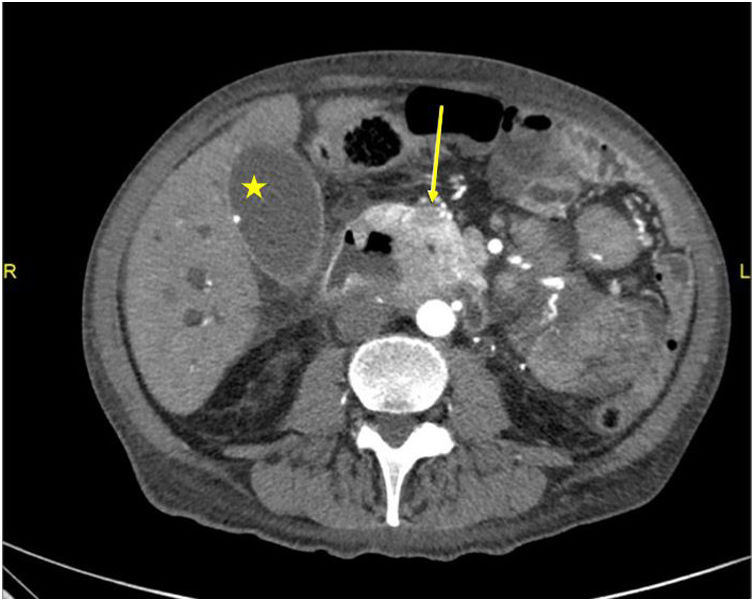
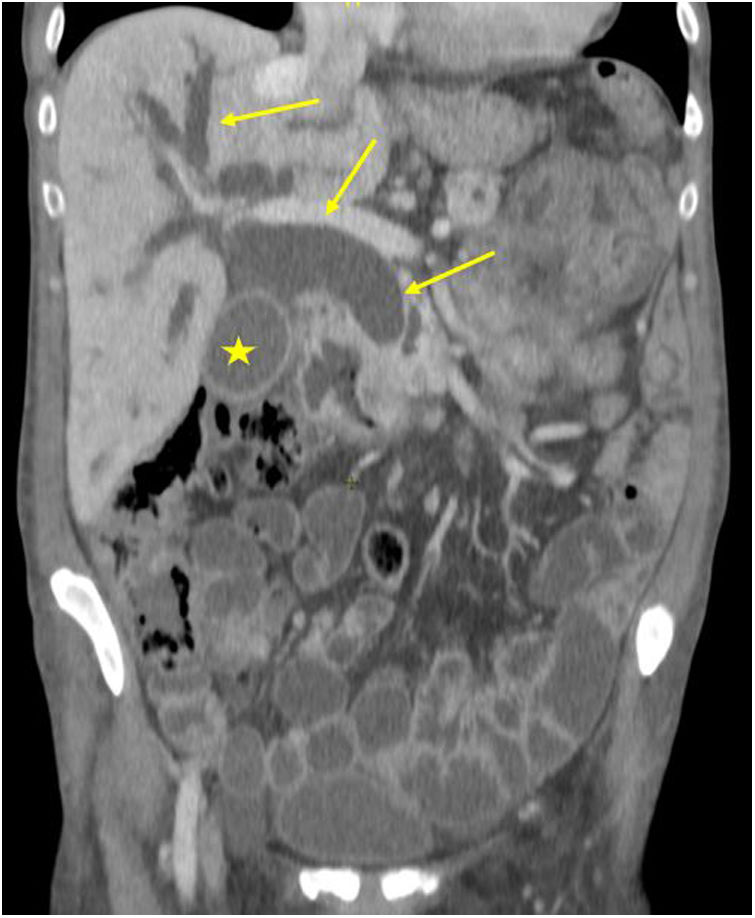
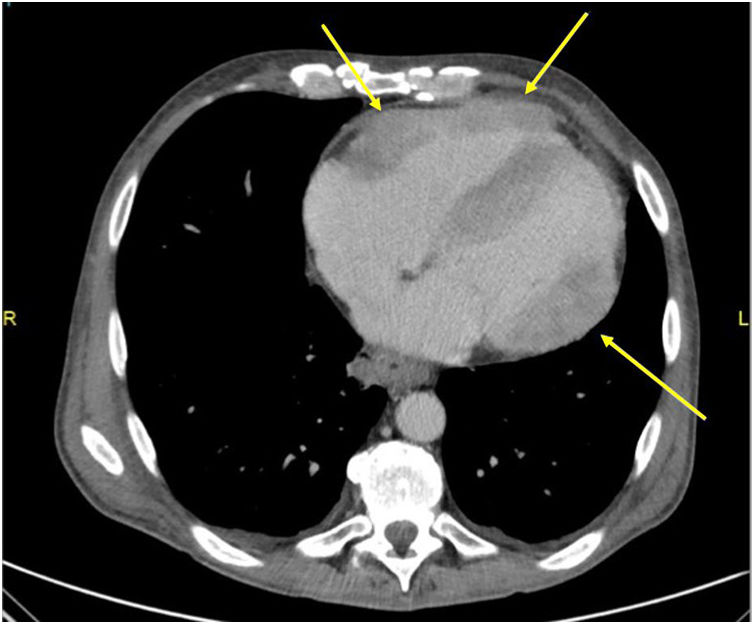
Full-body computerized tomography revealed a biliary obstruction by an ulcerated tumor of the duodenum-pancreatic crossroads (Figs. 1 and 2) with nodular lesions suggestive of chloromas in the pancreas, right kidney, myocardium (Fig. 3) and lung. Duodenal infiltrate biopsies showed lymphoblastic lymphoma (CD34+, CD117+, TdT−) with partial differentiation to B-phenotype (CD79+, PAX 5+, CD20−, CD19−). Rescue chemotherapy was begun but finally, the patient died in the Intensive Care Unit due to refractory septic shock.
Chloroma or myeloid sarcoma is a rare extramedullar manifestation of hematological malignancies. It can be the evolution of acute uncured leukemia or debut as a relapse, especially after allogeneic hematopoietic stem cell transplantation.1 Locations and most affected organs are orbit, bone, skin, spine, lymph nodes, and gastrointestinal tract.2 High suspicion is necessary to reach an early diagnosis and improve prognosis.3
