





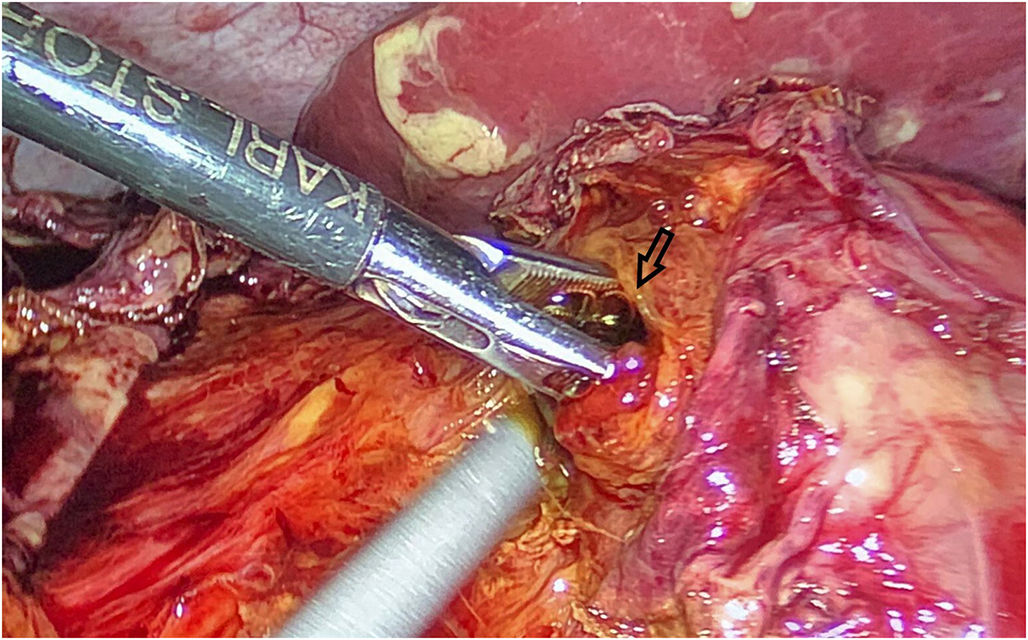
This is a case of an 18-year-old male patient who sustained injuries from a motor vehicle crash. Contrast-enhanced computed tomography (CECT) scan of the body was performed upon arrival at the emergency department. There was a small amount of free abdominal fluid in contact with the right psoas muscle, without any other significant finding (fig. 1A, arrow). The patient was hemodynamically stable and other routine analysis were all within normal values, non-operative management (NOM) was considered. Twenty-four hours after injury, the patient manifested severe abdominal pain, fever and leukocytosis. Repeat abdominal CECT scan was performed, showing (fig. 1B-C) an increased amount of free abdominal fluid (arrow) and free air (arrow heads) in the right retroperitoneal space below to duodenum (asterisk). These findings suggested a hollow viscus perforation, probably in the second part of the duodenum. The patient underwent exploratory laparoscopy, revealing 1-cm diameter perforation of the duodenal wall on the second portion of duodenum (fig. 2). A primary repair of the duodenum was performed using an interrupted suturing technique. There were no further complications and patient was discharged 7 days after surgery.
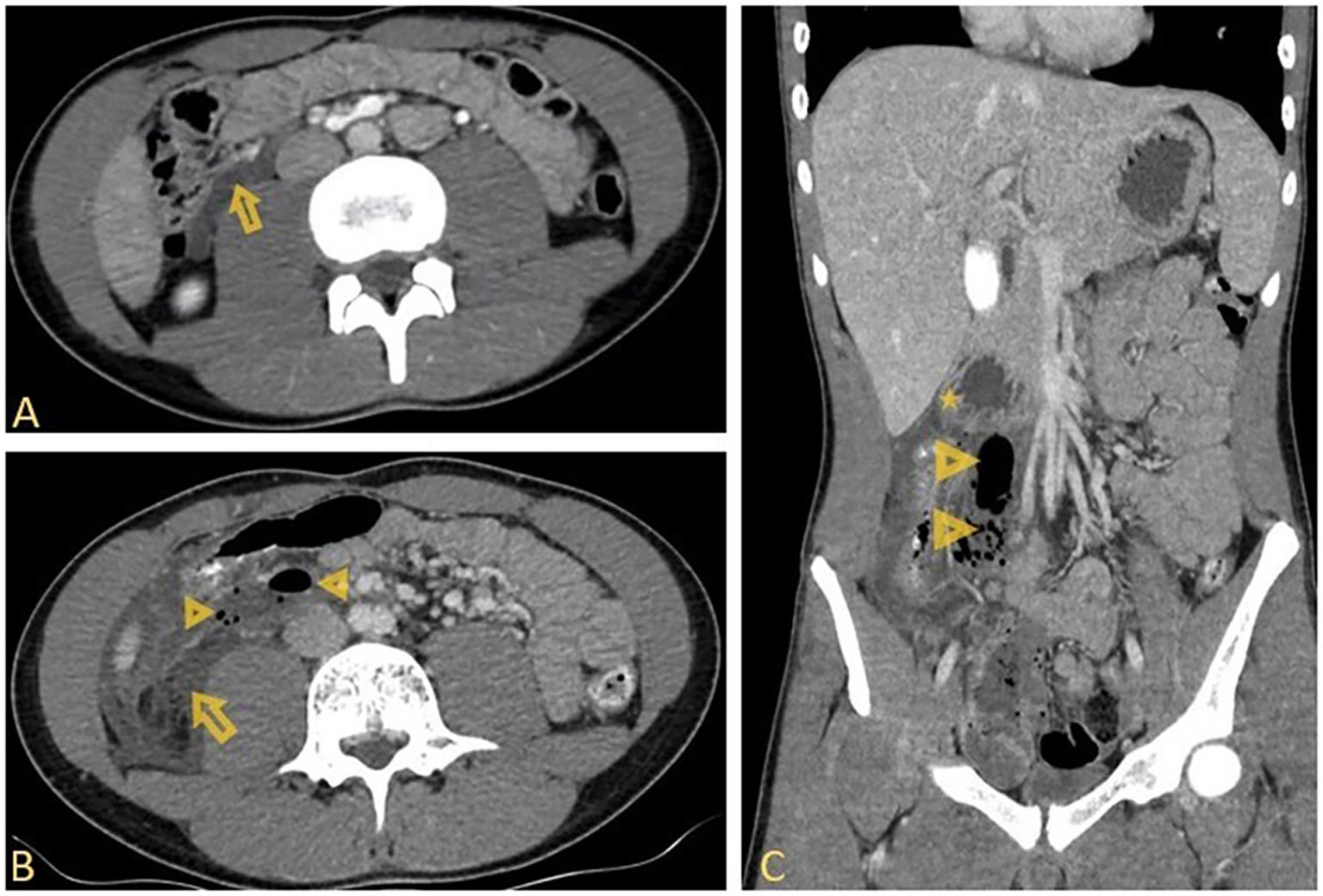
Isolated duodenal injury is found in 0.2% of blunt trauma patients, with males being commonly affected. Clinical signs of peritoneal irritation are usually absent in duodenal injury because most of the duodenum is located in the retroperitoneal space. This can lead to a delay in diagnóstico or a misdiagnosis, which can have serious consequences, such as sepsis and increase risk of death. For this reason, it is essential to know the signs of duodenal injury seen on CT. Duodenal perforation should be suspected if there is a retroperitoneal collection of the contrast medium, extraluminal gas, or a lack of continuity of the duodenal wall; these should be identified because duodenal perforation would require surgical management. These findings are differentiated from duodenal contusion that may be treated through NOM, characterized by edema or hematoma of the duodenal wall, intramural gas accumulations, and focal duodenal wall thickening (>4 mm). Retroperitoneal fluid or hematoma, or stranding of retroperitoneal fatty tissue can be found in both conditions.
Declaration of interestsThe authors have no conflicts of interest to declare. All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report.
