







To report the impact of the COVID-19 pandemic on the activity of nurses working on an inflammatory bowel disease (IBD) unit and to identify reasons for telehealth care and its relationship to certain characteristics.
BackgroundThe COVID-19 pandemic had led to an increase in demand for remote care in patients with inflammatory bowel disease who require monitoring and frequent access to health services.
Design – methodsA retrospective study of all activity (in person and by phone call or email) done on the unit during the acute phase of the pandemic at a reference hospital in Spain. Numbers of activities done by nurses, reasons for telehealth care and sociodemographic and clinical data were collected. Statistical analysis was performed using frequency, chi-squared and analysis of variance tests.
ResultsA total of 1095 activities for 561 patients who received care were reported. Among them, 1042 (95.2%) were telemedicine activities, amounting to a 47.3% increase over the prior year. COVID-19-related activities numbered 588 (59.5%). Consultations due to disease flare-up numbered 134 (13.7%), representing a 145% increase compared to 2019. Significant differences were found between reasons for using telemedicine and diagnosis, occupational status, contact week and treatment.
ConclusionThe acute phase of the pandemic has changed the activity managed by the nursing staff on the unit. Identifying and analysing these changes has yielded valuable information to achieve more efficient management and better care quality for patients in special situations.
Describir el impacto de la pandemia por COVID-19 en la actividad de la enfermera, en enfermedad inflamatoria intestinal (EII) de la unidad, e identificar las razones de la asistencia telemática y la relación con las variables recogidas.
AntecedentesLa pandemia de COVID-19 ha dado lugar a un aumento en la demanda de atención remota en pacientes con EII que requieren un seguimiento y un acceso frecuente a los servicios de salud.
Diseño y métodosEstudio retrospectivo de toda la actividad (presencia, llamada telefónica o correo electrónico), realizado en la unidad durante la fase aguda de la pandemia, en un hospital de referencia en España. Se recogió el número de actividades llevadas a cabo por la enfermera, motivo de asistencia telemática y datos sociodemográficos y clínicos. El análisis estadístico se realizó utilizando la prueba de frecuencia, χ2 y el análisis de varianza.
ResultadosFueron registradas 1.095 actividades por 561 pacientes atendidos, siendo 1.042 (95,2%) actividades de telemedicina, lo que supuso un incremento del 47,3% con respecto al año anterior. Las demandas relacionadas con COVID-19 fueron 588 (59,5%). Por otro lado, 134 (13,7%) fueron consultas por brote de su enfermedad, un 145% más que en 2019. Se han encontrado diferencias significativas entre los motivos del uso de la telemedicina y el diagnóstico, la situación laboral, la semana en que se realizó el contacto y el tratamiento.
ConclusiónLa fase aguda de la pandemia ha cambiado la actividad gestionada por enfermería en la unidad. Identificar y analizar estos cambios nos ha proporcionado información para conseguir una gestión más eficiente y de calidad al cuidado de los pacientes en situaciones excepcionales.
On January 7, 2020, a new SARS-CoV-2 was identified in China.1 The disease associated with this virus was named coronavirus disease 2019 (COVID-19) which subsequently spread rapidly,2 and was declared a pandemic by the World Health Organization (WHO) on March 11, 2020.3
The COVID-19 pandemic is an unprecedented global challenge both at an economic level and on the resilience of health systems worldwide. Strategic plans have been created, focused on the emerging care of COVID-19. However, it seems that the approach to patients with chronic conditions has been left to the experts of each specialty. Specifically, there are several recommendations on the management of Inflammatory Bowel Disease (IBD) during the current COVID-19 pandemic.4–6
IBD is defined as a group of chronic inflammatory disorders of unknown cause affecting the gastrointestinal tract, comprising two diseases: Crohn's disease (CD) and Ulcerative Colitis (UC).7 It is characterized by a chronic course that usually alternates periods of active disease (relapse) with periods of remission, with potential complications that often require urgent or less preferential care. IBD affects mainly young people from a productive or formative age, and has an impact on their quality of life8; all this increases the use of health resources at an economic cost, and also has a great impact on the labor force.9
The Crohn-Colitis Care Unit (UACC) of the Hospital Universitari de la Vall d’Hebron in Barcelona follows a model of comprehensive patient-centered care through face-to-face and distance care. It is the Advanced IBD Nurse (AIN) who takes an outstanding leadership role in telehealth assistance (TA), known as telemedicine, due to their clinical profile and professional skills.10,11
As in other countries, this pandemic has had an impact on material and human resources of the UACC and has resulted in an increase of telemedicine provided to IBD patients.12–16 This can probably be related to patient uncertainty, fear of treatments, health system collapse and home-stay, among other reasons. We think it is compulsory to analyze the type of activities carried out by the AIN, in order to improve the care of our patients in exceptional situations such as those we have experienced. Patients with IBD require continuity of care because of the chronic nature of their disease and need to be well-informed.13,17 Telemedicine seems to be the best strategy for patient care in special situations because it provides flexibility and immediacy, and promotes patient autonomy.
The objective of the study is to describe the impact of the pandemic on the activity managed by the UACC nurse during the acute phase of the pandemic produced by COVID-19, comparing this activity with the same period from the previous year. As secondary objectives, we want to examine the reasons for remote care of UACC patients during the acute phase of the pandemic and assess predictors of the reason for consultation according to sociodemographics as well as the clinical characteristics of patients.
Patients and methodsInstitutional setting and study populationObservational, descriptive and retrospective study. The research was carried out at the UACC of the Hospital Universitari Vall d’Hebron, a third-level reference hospital, located in Barcelona (Spain) and affiliated with the Public Health Service of Catalonia. The health care team consists of two Advanced IBD Nurses and five gastroenterologists, which during the pandemic were reduced to one AIN and two gastroenterologists. The UACC's medical and nursing care services remained unchanged throughout the period under review. An informative email was also sent to all patients linked to the unit, providing them with prevention advice and reporting the conversion of UACC's face-to-face medical activity into telehealth assistance during the pandemic period. The AIN's protocolized interventions were adapted, focusing our attention on patient education and emotional support to patients in situations of fear, worry or anxiety.
Telemedicine encompasses telephone service (automatic answering system from 4PM to 9AM) and email. Accredited as a unit of excellence.18 UACC currently treats 2500 IBD patients, who have been chosen as the study population.
The analyzed sample consisted in all activities (face-to-face, by telephone or e-mail) made to the UACC during the acute phase of the COVID-19 pandemic in Spain (from 2 March to 17 April 2020). Due to the descriptive and retrospective nature of the study, no formal sample calculation was performed. All records that fulfilled the inclusion criterion, defined as any priming performed by patients or family members>14 years, have been included. Any contact made by a person who was not recorded in our general database was excluded.
Ethical considerations of the studyThis study has been approved by the Ethics Committee for Clinical Research of the Hospital Universitari Vall d’Hebron (reference 308/20). Throughout the investigation process, ethical and data protection protocols related to anonymity and data confidentiality were complied with.
Data collectionPatient data was exempted from a database, which includes patients treated at the UACC; and activity data was collected in a coded method from the electronic medical history of the patient.
All activities were reviewed either face-to-face, via telephone or email during the study period. Four of the authors (EN, AI, IB, JA, SL) independently analyzed the records, and those activities whose activity type information was not complete were excluded.
The activity managed by the AIN was defined into three categories: face-to-face, telephone and email. In addition, telemedicine was defined as any service through which IBD patients can consult health professionals via telephone or electronic means.19
The reasons for telemedicine were classified into 4 categories: I “COVID-19” (resolution of doubts on the impact of COVID-19 and IBD/health advice to prevent infection, explaining and reinforcing the recommendations generated by WHO and the Spanish Ministry of Health/guarantee the adherence to basic medications by working on risk-benefit communication/compassion and emotion management), II “Administrative visits COVID-19” (Resolution of doubts on the protocol changes of the follow-up of patients with biological treatment, picking up hospital medication and advising the change of location of the daily clinic for infusion treatments due to pandemic reorganization/reports to justify trips to the Hospital for administration of treatments/voluntary changes of patients), III “Disease relapse” (presentation of digestive symptoms) and IV “Others” (test results, appointments, prescription, updates, etc.).
Sociodemographic data (age, gender and employment situation) and clinical data (clinical diagnosis and treatments) were collected.
STROBE guidelines for cross-sectional studies were followed in reporting this study.
Statistical analysisA descriptive analysis of the data was performed using frequencies and percentages, to present the categorical data and the mean and standard deviation for quantitative variables. To contextualize the results obtained, they were compared to the activity carried out by the AIN in the UACC in the same period from March 2 to April 17, 2019.
A comparative analysis was performed to detect significant differences between unit groups by testing chi-square for categorical variables and for quantitative variables, variance analysis (ANOVA) was used. A type I error of 0.05 was considered.
SPSS software package version 21.0 (SPSS, Chicago IL) has been used for statistical analysis.
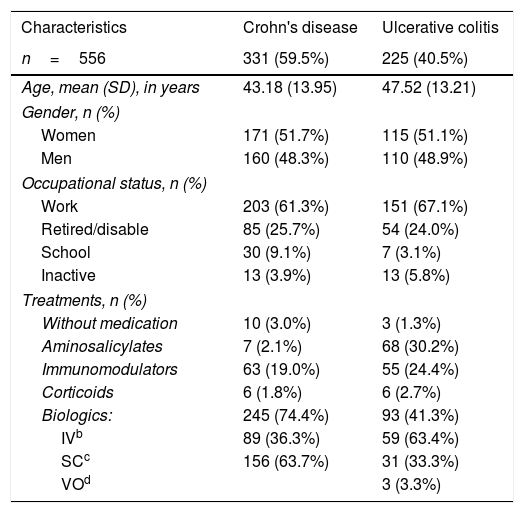
ResultsDuring the 7 weeks of study, 1095 activities were generated by 561 patients (22% of the study population), 5 of whom did not have IBD and were excluded from the analysis. The description of the demographics and clinical characteristics can be found in Table 1. 331 (59.9%) were patients with CD. Gender distribution is similar, with 286 (51.4%) women. Patients with an active working situation were 354, which accounted for 63.7% of the sample. Regarding medication, it should be noted that 468 (84, 2%) receive immunosuppressive or immunomodulatory treatments. During the inclusion period, 5 patients in our sample had confirmed diagnoses of COVID-19 by the PCR test.
Description of demographic and clinical characteristics of patients who contacted Advanced IBD Nurse from UACCa.
| Characteristics | Crohn's disease | Ulcerative colitis |
|---|---|---|
| n=556 | 331 (59.5%) | 225 (40.5%) |
| Age, mean (SD), in years | 43.18 (13.95) | 47.52 (13.21) |
| Gender, n (%) | ||
| Women | 171 (51.7%) | 115 (51.1%) |
| Men | 160 (48.3%) | 110 (48.9%) |
| Occupational status, n (%) | ||
| Work | 203 (61.3%) | 151 (67.1%) |
| Retired/disable | 85 (25.7%) | 54 (24.0%) |
| School | 30 (9.1%) | 7 (3.1%) |
| Inactive | 13 (3.9%) | 13 (5.8%) |
| Treatments, n (%) | ||
| Without medication | 10 (3.0%) | 3 (1.3%) |
| Aminosalicylates | 7 (2.1%) | 68 (30.2%) |
| Immunomodulators | 63 (19.0%) | 55 (24.4%) |
| Corticoids | 6 (1.8%) | 6 (2.7%) |
| Biologics: | 245 (74.4%) | 93 (41.3%) |
| IVb | 89 (36.3%) | 59 (63.4%) |
| SCc | 156 (63.7%) | 31 (33.3%) |
| VOd | 3 (3.3%) | |
aUnidad Atención Crohn y Colitis ulcerosa.
bIntravenous.
cSubcutaneus.
dOral.
Regarding the type of activity managed by the AIN, 1042 (95.2%) were telemedicine activities, and 53 (4.8%) were face-to-face at the UACC. In 2019, 743 activities were conducted from 409 patients (17% of the study population), of which 614 (82.6%) were telemedicine contacts and 129 (17.4%) being face-to-face at the UACC (Fig. 1). Therefore, in the same period this year, an increase of 352 activities in total has been recorded, which is 47.3% more than 2019. Specifically, telemedicine has grown by 70% whereas face-to-face activity has decreased by 41%.

The evolution of activity in the acute period of the pandemic can be observed in Fig. 2, reaching its peak during the 3rd week (16–21 March) with 238 (21.7%) activities, followed in number by the 2nd week (9–15 March) with 179 (16.3%).

The reasons for the 1042 telemedicine activities are described in Fig. 3. COVID-19 (I–II) related activities numbered at 588, which meant 59.5% from total activity including 17 TA activities performed by the 5 patients diagnosed with COVID-19, and 42 TA for symptoms compatible with COVID-19 without confirmed diagnosis. 299 (27.3%) activities were placed under the category of others (IV).

With cases related to COVID-19, 5 patients (3 men and 2 women) were diagnosed with the novel coronavirus, 3 of whom required hospitalization. 4 patients had CD, and the other UC. 3 CD patients were under biological anti-TNF treatment, and the patient with UC was taking aminosalicylates.
29 patients contacted the illness, as they had respiratory symptoms, 17 (58.6%) were women, 17 (58.6%) with CD and 18 (63.1%) were under biological treatment. They were referred to primary care, with no confirmation of COVID-19 at the end of the study.
Relapse symptoms generated 134 (13.7%) activities from 86 patients. From this group, 55 (64%) had ulcerative colitis, 54 (62.8%) were women, 44 (51.2%) were working. Referring to treatment, 37 (43%) carried biologics and 25 (29.1%) base aminosalicylates. Whereas in 2019 there were only 35 related activities due to relapse, representing 145% more activity for this reason.
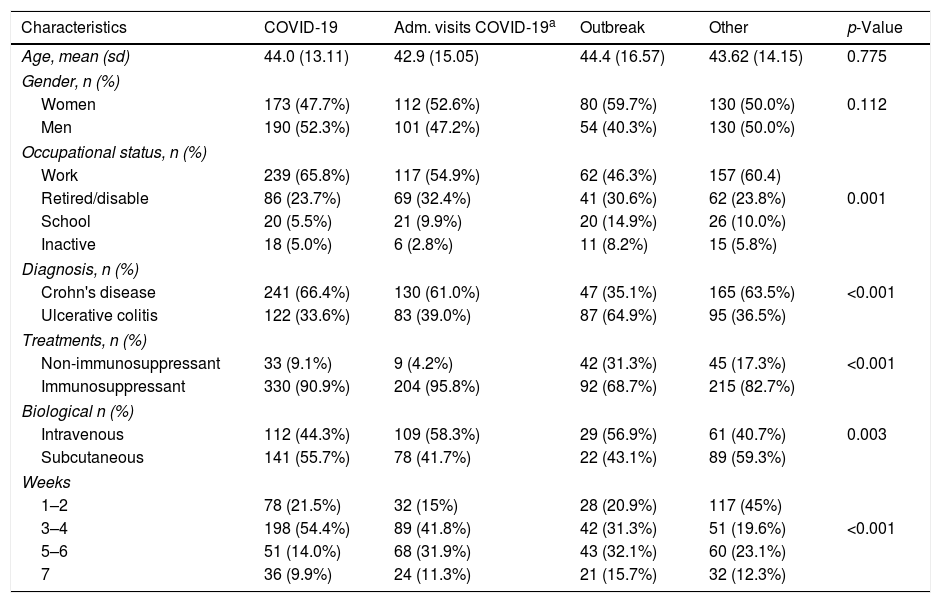
In the study, 970 of the 1042 telemedicine activities have been analyzed, and 72 have not due to missing data. The analysis of contact reasons has demonstrated that differences have been found in relation to employment situation, diagnosis, week of contact and treatment. Differences have also been found in the test carried out to assess the differences between biological treatments (not so with the variables of age and gender, Table 2).
Relationship of sociodemographic and clinical characteristics with the reason for consultation (n=970).
| Characteristics | COVID-19 | Adm. visits COVID-19a | Outbreak | Other | p-Value |
|---|---|---|---|---|---|
| Age, mean (sd) | 44.0 (13.11) | 42.9 (15.05) | 44.4 (16.57) | 43.62 (14.15) | 0.775 |
| Gender, n (%) | |||||
| Women | 173 (47.7%) | 112 (52.6%) | 80 (59.7%) | 130 (50.0%) | 0.112 |
| Men | 190 (52.3%) | 101 (47.2%) | 54 (40.3%) | 130 (50.0%) | |
| Occupational status, n (%) | |||||
| Work | 239 (65.8%) | 117 (54.9%) | 62 (46.3%) | 157 (60.4) | |
| Retired/disable | 86 (23.7%) | 69 (32.4%) | 41 (30.6%) | 62 (23.8%) | 0.001 |
| School | 20 (5.5%) | 21 (9.9%) | 20 (14.9%) | 26 (10.0%) | |
| Inactive | 18 (5.0%) | 6 (2.8%) | 11 (8.2%) | 15 (5.8%) | |
| Diagnosis, n (%) | |||||
| Crohn's disease | 241 (66.4%) | 130 (61.0%) | 47 (35.1%) | 165 (63.5%) | <0.001 |
| Ulcerative colitis | 122 (33.6%) | 83 (39.0%) | 87 (64.9%) | 95 (36.5%) | |
| Treatments, n (%) | |||||
| Non-immunosuppressant | 33 (9.1%) | 9 (4.2%) | 42 (31.3%) | 45 (17.3%) | <0.001 |
| Immunosuppressant | 330 (90.9%) | 204 (95.8%) | 92 (68.7%) | 215 (82.7%) | |
| Biological n (%) | |||||
| Intravenous | 112 (44.3%) | 109 (58.3%) | 29 (56.9%) | 61 (40.7%) | 0.003 |
| Subcutaneous | 141 (55.7%) | 78 (41.7%) | 22 (43.1%) | 89 (59.3%) | |
| Weeks | |||||
| 1–2 | 78 (21.5%) | 32 (15%) | 28 (20.9%) | 117 (45%) | |
| 3–4 | 198 (54.4%) | 89 (41.8%) | 42 (31.3%) | 51 (19.6%) | <0.001 |
| 5–6 | 51 (14.0%) | 68 (31.9%) | 43 (32.1%) | 60 (23.1%) | |
| 7 | 36 (9.9%) | 24 (11.3%) | 21 (15.7%) | 32 (12.3%) | |
aAdministrative visit COVID-19.
When performing a stratified analysis by the type of diagnosis, we found the same results.
DiscussionThe results of this study suggest that the acute phase of the pandemic by COVID-19 modified the activity managed by the AIN in the UACC, in a public hospital of reference in Barcelona (Spain). The 1095 activities recorded in the study interval clearly stand out in quantity, representing almost 50% more activity than in 2019 (p<0.001); 53.7% of them were related to aspects arising from the pandemic.
There has also been a change in proportions depending on the type of interaction with the UACC, in favor of telemedicine to the detriment of face-to-face activity, as seen in the study of Spanish group, when talking about the global work of the interdisciplinary team.20 Telemedicine has emerged as one of the best tools to maintain the quality of care for IBD patients, as demonstrated in previous studies19,21 and described in Italian groups in the current situation12,13 while face-to-face care has been minimized.
The busiest weeks concur with the WHO declaration of the global pandemic on the 11th and 14th March with the Spanish State's Declaration of State of Alarm, where movement was virtually forbidden.22
AIN increase of activity related to COVID-19 can be explained through several reasons. On the one hand, the statement by the Ministry of Health defining people with chronic health conditions and immunocompromised patients as people at risk could be viewed as one of them.23 Patients with IBD with immunosuppressive treatment usually refer to concern about the possibility of getting an infection9 with the pandemic. In a survey conducted by the European Federation of Crohn's and Ulcerative Colitis Associations (EFCCA) 85% of patients were afraid to become infected and 64% believed that immunosuppressants were associated with a higher risk of infection.17 On the other hand, patients taking biological treatment had to travel to pick up subcutaneous drugs at the pharmacy or to the daily clinic to administer their intravenous medication, despite the limitations placed on movement during the initial lockdown. It should be noted that Hospital Universitari de la Vall d’Hebron is the hospital with the highest number of patients admitted with COVID-19 in Catalonia.
Due to the preventive measures of lockdown, which have made accessibility to our services difficult, the use of telemedicine resources has been promoted. From the patient's point of view, it is vital to have flexible and fast access to health professionals,24 and this resource has been essential during the pandemic.
Several studies suggest that chronic disease management through telemedicine is acceptable and provides cost-effective solutions at a time when national health systems in European countries are experiencing problems with funding or sustainability.25 Currently, with the pandemic caused by COVID-19, there are also problems of accessibility to health services.
What has been surprising is the high number of consultations related to disease relapses, which has tripled in reference to the previous year, where 64% of patients had UC. Although more research would be required, it could be argued that as seen in other investigations, emotional and/or psychological factors such as anxiety or stress may be related to this augmented disease activity in our sample.4
A relation appears to be drawn in the profile of the active labor patient, under treatments that work on the immune system, since in the analysis stratified by pathology the same results are maintained. It would be logical to assume that in a situation such as this one, those active patients with immunosuppressants have experienced more feelings of anxiousness and worry. Perhaps we would need to design a more personalized care for this patient's profile, based on the shared decision-making paradigm. This is supported by the current patient-centered approach. With this approach, we could enlarge the relationship of the patient with their health team (communication and trust), improve the experience, attitudes and beliefs about their illness knowledge and treatment(s), and reduce the loneliness experienced by the patient.26
The increased activity of the UACC AIN has been shown effective, especially in telemedicine, which has been defined in the approach guidelines as a minimum and priority service.5 Historically, nurses have led the field of telematic assistance.10,19 It is compulsory to follow the recommendations of the second Nurses European Crohn's and Colitis Organisation [N-ECCO] Consensus, which defines the skills necessary for successful communication based on the following criteria: knowledge regarding communication techniques (active listening, simple language), skills (being present, empathy) and attitudes (open, quiet, reliable).10
With this study we join the international Nursing Now campaign promoted by the WHO and the International Council of Nurses (ICN),27 emphasizing the visibility in the management of AINs. We must go on focusing our work on accompanying patients in the emotional management of this health crisis, fostering the confidence of our patients through truthful and up-to-date information, and promoting adherence to treatments.
The Spanish health system appears to have shown sufficient resilience to absorb the blow of this pandemic, although many are the considerations to take into account.28,29 One of them could be the implementation of telemedicine, which, although it is not new, seems to have encountered many pitfalls along its implementation in the area of health care, as reflected by the Aguas M group.30 Studies like Taxonera C et al have demonstrated that patients reported a very high degree of satisfaction with and acceptance of telephone consultations.20 In time, we will have the opportunity to lead the unstoppable shift towards more universal and equitable health care.
Our study has some limitations: sociodemographic and clinical characteristics of our sample may not be comparable to other communities. While this study has provided us with information on telemedicine, it would also be interesting to analyze other determinants such as psycho-emotional aspects, perceived quality of life or sociocultural issues.
ConclusionThe pandemic has completely changed the paradigm of health care worldwide. With our study we have been able to verify the impact it has had in the activity managed by Crohn's-Colitis Care Unit nurses during the first wave of the pandemic. We have the opportunity to improve patient care, especially those patients’ profiles who were actively working, and also received immunosuppressive treatment.
Relevance to clinical practiceFinally, the identification of AIN activity in the UACC during the pandemic has provided useful information which will allow more efficient and quality planning and care management of the kind that has been shown to be needed by IBD patients in exceptional situations. Sharing experiences and proposals for improvement provide us greater knowledge to face the future. We believe it is our duty to maintain and strengthen care for our patients regardless of the circumstances they may be experiencing.
- •
We have shown a considerable increase in nurse activities with a decrease in human resources during the acute phase of the COVID-19 pandemic. This study has provided useful information that will allow be more efficient and quality planning and management of chronic condition's patients.
- •
COVID-19 Pandemic has completely changed the paradigm of healthcare. This must now be the point of departure to lead unstoppable shift towards more universal and equitable health care.
- •
There must now be a greater emphasis and responsibility placed upon the role of nurses in healthcare management. Our value is to be next to the patient to listen, teach and help to manage their emotions.
There is a funding from: Health Department of Generalitat de Catalunya. PERIS SLT008/18/00077.
Conflict of interestThe authors declared no conflicts of interest.
We want to recognize both the general population, who have been able to act at this extraordinary moment, professionals, and agencies, who helped to deal with this crisis.
The authors also acknowledge Coral, Isabel and Matthew for writing English assistance.

