






The COVID-19 pandemic accelerated the adoption of online counselling in social care, a development that may permanently alter professional practices. However, the full extent of its utilisation, associated occupational risks, and impacts on health remain underexplored. This study investigates the effects of digitisation on the traditionally face-to-face profession of counselling. We conducted a cross-sectional web survey involving 1049 German counsellors to examine the prevalence of online counselling, remote work, and their associations with occupational risks and health outcomes such as musculoskeletal symptoms, cognitive fatigue, and sleep disorders. Our analysis utilised Kruskal-Wallis tests and multiple regression. Findings reveal that only 9.5 % of participants belonged to the high user group, yet high online usage was associated with more favourable working conditions, including lower emotional burden (p = 0.01), and reduced cognitive fatigue (b = 0.22, p < 0.001) and sleep disorders (b = 0.17, p = 0.004) compared to medium users. Engaging in remote work more than once a week was linked to lower cognitive fatigue compared to doing so up to once a week (b = 0.10, p = 0.03). No correlation was observed between musculoskeletal symptoms and the frequency of online counselling or remote work. These results indicate that online counselling could enhance working conditions, although initial increases in cognitive fatigue may occur as counsellors adapt. The findings underscore the need for continued efforts to improve digital working conditions in social care.
“Anticipating and managing change in the context of green, digital, and demographic transitions” is a central priority of the European Commission's Strategic Framework on Health and Safety at Work 2021–2027 (European Commission, Directorate-General for Employment, Social Affairs & Inclusion, 2021). A recent report by the European Agency for Safety and Health at Work (EU-OSHA) highlights the transformative impact of digitalisation on the HeSCare sector—encompassing healthcare, residential care, and social work. This report presents both opportunities for improvement and challenges to working conditions (European Agency for Safety & Health at Work, 2024). It emphasises the need to enhance the visibility of occupational safety and health (OSH) situations for HeSCare workers, especially as emerging risks associated with digitalisation continue to evolve. While the effects of digitalisation on healthcare professionals such as physicians and nurses have been extensively studied (Razavi et al., 2022; Virtanen et al., 2023), its impact on social work and the counselling profession has often been overlooked. However, with over 5 million people employed in the EU's social work sector in 2022—an increase of 1.1 million since 2013—there is an urgent need for more research on how digitalisation affects working conditions and health outcomes (European Agency for Safety & Health at Work, 2024). This need is particularly important given the widespread adoption of digital tools, with >86 % of social work establishments now relying on devices such as computers, tablets, or smartphones in their daily operations.
Online counselling, as defined by Mallen et al., refers to any form of asynchronous or synchronous non-face-to-face communication using digital technologies, including telephone, email, chat, and video calls (Mallen & Vogel, 2005). While some organisations offered digital services before the COVID-19 pandemic, online counselling remained a marginal practice in Germany's social care sector (Schlenger et al., 2022). However, the pandemic's isolation and quarantine measures accelerated the adoption of digital services to maintain access to essential services and prevent organisational crises (Nordesjö et al., 2022; Nordesjö & Scaramuzzino, 2023). Despite this shift, the prevalence of online counselling in Germany and its effects on work characteristics and employee well-being remain largely unexamined, highlighting the need for further research. While digitalisation's broader impact on workplace dynamics and health has been studied across various industries, its specific implications for social care are still insufficiently understood.
This paper explores how digitalisation affects working conditions and OSH in social counselling, with a focus on online counselling services. The following sections examine these effects within the demands-resources model proposed by Bakker et al. (Section 1.1) (Bakker & Demerouti, 2007) as a conceptual framework. A comprehensive literature review then provides an overview of the current state of digitalisation in social care and its effects on both counsellors and clients (Section 1.2). Finally, the research questions and their respective rationales are outlined in relation to the findings from the literature review (Section 1.2).
Digitalisation and the workplaceDigitalisation is fundamentally reshaping work conditions by introducing digital job demands and resources into the traditional demands-resources model (Bakker & Demerouti, 2007; Demerouti et al., 2001; Scholze & Hecker, 2023). According to this model, work conditions can be either demanding—such as increased workload, which may lead to job strain, burnout, and health issues—or resourceful, providing factors such as autonomy, which can enhance motivation and job satisfaction, potentially counteracting the negative effects of job demands and promoting well-being (Bakker & Demerouti, 2007; Demerouti et al., 2001).
Various studies have highlighted both positive and negative effects of digitalisation in the workplace. While digital technologies can streamline processes and improve communication, they also increase job pressure (Scholze & Hecker, 2023). For instance, constant connectivity often results in employees being available beyond work hours, blurring the boundaries between personal and professional life and contributing to work-life conflicts (Boswell & Olson-Buchanan, 2007; Leung, 2011). Furthermore, a growing dependence on digital technology can lead to significant interruptions when malfunctions occur, increasing job frustration and stress, and ultimately impairing performance (Scholze & Hecker, 2023; Stenfors et al., 2013; ter Hoeven & van Zoonen, 2015). Additionally, digitalisation may intensify workloads by increasing task volume and execution speed, placing greater demands on employees (Carlson et al., 2017; Scholze & Hecker, 2023). Employees often feel pressured to respond more quickly, multitask, and handle additional IT-related administrative tasks, which can contribute to stress and decrease job satisfaction (Scholze & Hecker, 2023). At the same time, digital tools have reshaped workplace collaboration by facilitating data sharing, potentially enhancing accessibility, performance, and job satisfaction (Day et al., 2010; Scholze & Hecker, 2023). However, these tools can also reduce face-to-face interaction, increasing the risk of social isolation and weakening connections with office-based colleagues (Collins et al., 2016).
Despite these challenges, digitalisation can also help to mitigate job strain and improve well-being and job satisfaction when effectively managed (Cijan et al., 2019). In response to evolving OSH challenges, organisations are increasingly adopting international standards such as the International Organization for Standardization (ISO) 45,001 (International Organization for Standardization, 2018). This framework provides guidelines for OSH management and mandates responsibility for worker safety, even in digitalised settings (International Organization for Standardization, 2018). In Germany, the standard is implemented through legally required OSH risk assessments as outlined by the German Guideline of Health and Safety (GDA) (Gemeinsame Deutsche Arbeitsschutzstrategie (GDA), 2018). These assessments cover various aspects of work, including content, organisation, social interaction, and work environment, as well as emerging forms of work such as flexible and remote work (Gemeinsame Deutsche Arbeitsschutzstrategie (GDA), 2018). The effectiveness of these management standards depends on factors such as organisational context, scope, and the inherent nature of activities and risks (International Organization for Standardization, 2018). Similarly, the impact of digital technologies on employees’ health is influenced by both organisational and personal factors, including boundary management and occupation type (Beckel & Fisher, 2022; Bulger et al., 2007; Vander Elst et al., 2017). This variability suggests that the overall impact of digitalisation on OSH management may not be directly transferable to the social care sector. Given the limited research in this area, our study aims to fill this gap by generating evidence for a safe and thriving future for both organisations and employees, while evaluating the universality of current guidelines across specific occupational fields.
Social counsellingSocial counselling addresses sensitive topics such as substance abuse, pregnancy, and migration, often requiring intensive personal contact and relationship-building between counsellors and clients (Rollins, 2020). However, social care workers also face significant demands related to documentation and preparation in order to adequately address these emotionally charged topics (Blomberg et al., 2015; Reamer, 2005). Combined with the strain of working with challenging clients, these demands can contribute to stress levels that are higher than average compared to other occupations. According to the EU-OSHA, 18 % of social workers across the EU report exposure to difficult customers and patients, nearly double the 10 % average across all professions (European Agency for Safety & Health at Work, 2024). Additionally, 8 % of social workers experience violence, bullying, or harassment in the workplace. More than 70 % of social work establishments cite work-related stress as a concern, significantly exceeding the 46 % average across all occupational groups (European Agency for Safety & Health at Work, 2024). Given the already high stress levels in social care, it is crucial to assess the impact of online counselling on the occupational health of counsellors.
Prior to the COVID-19 pandemic, online counselling in Germany was primarily viewed as a supplementary tool, often used to initiate contact before in-person sessions (Schlenger et al., 2022). However, during the pandemic, the use of digital services in social care surged to ensure continued access to services and to mitigate social isolation, particularly for vulnerable groups (Nordesjö et al., 2022; Nordesjö & Scaramuzzino, 2023). While data on the pre-pandemic prevalence of online counselling in general is limited, evidence from German family counselling organisations highlights a sharp increase in the use of different digital services (Lüken-Klaßen et al., 2021). The proportion of institutions offering telephone counselling more than once a week increased from 47 % in 2019 to 81 % in 2020, while the use of video counselling rose from 5 % before the pandemic to 55 % by May 2020. Despite this rapid shift, the long-term impact remains unclear, especially as factors like organisational preparedness, which have historically influenced the adoption of digital services, were neglected during the emergency transitions caused by the pandemic. To address the research gap, the following research question (RQ1) was proposed:
Research Question (RQ) 1: What is the extent of online counselling among counsellors in a large German welfare organisation after the COVID-19 pandemic in 2022?
Like digitalisation in general, digital or online counselling can have both positive and negative effects on clients, counsellors, and their relationships. Research shows that frequent users tend to be more sceptical of further digitalisation (Schlenger et al., 2022). However, evidence also indicates that perceptions improve with increased experience, suggesting a potential habituation effect (Fiorentino et al., 2023). Digital services can give clients greater control and accessibility, particularly for those with limited access to in-person care (Mishna et al., 2022; Nordesjö et al., 2022; Owens et al., 2024). For younger clients, methods like smartphones and social media may be preferred, and some may find it easier to discuss sensitive topics online due to increased anonymity (Bolin & Sorbring, 2017; Denby et al., 2016; Mishna et al., 2022; Schlenger et al., 2022). Moreover, digital technologies enable enhanced multidisciplinary collaboration (Owens et al., 2024; Wheatley et al., 2021) and offer greater flexibility for balancing work and personal life (Schlenger et al., 2022).
However, certain challenges remain. During the pandemic, client relationships deteriorated due to limited communication and the absence of facial expressions, resulting in more goal-focused interactions with reduced emotional engagement (Nordesjö & Scaramuzzino, 2023; Owens et al., 2024; Schlenger et al., 2022; van de Luitgaarden & van der Tier, 2018). The increased anonymity has led to a loss of responsibility and respect among clients, which has been a major source of emotional distress among counsellors (Schlenger et al., 2022). Digital poverty, defined as the unavailability or unaffordability of essential digital resources, has also been a significant stressor, especially when technical limitations impair counselling quality (Fiorentino et al., 2023; Manthorpe et al., 2021; Schlenger et al., 2022). In the UK, remote social workers have struggled with blurred work-life boundaries, loneliness, and isolation, with insufficient social support substantially contributing to psychological distress (Manthorpe et al., 2021; Mishna et al., 2022; Owens et al., 2024). Despite the evidence, research remains especially scarce on how online counselling alters the traditional occupational risk assessment outlined by the GDA (Gemeinsame Deutsche Arbeitsschutzstrategie (GDA), 2018). To address this gap, we propose the following research question:
RQ2: How are OSH risks and resources, resulting from different working conditions, associated with various online counselling characteristics such as work location, and the frequency of online counselling and remote work among a sample of German counsellors?
This question follows established procedures for occupational risk assessments and explores the impact of online counselling on key occupational demands and resources. These include the work environment, information, workload, emotional burden, and work interruptions, as well as variety, collaboration, and social support. The quantitative analysis considers potential habituation effects by accounting for different levels of online counselling frequency. Additionally, OSH risks are examined across different work locations, and variations in remote work frequency are considered integral characteristics of online counselling.
While research on health outcomes in digital social care remains limited, studies on remote work suggest that digitalisation can offer benefits, including healthier lifestyles marked by improved eating habits and enhanced work-life balance due to reduced commuting and greater flexibility (Grzywacz et al., 2007; Henke et al., 2016; Junça et al., 2022). Conversely, musculoskeletal symptoms have increased as employees spend more time sitting and working on screens with fewer interruptions (Montreuil & Lippel, 2003). Moreover, the blurring of work-life boundaries can impede recovery and disrupt work-life balance, contributing to exhaustion and burnout (Berg-Beckhoff et al., 2017; Cijan et al., 2019; Wepfer et al., 2018). Nearly one-third of social care workers also reported higher stress levels following the implementation of online counselling during the pandemic (Nordesjö & Scaramuzzino, 2023). Remote work and digitalisation have been linked to increased fatigue, eye pain, inattention, and disrupted sleep quality due to prolonged screen use and intensified cognitive tasks (Christensen et al., 2019; Hilty et al., 2023; Mocci et al., 2001; Niu et al., 2021; Park et al., 2019). However, it remains unclear whether the effects observed in typical remote work fully translate to the social care sector, as online counselling may still involve office-based elements and in-person interactions with colleagues while only limiting direct client contact—unlike more isolated forms of telework. Therefore, this study aims to address this research gap with a third research question:
RQ3: How do different characteristics of online counselling (as outlined in RQ2) influence occupational health outcomes such as musculoskeletal symptoms, cognitive fatigue, and sleep disorders among a German sample of counsellors?
This study explores the impact of online counselling on musculoskeletal symptoms, cognitive fatigue, and sleep, while adjusting for job demands and resources, age, gender, and remote work frequency and location. By analysing these factors, the study aims to provide insights into how digital services influence employee well-being in social care, differentiating between online counselling conducted in remote versus office settings. The findings may inform decisions aimed at improving online counselling experiences and preventing adverse health outcomes for social care workers.
The remainder of the paper is organised as follows: Section 2 “Methodology” provides a detailed description of the methodological approach, followed by Section 3 “Results”, which outlines the findings of the quantitative analysis. Section 4 discusses these findings and contextualises them within the current literature. We conclude this paper with implications for practitioners, a discussion of the study's strengths and limitations, and suggestions for future research.
MethodologyThis section outlines the overall study design and methods used to investigate the prevalence of online counselling and its associations with work conditions and health outcomes. A quantitative research design utilising cross-sectional data was chosen, adhering to established practices in survey research (Mann, 2003). The subsequent sections provide details on the recruitment process, data collection, questionnaire development, measurements, and data analysis. An overview is provided in Fig. 1.

Methodology flowchart.
This report is based on data from a cross-sectional, questionnaire-based online survey conducted among social counsellors employed by a major German social welfare organisation. The survey also served as the first wave of a longitudinal study within a larger project on online counselling in Germany. Participants were recruited via an intra-organizational mailing list for employees interested in online counselling. The list included both experienced online counsellors and those interested in online counselling without practical experience. Approximately 5000 contacts were subscribed to this mailing list, which served as the reference population. The exact number of online counsellors remained unclear due to the decentralised organisational structure. Out of the approximately 5000 potential participants, 1049 completed the survey, representing a participation rate of about 20 %.
A web-based questionnaire was developed, incorporating several pre-existing standardised instruments. Electronic distribution of surveys is a well-established and effective method for reaching large populations, particularly advantageous given the welfare organisation's federal structure with offices across Germany (Bhattacherjee, 2019; Fowler, 2009; McLafferty, 2010). Feedback and background information from officials and employees of the organisation during the development process further enhanced the questionnaire's reliability and validity in the context of social care (Rattray & Jones, 2007). Information about the survey and a link to participate were sent to participants via email between April and June 2022, with regular reminders approximately every two weeks to enhance participation. The software used for data collection was SoSci Survey (Leiner, 2021).
The questionnaire included items on sociodemographic and work-related characteristics, such as gender, age, field of counselling, and counselling experience. Specific items addressed online counselling modalities, including video, email, chat, phone, and platform-based software. These covered participants’ experience, frequency of use, preferred formats, and perceptions of effectiveness. Additionally, participants were asked about their motivations for using online counselling, the extent and location of remote work, and the impact of the pandemic on counselling practices, with all questions tailored to online counselling workplaces. Working conditions were examined using the Short Questionnaire for Workplace Analysis (KFZA), a validated tool for psychosocial occupational risk assessment as outlined by the GDA (Appel et al., 2017; Gemeinsame Deutsche Arbeitsschutzstrategie (GDA), 2018; Prümper et al., 1995). This instrument measures factors such as variety, social support, collaboration, work environment, workload, and work interruptions on a 5-point Likert scale, ranging from “not at all” (1) to “completely agree” (5), with higher scores indicating a higher level of the respective demand or resource (Prümper et al., 1995). Information was inversely scaled, with scores ranging from (1) “to a very high degree” to (5) “to a very low degree”. Emotional burden was measured using the relevant sections of the German version of the Copenhagen Psychosocial Questionnaire (COPSOQ) (Lincke et al., 2021; Nübling, 2005). Outcome measures included stress and perceived general health, which were assessed with a 10-point Likert scale, as well as various psychosomatic symptoms (e.g., headaches, back pain, problems sleeping or concentrating), evaluated on a 5-point Likert scale ranging from 1 (never) to 5 (almost daily). These items were adapted from the psychosocial symptoms in non-clinical contexts questionnaire (Mohr & Müller, 2004). Furthermore, burnout was assessed using the respective items from the German version of the COPSOQ questionnaire (Lincke et al., 2021; Nübling et al., 2005).
MeasuresThis study examined sociodemographic variables and characteristics of online counselling, including age, gender, online counselling experience, field of counselling, and the proportion of online to all counselling sessions. Additionally, work location and remote work frequency were assessed, as these factors may influence job demands and health outcomes—for example, by reducing social support and increasing quantitative demands (Collins et al., 2016; Petcu et al., 2023). Age and gender were included as potential confounders given their associations with various psychosomatic health outcomes. For instance, previous research has indicated that women and older individuals are generally more prone to lower back pain than men and younger individuals (Beller et al., 2024).
The amount of online counselling was recategorised into three groups: “low” (0 %−10 %), “medium” (20 %−30 %), and “high” (40 % and more), to account for the small sample sizes in higher usage categories. The variable for the location of work, which initially included various combinations (e.g., “mobile work/office”), was simplified to “office,” “office combined with other locations,” and “other” due to varying and small group sizes in some categories. Similarly, counselling fields with fewer than 30 participants (4.0 %) were categorised as “other.” Additionally, the remote work frequency categories “daily” and “more than once a week” were combined into “more than once a week” to balance group sizes and improve interpretability. Occupational risk assessment results were reported for variety, social support, collaboration, work environment, information, workload, emotional burden, and work interruptions. Collaboration was further divided into a demand and resource aspect, with the former measured by the statement “my job demands collaboration with colleagues or clients,” and the latter derived from the combined statements “I can talk with work colleagues about work-related and private things,” and “I always get feedback from supervisors and colleagues” (Prümper et al., 1995). For the multivariate analysis, job resources were summarised as variety, social support, and collaboration (resource), while job demands were summarised as work environment, collaboration (demand), information, workload, emotional burden, and work interruption (Bakker & Demerouti, 2007).
Primary outcomes included musculoskeletal symptoms, cognitive fatigue, and sleep disorders, with individual psychosomatic symptoms combined into broader categories. Sleep disorders were measured using items asking, “Do you get tired quickly?”, “Do you experience difficulties sleeping?” and “Are you often tired during the day?”. Cognitive fatigue was assessed by combining the symptoms “headache”, “difficulties concentrating” and “getting tired quickly”. Finally, musculoskeletal symptoms consisted of “back pain”, “shoulder pain” and “neck pain”.
AnalysisData were analysed using SPSS Version 29 (IBM Corp, 2023). Descriptive statistics were computed using frequencies and proportions for categorical data, and means and standard deviations for continuous data, in line with established international standards (Mishra et al., 2019). Missing data were addressed through listwise deletion for each analysis, with the number of missing observations noted for each variable and analysis (Allison, 2009). To assess the impact of the amount of online counselling, we examined the risk assessment items including variety, collaboration (resource and demand), social support, work environment, information, workload, emotional burden, and work interruption, as well as the summary scores for demands and resources. The Kruskal-Wallis test was used to compare these measures across the three groups (low, medium, and high amounts of online counselling) and remote work characteristics. This rank-based, non-parametric test is widely recommended as a robust alternative to a one-way ANOVA when the assumption of normality is violated (Kruskal & Wallis, 1952; Ostertagová et al., 2014). The normality of continuous variables was assessed through visual inspection of histograms and Q-Q plots (Mishra et al., 2019). A chi-square analysis was conducted to test for significant associations between categorical data, including the three online counselling groups and the characteristics of remote work. The Chi-square test is a standard method for examining relationships among categorical variables and for determining whether the observed distribution of a variable significantly differs from the expected distribution (McHugh, 2013).
Multivariate regression analysis was then utilised to assess the impact of the amount of online counselling on musculoskeletal symptoms, cognitive fatigue, and sleep disorders, while simultaneously adjusting for continuous variables (job demands and resources) and categorical variables (location of work, frequency of remote work, age, and gender) (Aiken et al., 2012). For better interpretability, only summary variables were used for demands and resources in the adjusted model. A significance level of p < 0.05 was used for all analyses. Preliminary analyses using Shapiro-Wilk tests, scatter plots, and correlations confirmed that the assumptions of normality of residuals, linearity, multicollinearity, and homoscedasticity were met (Aiken et al., 2012; Schneider et al., 2010).
EthicsEthics approval was obtained from the ethics commission at the University of Lübeck under reference number AZ 21–388. Participation was entirely voluntary, and potential participants were informed about the study's aims and procedures before taking part. Written consent was required to begin the questionnaire. Participants received ongoing information throughout the study, and results were shared with both participants and relevant stakeholders within the welfare organisation. Data protection was ensured by using only de-identified data.
ResultsDigitalisation presents substantial challenges and opportunities for OSH, especially in high-stress occupations such as social counselling. In the following sections, we outline the results of our analysis, directly addressing our research questions and objectives. First, we provide an overview of the sample characteristics, exploring the current amount of online counselling within a large welfare organisation. Next, we display the occupational risks associated with online counselling and remote work using descriptive statistics. We then describe the relationship between online counselling, remote work, and occupational risks using the non-parametric Kruskal-Wallis test, followed by an overview of psychosomatic health outcomes. Finally, we discuss associations between online counselling and health outcomes using multiple regression analysis.
A total of N = 1049 participants were surveyed at T1. Missing data was especially notable in the psychosomatic health variables such as cognitive fatigue (with headache) and sleep disorders/problems, with 78 (7.44 %) and 76 (7.24 %) cases missing, respectively. Because listwise deletion was employed, multiple regression analyses were conducted only on participants with complete data for all included variables of the respective analysis. This resulted in further reductions in sample size, with up to 190 (18.11 %) cases missing in the regression analysis for cognitive fatigue. The final case numbers for each analysis are reported in Table 5.
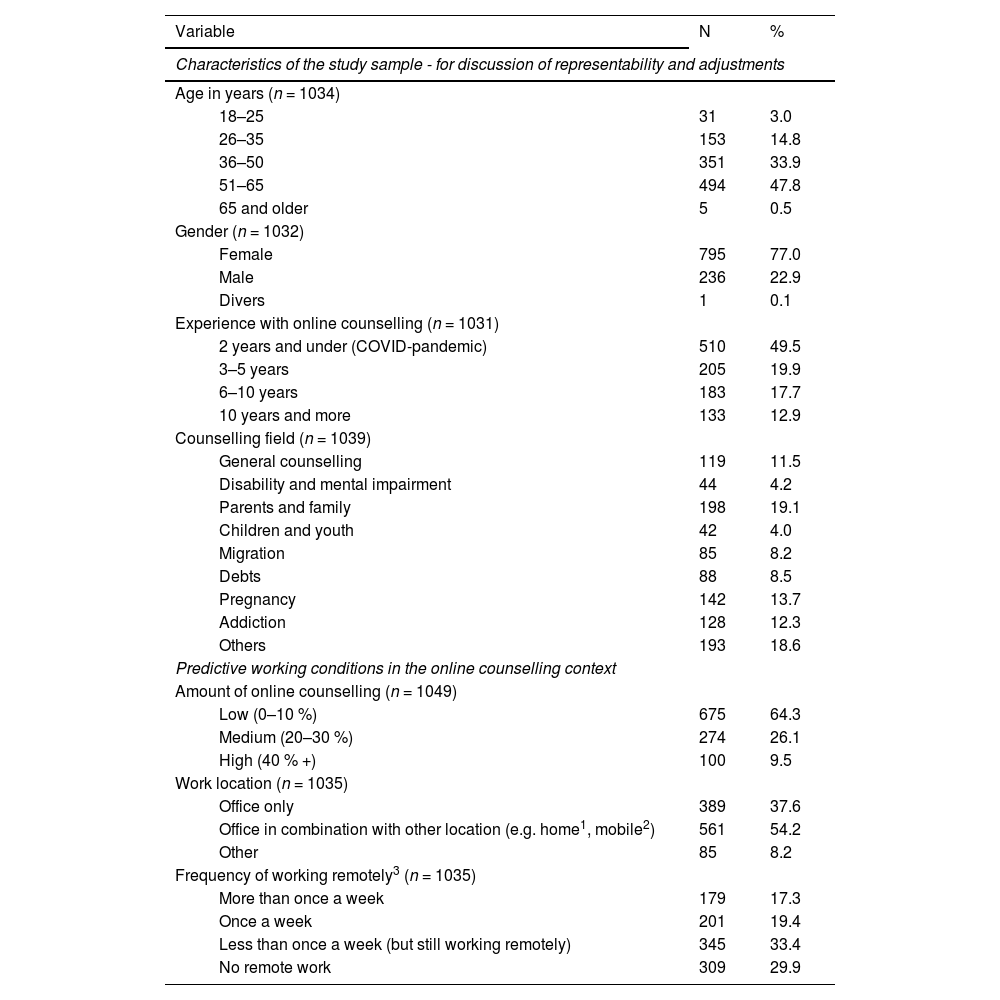
Participant profile and characteristicsTo facilitate understanding of the study population and enable thorough interpretation of the results, Table 1 provides an overview of the sociodemographic and work-related characteristics of our sample, including details pertinent to RQ1 (the amount of online counselling).
Descriptive analysis of the sociodemographic characteristics of the sample (n = 1049).
| Variable | N | % | |
|---|---|---|---|
| Characteristics of the study sample - for discussion of representability and adjustments | |||
| Age in years (n = 1034) | |||
| 18–25 | 31 | 3.0 | |
| 26–35 | 153 | 14.8 | |
| 36–50 | 351 | 33.9 | |
| 51–65 | 494 | 47.8 | |
| 65 and older | 5 | 0.5 | |
| Gender (n = 1032) | |||
| Female | 795 | 77.0 | |
| Male | 236 | 22.9 | |
| Divers | 1 | 0.1 | |
| Experience with online counselling (n = 1031) | |||
| 2 years and under (COVID-pandemic) | 510 | 49.5 | |
| 3–5 years | 205 | 19.9 | |
| 6–10 years | 183 | 17.7 | |
| 10 years and more | 133 | 12.9 | |
| Counselling field (n = 1039) | |||
| General counselling | 119 | 11.5 | |
| Disability and mental impairment | 44 | 4.2 | |
| Parents and family | 198 | 19.1 | |
| Children and youth | 42 | 4.0 | |
| Migration | 85 | 8.2 | |
| Debts | 88 | 8.5 | |
| Pregnancy | 142 | 13.7 | |
| Addiction | 128 | 12.3 | |
| Others | 193 | 18.6 | |
| Predictive working conditions in the online counselling context | |||
| Amount of online counselling (n = 1049) | |||
| Low (0–10 %) | 675 | 64.3 | |
| Medium (20–30 %) | 274 | 26.1 | |
| High (40 % +) | 100 | 9.5 | |
| Work location (n = 1035) | |||
| Office only | 389 | 37.6 | |
| Office in combination with other location (e.g. home1, mobile2) | 561 | 54.2 | |
| Other | 85 | 8.2 | |
| Frequency of working remotely3 (n = 1035) | |||
| More than once a week | 179 | 17.3 | |
| Once a week | 201 | 19.4 | |
| Less than once a week (but still working remotely) | 345 | 33.4 | |
| No remote work | 309 | 29.9 | |
Note.
Describes only the location of work (the home). Can include both “home office” as a type of regulated and planned work at home and “mobile work at home” which is not planned and under less legal regulations.
Approximately half of the participants were aged between 51 and 65 years, with only 3.0 % aged 18 to 25 years. The majority were female (77.0 %), and most reported limited experience with online counselling, with 49.5 % having 2 years or less experience, coinciding with the onset of the COVID-19 pandemic. Prominent counselling fields included general counselling (11.5 %), parents and family (19.1 %), pregnancy (13.7 %), and addiction (12.3 %). Addressing our first research question (RQ1), the amount of online counselling was generally low: 64.3 % of respondents reported that 10 % or less of the counselling was conducted online, while only 9.5 % reported high online counselling use. Most participants utilised a combination of office and remote work settings (54.2 %), with most working remotely less than once a week (33.4 %). When examining the distribution of remote work among the three online counselling groups, 44.5 % of the low-frequency group worked exclusively in the office compared to 30.3 % in the medium group and 12.0 % in the high user group (X2(4, N = 1035)=72.33, p < 0.001). Additionally, 39.4 % of the high user group reported working remotely more than once a week compared to only 14.9 % of the low user group (X2(6, N = 1034)=57.27, p < 0.001).
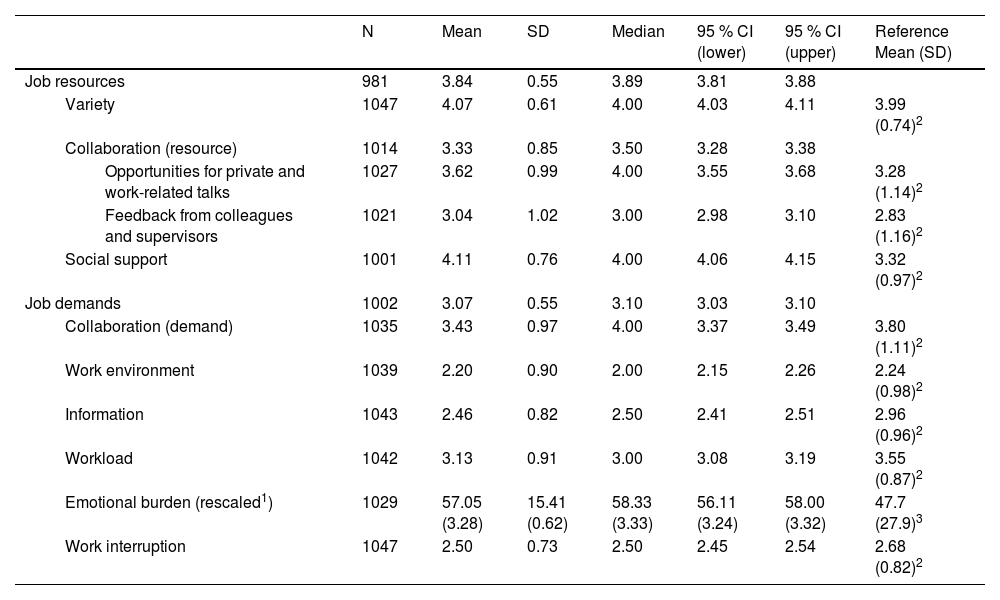
Occupational risk assessmentOur second research question (RQ2) focused on the working conditions and OSH risks associated with different online counselling groups and remote work characteristics, as determined through a systematic occupational risk assessment. First, we present the overall results for the full sample (Table 2). Then, Table 3 details the outcomes of a Kruskal-Wallis analysis, which identifies differences among online counselling groups. The results related to remote work characteristics are summarised in the text.
Occupational risk assessment according to the GDA guideline.
| N | Mean | SD | Median | 95 % CI (lower) | 95 % CI (upper) | Reference Mean (SD) | |||
|---|---|---|---|---|---|---|---|---|---|
| Job resources | 981 | 3.84 | 0.55 | 3.89 | 3.81 | 3.88 | |||
| Variety | 1047 | 4.07 | 0.61 | 4.00 | 4.03 | 4.11 | 3.99 (0.74)2 | ||
| Collaboration (resource) | 1014 | 3.33 | 0.85 | 3.50 | 3.28 | 3.38 | |||
| Opportunities for private and work-related talks | 1027 | 3.62 | 0.99 | 4.00 | 3.55 | 3.68 | 3.28 (1.14)2 | ||
| Feedback from colleagues and supervisors | 1021 | 3.04 | 1.02 | 3.00 | 2.98 | 3.10 | 2.83 (1.16)2 | ||
| Social support | 1001 | 4.11 | 0.76 | 4.00 | 4.06 | 4.15 | 3.32 (0.97)2 | ||
| Job demands | 1002 | 3.07 | 0.55 | 3.10 | 3.03 | 3.10 | |||
| Collaboration (demand) | 1035 | 3.43 | 0.97 | 4.00 | 3.37 | 3.49 | 3.80 (1.11)2 | ||
| Work environment | 1039 | 2.20 | 0.90 | 2.00 | 2.15 | 2.26 | 2.24 (0.98)2 | ||
| Information | 1043 | 2.46 | 0.82 | 2.50 | 2.41 | 2.51 | 2.96 (0.96)2 | ||
| Workload | 1042 | 3.13 | 0.91 | 3.00 | 3.08 | 3.19 | 3.55 (0.87)2 | ||
| Emotional burden (rescaled1) | 1029 | 57.05 (3.28) | 15.41 (0.62) | 58.33 (3.33) | 56.11 (3.24) | 58.00 (3.32) | 47.7 (27.9)3 | ||
| Work interruption | 1047 | 2.50 | 0.73 | 2.50 | 2.45 | 2.54 | 2.68 (0.82)2 | ||
Note.
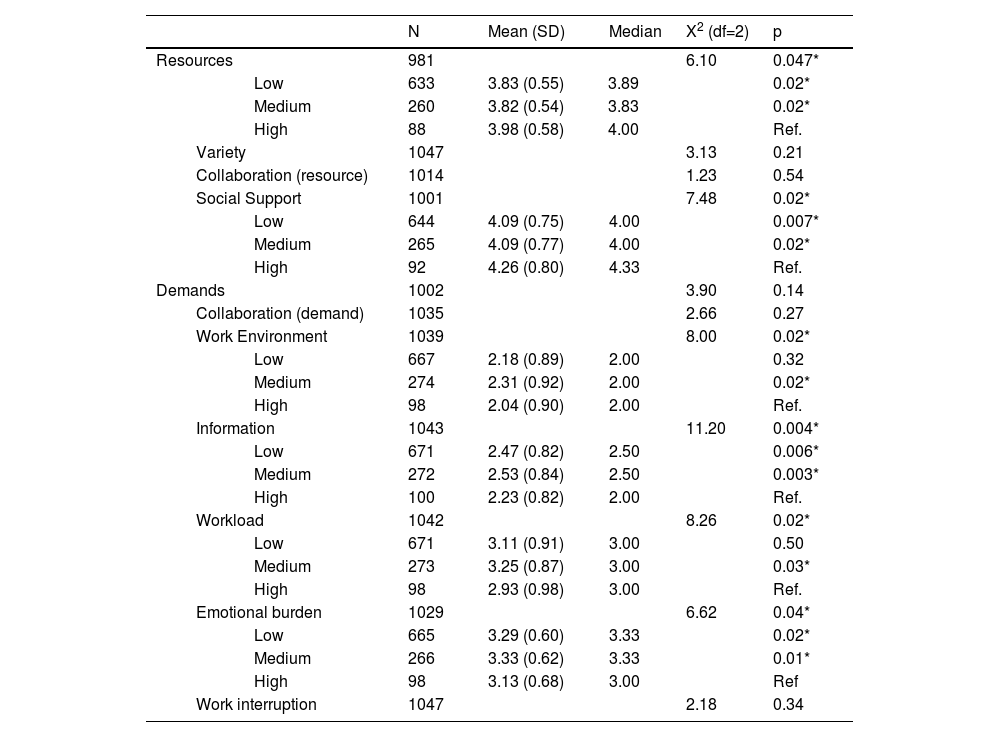
Occupational risk assessment distributed by amount of online counselling.
| N | Mean (SD) | Median | X2 (df=2) | p | ||||
|---|---|---|---|---|---|---|---|---|
| Resources | 981 | 6.10 | 0.047* | |||||
| Low | 633 | 3.83 (0.55) | 3.89 | 0.02* | ||||
| Medium | 260 | 3.82 (0.54) | 3.83 | 0.02* | ||||
| High | 88 | 3.98 (0.58) | 4.00 | Ref. | ||||
| Variety | 1047 | 3.13 | 0.21 | |||||
| Collaboration (resource) | 1014 | 1.23 | 0.54 | |||||
| Social Support | 1001 | 7.48 | 0.02* | |||||
| Low | 644 | 4.09 (0.75) | 4.00 | 0.007* | ||||
| Medium | 265 | 4.09 (0.77) | 4.00 | 0.02* | ||||
| High | 92 | 4.26 (0.80) | 4.33 | Ref. | ||||
| Demands | 1002 | 3.90 | 0.14 | |||||
| Collaboration (demand) | 1035 | 2.66 | 0.27 | |||||
| Work Environment | 1039 | 8.00 | 0.02* | |||||
| Low | 667 | 2.18 (0.89) | 2.00 | 0.32 | ||||
| Medium | 274 | 2.31 (0.92) | 2.00 | 0.02* | ||||
| High | 98 | 2.04 (0.90) | 2.00 | Ref. | ||||
| Information | 1043 | 11.20 | 0.004* | |||||
| Low | 671 | 2.47 (0.82) | 2.50 | 0.006* | ||||
| Medium | 272 | 2.53 (0.84) | 2.50 | 0.003* | ||||
| High | 100 | 2.23 (0.82) | 2.00 | Ref. | ||||
| Workload | 1042 | 8.26 | 0.02* | |||||
| Low | 671 | 3.11 (0.91) | 3.00 | 0.50 | ||||
| Medium | 273 | 3.25 (0.87) | 3.00 | 0.03* | ||||
| High | 98 | 2.93 (0.98) | 3.00 | Ref. | ||||
| Emotional burden | 1029 | 6.62 | 0.04* | |||||
| Low | 665 | 3.29 (0.60) | 3.33 | 0.02* | ||||
| Medium | 266 | 3.33 (0.62) | 3.33 | 0.01* | ||||
| High | 98 | 3.13 (0.68) | 3.00 | Ref | ||||
| Work interruption | 1047 | 2.18 | 0.34 | |||||
Note.
For the full sample, task variety and social support were high, with mean scores of 4.07 (95 % CI 4.03–4.11) and 4.11 (95 % CI 4.06–4.15), respectively. Among job demands, workload (3.13 (95 % CI 3.08–3.19)) and emotional burden (3.28 (95 % CI 3.24–3.32)) were particularly notable. Participants reported lower levels of organisational information and higher levels of emotional burden. Additionally, collaboration as a resource was higher compared to reference values, while collaboration as a demand was lower.
Table 3 presents the occupational risk assessment in relation to the amount of online counselling. Overall, the summary variable “job resources” differed significantly between online counselling groups (p = 0.047), with the high user group showing significantly higher averages than both the medium (p = 0.02) and low user groups (p = 0.02). In contrast, the summary variable “job demands” showed no significant difference across online counselling groups with p = 0.14. Some workplace factors differed across groups, with the high user group reporting significantly lower average burdens, particularly when compared to the medium user group. Among individual resource factors, only social support showed significant differences, with high users reporting higher average levels than both low and medium users (p = 0.007 and p = 0.02, respectively). For job demands, workload and work environment also differed significantly between the medium and high user groups, with the high user group experiencing a lower average burden. Additionally, burdens related to information and emotional demands were significantly higher in the low and medium user groups compared to the high user group.
Regarding remote work characteristics in the context of online counselling, significant associations were found between remote work frequency and workload (X2(3, N = 1028)=8.77, p = 0.03) and between remote work location and information burden (X2(2, N = 1031)=8.91, p = 0.01). Post-hoc analysis revealed that participants working remotely once a week reported a higher workload burden (3.28 (95 %CI 3.15–3.41)) compared to those who never worked remotely (3.05 (95 %CI 2.94–3.15)). Participants working in the office (2.48 (95 %CI 2.40–2.57)) or a combination of office and remote settings (2.48 (95 %CI 2.41–2.54)) reported higher information burden compared to those working at other locations (2.24 (95 %CI 2.05–2.43)).
Online counselling and occupational healthAs employees spend more time at work, effective OSH management becomes increasingly important for maintaining and improving health and well-being. Digitalisation has shown potential to mitigate adverse health effects by modifying working conditions and enhancing work-life balance. In this section, our third research question (RQ3) explores the role of online counselling in influencing various health outcomes, while adjusting for the effects of changing working conditions, remote work, and sociodemographic factors. To provide context, Table 4 presents an overview of the psychosomatic health outcomes in our sample. Finally, the results of the regression analyses are presented for each outcome, highlighting the specific contribution of online counselling (Table 5).
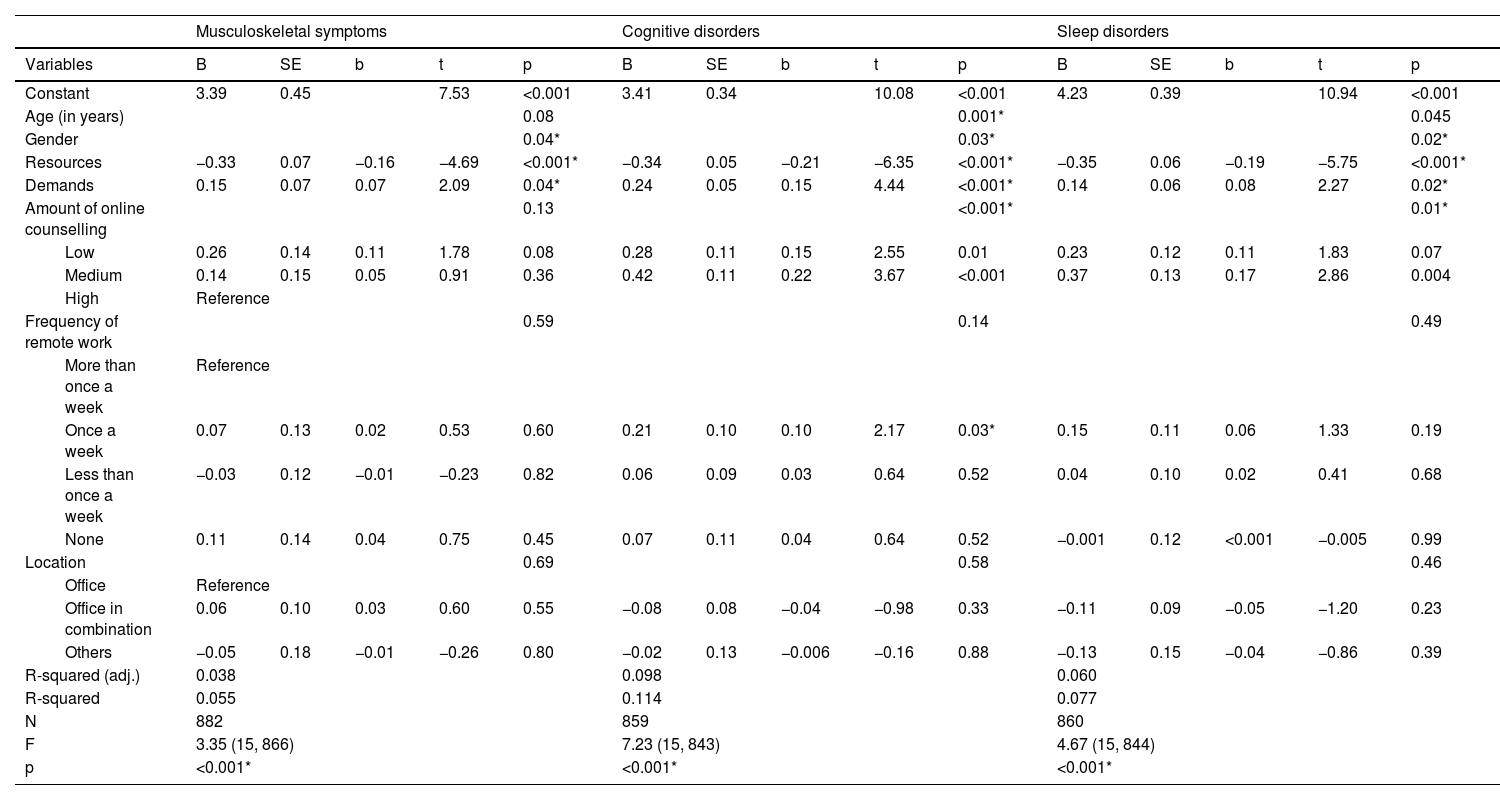
Multivariate Regression for psychosomatic health outcomes.
| Musculoskeletal symptoms | Cognitive disorders | Sleep disorders | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | B | SE | b | t | p | B | SE | b | t | p | B | SE | b | t | p | |
| Constant | 3.39 | 0.45 | 7.53 | <0.001 | 3.41 | 0.34 | 10.08 | <0.001 | 4.23 | 0.39 | 10.94 | <0.001 | ||||
| Age (in years) | 0.08 | 0.001* | 0.045 | |||||||||||||
| Gender | 0.04* | 0.03* | 0.02* | |||||||||||||
| Resources | −0.33 | 0.07 | −0.16 | −4.69 | <0.001* | −0.34 | 0.05 | −0.21 | −6.35 | <0.001* | −0.35 | 0.06 | −0.19 | −5.75 | <0.001* | |
| Demands | 0.15 | 0.07 | 0.07 | 2.09 | 0.04* | 0.24 | 0.05 | 0.15 | 4.44 | <0.001* | 0.14 | 0.06 | 0.08 | 2.27 | 0.02* | |
| Amount of online counselling | 0.13 | <0.001* | 0.01* | |||||||||||||
| Low | 0.26 | 0.14 | 0.11 | 1.78 | 0.08 | 0.28 | 0.11 | 0.15 | 2.55 | 0.01 | 0.23 | 0.12 | 0.11 | 1.83 | 0.07 | |
| Medium | 0.14 | 0.15 | 0.05 | 0.91 | 0.36 | 0.42 | 0.11 | 0.22 | 3.67 | <0.001 | 0.37 | 0.13 | 0.17 | 2.86 | 0.004 | |
| High | Reference | |||||||||||||||
| Frequency of remote work | 0.59 | 0.14 | 0.49 | |||||||||||||
| More than once a week | Reference | |||||||||||||||
| Once a week | 0.07 | 0.13 | 0.02 | 0.53 | 0.60 | 0.21 | 0.10 | 0.10 | 2.17 | 0.03* | 0.15 | 0.11 | 0.06 | 1.33 | 0.19 | |
| Less than once a week | −0.03 | 0.12 | −0.01 | −0.23 | 0.82 | 0.06 | 0.09 | 0.03 | 0.64 | 0.52 | 0.04 | 0.10 | 0.02 | 0.41 | 0.68 | |
| None | 0.11 | 0.14 | 0.04 | 0.75 | 0.45 | 0.07 | 0.11 | 0.04 | 0.64 | 0.52 | −0.001 | 0.12 | <0.001 | −0.005 | 0.99 | |
| Location | 0.69 | 0.58 | 0.46 | |||||||||||||
| Office | Reference | |||||||||||||||
| Office in combination | 0.06 | 0.10 | 0.03 | 0.60 | 0.55 | −0.08 | 0.08 | −0.04 | −0.98 | 0.33 | −0.11 | 0.09 | −0.05 | −1.20 | 0.23 | |
| Others | −0.05 | 0.18 | −0.01 | −0.26 | 0.80 | −0.02 | 0.13 | −0.006 | −0.16 | 0.88 | −0.13 | 0.15 | −0.04 | −0.86 | 0.39 | |
| R-squared (adj.) | 0.038 | 0.098 | 0.060 | |||||||||||||
| R-squared | 0.055 | 0.114 | 0.077 | |||||||||||||
| N | 882 | 859 | 860 | |||||||||||||
| F | 3.35 (15, 866) | 7.23 (15, 843) | 4.67 (15, 844) | |||||||||||||
| p | <0.001* | <0.001* | <0.001* | |||||||||||||
Psychosomatic health outcomes (Table 4) were generally in the mid-range, with symptom frequencies falling between approximately once a month (score=2) and once a week (score=3). Sleep disorders (2.89 (95 %CI 2.83–2.95) were slightly more frequent than musculoskeletal (2.79 (95 %CI 2.72–2.86)) and cognitive complaints (2.66 (95 %CI 2.61–2.72)).
To address RQ3, linear multiple regression was conducted to assess the influence of online counselling on health outcomes, while adjusting for job demands and resources, work location, remote work frequency, age, and gender.
Musculoskeletal symptomsTable 5 presents the results of the standard multiple regression for all psychosomatic health outcomes. Overall, the adjusted model explained R2(adj.)=0.038 of the variance in musculoskeletal symptoms (p < 0.001). Higher job resources were significantly associated with fewer musculoskeletal symptoms (b=−0.16, p < 0.001), while higher job demands were linked to an increase in symptoms (b = 0.07, p = 0.04). Additionally, gender was a significant predictor, with females reporting symptoms more frequently than males (b=−0.09, p = 0.01). No significant associations were found for the amount of online counselling, work location, or remote work frequency.
Cognitive fatigueFor cognitive fatigue, the adjusted model (Table 5) accounted for 9.8 % of the variance (R2(adj.)=0.098, p < 0.001). Higher job demands were significantly associated with increased cognitive fatigue (b = 0.15, p < 0.001), while higher job resources were linked to reduced fatigue (b=−0.21, p < 0.001). Regarding online counselling, participants in the high usage group reported significantly lower levels of cognitive fatigue compared to both the low (b = 0.15, p = 0.01) and medium (b = 0.22, p < 0.001) usage groups. Moreover, the medium group also exhibited significantly greater fatigue compared to the low usage group with b = 0.17, p = 0.03. Regarding remote work, participants working remotely more than once a week experienced significantly less fatigue compared to those working remotely up to once a week (b = 0.10, p = 0.03). Additionally, younger age was associated with higher cognitive fatigue, particularly in the comparison between the 18–25 age group and the 51–65 age group (b=−0.33, p = 0.004). Females also reported significantly higher fatigue than males (b=−0.07, p = 0.03). No significant association was found for work location.
SleepIn the adjusted model for sleep disorders presented in Table 5 (R2(adj.)=0.06, p < 0.001), higher job resources were associated with fewer sleep disorders (b=−0.19, <0.001), while higher job demands were linked to an increase in sleep complaints (b = 0.08, p = 0.02). All lower-usage online counselling groups reported more frequent sleep disorders compared to the high-usage group. However, statistically significant differences were observed only between the medium and high-usage groups (b = 0.17, p = 0.004), with the high-usage group reporting significantly fewer sleep disorders. Additionally, the 18–25 age group was significantly associated with more sleep disorders compared to all other age groups—for example, compared to the 51–65 group (b=−0.31, p = 0.009). Females also reported significantly higher levels of sleep disorders than males (b=−0.09, p = 0.007). No significant associations were found between sleep disorders and either work location or remote work frequency.
This study examined the relationship between online counselling, occupational risks, and psychosomatic health outcomes, addressing the research questions outlined in Section 1.2. Overall, our findings indicate that online counselling remains relatively uncommon among social counsellors in one of Germany's largest welfare organisations, with most participants using it infrequently (RQ1). Regarding RQ2, the occupational risk assessment revealed significant differences in job resources among the online counselling groups, with high-frequency users reporting greater resources—particularly in terms of social support. However, no significant differences in overall job demands were found between groups. Similarly, remote work characteristics showed no significant associations with job demands or resources. Addressing RQ3, the findings showed that cognitive fatigue and sleep disorders were more prevalent among low- and medium-frequency users compared to high-frequency users, suggesting a potential protective or habituation effect of frequent online counselling. In contrast, musculoskeletal symptoms were primarily influenced by job demands and resources rather than the frequency of online counselling. Furthermore, younger age and female gender were associated with a higher burden of psychosomatic symptoms. A visual representation of these relationships is provided in Fig. 2 to illustrate the key findings more clearly.

Overview of results and conceptual model.
This study examined the prevalence of online counselling in social care, the occupational risk factors associated with it, and its effects on psychosomatic health outcomes. Despite increased uptake during the pandemic (Stieler et al., 2022), the use of online counselling remained relatively low by 2022 (RQ1). This trend reflects the broader return to office-based work in Germany, where the weekly rate of remote work declined from 36 % to 28 % as the pandemic progressed (Böhm & Schepp, 2024). Although digitalisation efforts surged at the onset of the pandemic, many organisations later scaled back these initiatives (Böhm & Schepp, 2024). In the health and social care sector, the sustainability of online services largely depends on organisational preparedness, including motivation and investment (Caprioli et al., 2023; Kateb et al., 2022). However, the rapid and forced digital transitions triggered by the pandemic often bypassed the preferred gradual implementation process (Candi et al., 2013; Kateb et al., 2022; Kohli & Melville, 2019). For example, in the Netherlands, social welfare organisations without pre-existing online services encountered significant resistance, with many counsellors reverting to in-person sessions—even in cases where organisations were motivated, financial and structural barriers posed major challenges (Kateb et al., 2022). The organisation in this study has offered online counselling since 2006 and provided extensive educational resources, which have been shown to support sustained adoption in other contexts (Deutscher Caritasverband eV, 2020a, 2020b; Kateb et al., 2022). However, its federal structure means that service uptake may vary across counselling locations depending on local leadership and resource availability—factors that could partly explain the low prevalence observed in response to our first research question.
This study is among the first to systematically assess occupational risks among online counsellors using the GDA guidelines, as examined in RQ2. Compared to other occupational groups in Germany, counsellors reported higher emotional demands and collaboration requirements, reflecting the inherently relational and emotionally intensive nature of social care work (Prümper et al., 1995; Rollins, 2020). The Kruskal-Wallis test revealed that a higher frequency of online counselling was associated with more favourable working conditions, particularly when comparing medium- and high-frequency users, as evidenced by differences in perceived workload and work environment. Similarly, participants working remotely once a week reported a higher workload than those who never worked remotely, while this effect was not observed in those working remotely more frequently. This may suggest a habituation effect, whereby increased exposure to digital work improves perception, confidence, and resource utilisation (Fiorentino et al., 2023; Nordesjö & Scaramuzzino, 2023). For example, transitioning to online counselling may initially increase workload due to additional IT-related responsibilities; however, as digital skills improve, these challenges likely diminish, making online counselling more manageable and effective (Carlson et al., 2017; Scholze & Hecker, 2023). Individual factors and personality traits may also influence digital adoption and perceived working conditions. Higher self-efficacy, for instance, has been linked to greater uptake of information and communication technology (ICT) among teachers (Hatlevik & Hatlevik, 2018) and to lower perceived workload among social workers (Nowosad, 2023). Similarly, teleworkers with lower sociability and higher autonomy needs have been shown to perform better in remote settings (O'Neill et al., 2009). Work environment challenges, such as inadequate IT infrastructure, are common in underfunded sectors like social care (Fiorentino et al., 2023; Manthorpe et al., 2021). However, strong organisational support and effective employee feedback mechanisms can help mitigate these issues by securing financial resources and improving IT systems—thereby optimising working conditions and encouraging the adoption of digital tools (Fiorentino et al., 2023; Kateb et al., 2022). Contrary to previous research on telework, which suggests that digitalisation may enhance collaboration while reducing social support and the quality of interpersonal contact (Gajendran & Harrison, 2007; Schlenger et al., 2022; Wöhrmann & Ebner, 2021), our study found a positive association between frequent online counselling and higher levels of perceived social support. This distinction may be due to the nature of online counselling, which—unlike many forms of telework—often still includes office-based elements and regular interaction with colleagues, with only client communication occurring digitally. In our sample, 37.6 % of employees were fully office-based, and over 60 % worked remotely less than once a week, reinforcing this difference.
Our study examined occupational health as reflected in psychosomatic health outcomes (RQ3), drawing comparisons with telework research due to the limited number of studies specifically focused on online counselling. The model fit for musculoskeletal symptoms was relatively low, suggesting that other unmeasured factors—such as physical activity during leisure time—may play a role (Dang et al., 2024). In contrast, cognitive fatigue and sleep disorders were significantly associated with online counselling, with high-frequency users reporting fewer symptoms and a peak observed among medium-frequency users. More frequent remote work was linked to lower cognitive fatigue, although it showed no significant effect on sleep. These findings suggest that the use of digital tools may impact cognitive health more directly than physical symptoms. Symptom increases during the transition to online counselling may be attributed to prolonged screen exposure, which has been linked to eye strain, headaches, and fatigue (Hilty et al., 2022; Roy et al., 2024). A potential habituation effect is supported by research showing that frequent remote workers experience less technostress and adapt more effectively to technology-induced fatigue compared to those who work remotely less often (Borle et al., 2021; Singh et al., 2022; Suh & Lee, 2017). In addition to direct effects, online counselling may also influence health outcomes indirectly through changes in working conditions—an area that warrants further investigation. For example, Wöhrmann and Ebner (2021) used path analysis to examine psychosomatic outcomes in white-collar teleworkers and explained 19 % of the variance—only slightly higher than the variance explained by our regression model (Wöhrmann & Ebner, 2021). Their study found no direct link between telework and health complaints but identified indirect effects through changes in boundaryless working hours, time pressure, co-worker relations, and working time control (Wöhrmann & Ebner, 2021). Prior research on work location and psychosomatic health has yielded mixed results. Some studies have linked working from home to prolonged screen time and videoconferencing fatigue (Bennett et al., 2021; McDowell et al., 2020), while others have reported benefits such as longer sleep duration (Massar et al., 2023; Wöhrmann et al., 2020). Our study found no significant effects of work location. Although previous research suggests better outcomes for regulated telework compared to unregulated mobile work, this distinction was not evident in our findings (Massar et al., 2023; Wöhrmann et al., 2020). Given the small sample sizes across different work locations and the lack of differentiation in remote work regulations within our dataset, further research is needed to explore the role of remote work in the social care sector.
Implications for practitionersImproving the prevalence and working conditions of online counselling requires a holistic approach that addresses individual, structural, and organisational factors (Hilty et al., 2022). Counsellors need to develop digital competencies, including effective digital communication skills and proficiency in using secure, user-friendly platforms that comply with data protection regulations. They must also be sensitive to clients’ diverse digital needs. Vulnerable populations—such as the elderly or those with limited technological access—may require additional support or hybrid service models. Therefore, assessing clients’ digital literacy and willingness to engage in online counselling is essential to ensure equitable access. Given the increased burden during the transition to digital services, ongoing guidance and support throughout the digitisation process are critical.
Beyond individual adaptation, organisations must establish clear guidelines for digital counselling, including training programs, quality assurance measures, and strategies to address challenges such as screen fatigue and digital exclusion. Recognising online counselling as a core service rather than a supplementary offering can increase its adoption and justify greater financial investments to address structural barriers, such as inadequate IT infrastructure. Our findings further emphasise the importance of implementing standardised OSH management systems, such as those outlined by the GDA and ISO 45,001, to identify and mitigate potential occupational risks. By proactively addressing these factors, both counsellors and organisations can enhance the long-term sustainability, accessibility, and effectiveness of digital counselling services.
Limitations and recommendationsThis study benefits from a large sample size, which enhances statistical power and supports both the representativeness and generalisability of findings within the German social welfare context. Comparisons with organisational employee data indicate that the sample is representative in terms of gender and counselling field. To our knowledge, this is the first study to evaluate the impact of online counselling on OSH using a standardised risk assessment tool, thereby increasing the validity and applicability of the findings. Additionally, by distinguishing between remote work location, frequency, and the extent of online counselling, our approach offers nuanced insights into the impact of digitalisation on social care—an approach future research should continue to develop and extend to other digital service settings.
However, the study's cross-sectional design limits the ability to draw causal inferences. It remains possible that working conditions influence the uptake of online counselling or that a more complex, bidirectional relationship exists—despite the theoretical assumptions made in this study. Future research should employ longitudinal designs to better assess causal relationships over time. Moreover, the use of convenience sampling and voluntary survey participation may have introduced self-selection bias, and reliance on self-reported questionnaires increases the risk of subjective assessments and reporting bias. Although the overall sample size was large, the subgroup of high online counselling users (>40 % of counselling conducted online) was relatively small, limiting the scope for more detailed subgroup analyses. Further research focusing specifically on this group, and incorporating additional factors such as autonomy and work-life balance, could provide deeper insights. Finally, future studies should investigate potential moderation effects to better understand how to maximise the benefits and minimise the drawbacks of online counselling and remote work in the social care sector.
ConclusionDespite its potential benefits, online counselling remains underutilised in Germany, with only 9.5 % of social counsellors in a large welfare organisation using it frequently (defined as >40 % of counselling conducted online). Our findings support the hypothesis that OSH risks and outcomes may vary depending on the extent of online counselling use, suggesting that occupational risk assessments should be tailored to the level of digitalisation within an institution. Specifically, our assessment revealed that high-frequency users experienced significantly lower demands—such as quantitative workload—compared to medium users during the transitional usage range (20 %–30 % online counselling, p = 0.03). Furthermore, regression analyses showed that high levels of online counselling were associated with reduced cognitive fatigue (p < 0.001) and fewer sleep disorders (p = 0.01). These results may reflect a habituation effect and underscore the importance of providing targeted support during digital transitions. The findings also suggest that employees demonstrate varying levels of “digital maturity,” and, depending on organisational goals, should be trained to meet defined digital standards before engaging in online counselling. Since barriers to digitalisation can arise from individual, structural, or organisational factors, a holistic approach is essential. Future research should explore moderating factors such as autonomy, work-life balance, and individual predispositions to maximise the benefits of digitalisation in social care.
DisclosureIn accordance with Elsevier's Generative AI Policies for Journals, parts of this manuscript have been edited with the assistance of generative AI tools, such as GPT-4, to enhance readability and language clarity. AI tools have not been used in other parts of the research process. The editing process was conducted under human oversight, with all changes reviewed and approved by the authors. All intellectual contributions, content, and interpretations remain the sole responsibility of the authors.
FundingThis work was supported by the Employer's Liability Insurance Association for Health Services and Welfare Care (BGW) [grant number 1551] as institutional funding for the Institute of Occupational Medicine, Prevention and Workplace Health Management, Medical Faculty, University of Luebeck. The funding source had no involvement in the study design, collection, analysis or interpretation of data, in the writing of the report and in the decision to submit the article for publication.
CRediT authorship contribution statementEva Gnugesser: Writing – review & editing, Writing – original draft, Formal analysis, Data curation. Marlies Jöllenbeck: Project administration, Methodology, Funding acquisition, Conceptualization. Wiebke Schlenger: Validation, Software, Conceptualization. Elke Ochsmann: Writing – review & editing, Writing – original draft, Supervision.
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:
M. Jöllenbeck was affiliated with the Institute of Occupational Medicine, Prevention and Workplace Health Management, Medical Faculty, University of Luebeck at the time of her contribution to the project with no post or present affiliation to the funding partner, the Employer's Liability Insurance Association for Health Services and Welfare Care (BGW). After finishing her part in the project, she began working with the BGW but had no further involvement in the project thereafter.
We would like to thank our collaboration partner Caritas with special recognition for those who participated in the study. We also appreciate the efforts of Ms. Schellack and Ms. Grosse who facilitated the connection with Caritas and the funding partner, and managed the project in these institutions. Finally, we would like to acknowledge the support of the DICARO Steuerkreis who provided oversight and guidance throughout the project.