






Una mujer de 24 años de edad desarrolló repetidos fenómenos tromboembólicos. Después de tres ataques (de embolia cerebral), ella tenía una ecocardiografía transtorácica, en la cual una masa ecogénica cardiaca fue detectada. Después de la resección quirúrgica con la extirpación del tumor, el diagnóstico histopatológico definitivo fue de osteosarcoma primario auricular izquierdo, con diferenciación osteogénica y condroblástico.
El osteosarcoma extra-esquelético (EO) es una neoplasia mesenquimal maligna poco frecuente, que produce osteoide maligno, hueso y/o material condroide. Al contrario del osteosarcoma esquelético, generalmente afecta a personas mayores de 20 años de edad y es muy raramente detectado ante-mortem, cuando es de localización cardiaca. El progreso y difusión de técnicas de imagen cardiacas, está contribuyendo para un diagnóstico más temprano de esta neoplasia. Este es un reporte de un caso de un paciente con un osteosarcoma primario de la aurícula izquierda.
A 24-year-old white woman developed repeated thromboembolic phenomena. After three strokes (cerebrovascular embolism) she had a transthoracic echo-cardiography and a cardiac echogenic mass was detected. After surgical resection with removal of the tumor the definitive histopathological diagnosis was left atrial primary osteosarcoma with osteogenic and chondroblastic differentiation.
Extra-skeletal Osteosarcoma (EO) is a rare malignant mesenchymal neoplasm that produces malignant osteoid, bone and/or chondroid material. Unlike skeletal osteosarcoma, it usually affects people over 20 years of age, and it is very rarely detected ante mortem when located in the heart. The improvement and diffusion of imaging technologies is allowing early detection of this condition. This is a case report of a patient with primary left atrial osteosarcoma.
¿ INTRODUCTION
Extra-skeletal Osteosarcoma (EO) is a rare malignant mesenchymal neoplasm that produces malignant osteoid, bone, and/or chondroid material. It is located in soft tissues without attachment to bone or periosteum.1 Unlike skeletal osteosarcoma, which primarily occurs in the first two decades of life, EO generally affects those over 20 years of age. It may occasionally involve the heart. Historically, postmortem detection of cardiac tumors was the prevailing rule. As a result, most large series are based primarily on autopsy data. As diagnostic techniques, in particular 2-D echocardiography, have improved and attained widespread utility, it is now possible to detect more cases of primary cardiac tumors before the demise of the patients. This report documents one such patient with a primary left atrial osteosarcoma.
¿ CASE REPORT
The patient was a 24-year-old white woman. She was healthy until August 2004 when she developed signs and symptoms related to repeated (three episodes) thromboembolic phenomena. Physical examination revealed her to be in good general health, lucid, oriented and conscious, with moist and pink mucous membranes, there was no cyanosis or jaundice. Cardiovascular examination revealed pulses with good amplitude and good peripheral perfusion, normal heart sounds, sinus tachycardia and a heart rate of 105 bpm. Vesicular breath sounds were audible throughout both lung fields. Neurologic examination demonstrated that she was alert and able to understand simple questions; however she could not remain standing. She was weak with decrease strength in both lower extremities. She was aphasic. Movements of the tongue and oropharynx were preserved. Facial palsy was noted on the right side.
After three strokes (cerebrovascular embolisms) she was investigated with a transthoracic echocardiography and a pedicular echogenic mass was detected in her left atrium. This tumor had a longitudinal axis of 7.3 cm and was adhered to the upper segment of the inter-atrial septum (Figures 1A and 1B).

Figure 1A. 2-D Tumor dimensions inside left atrium (3.7 X 3.5 cm).
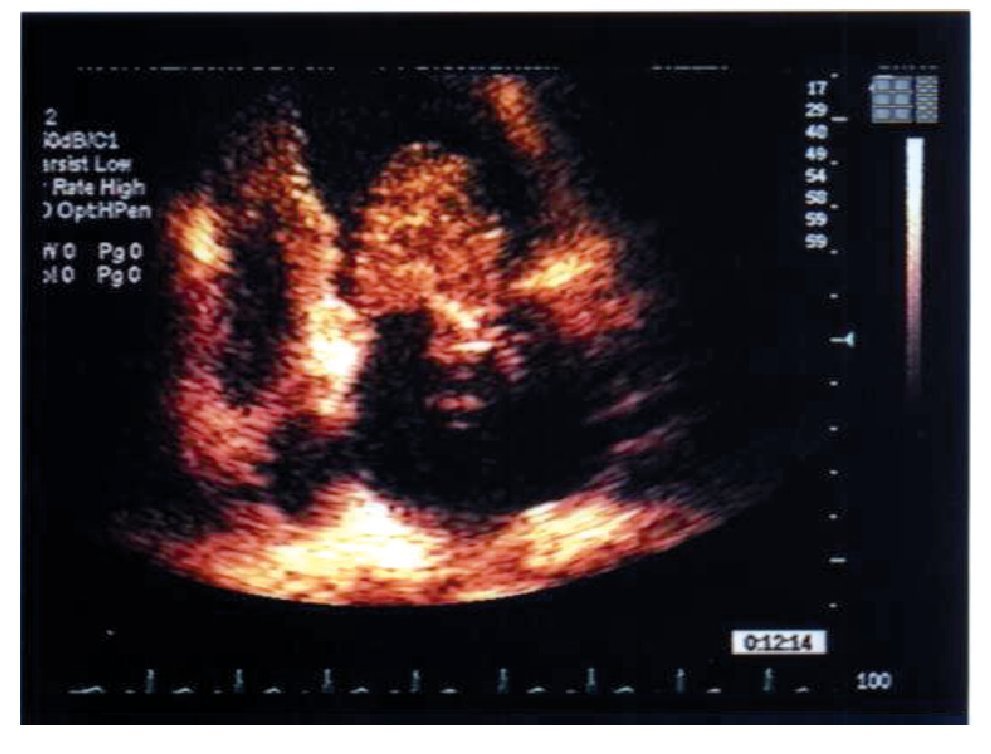
Figure 1B. 2-D protrusion of the tumor mass in diastole into the left ventricle (Apical angle).
Surgical resection with removal of the tumor from the left atrium was performed. The histological diagnosis was left atrial cardiac osteosarcoma with osteogenic (Figure 2A) and chondroblastic differentiation (Figure 2B). Imaging studies for staging (chest CT, abdominal CT, skull CT and bone scan) and hematological and biochemical investigations failed to reveal signs of tumor at distant sites. The definitive diagnosis was primary left atrial osteosarcoma (Figures 2A and 2B).
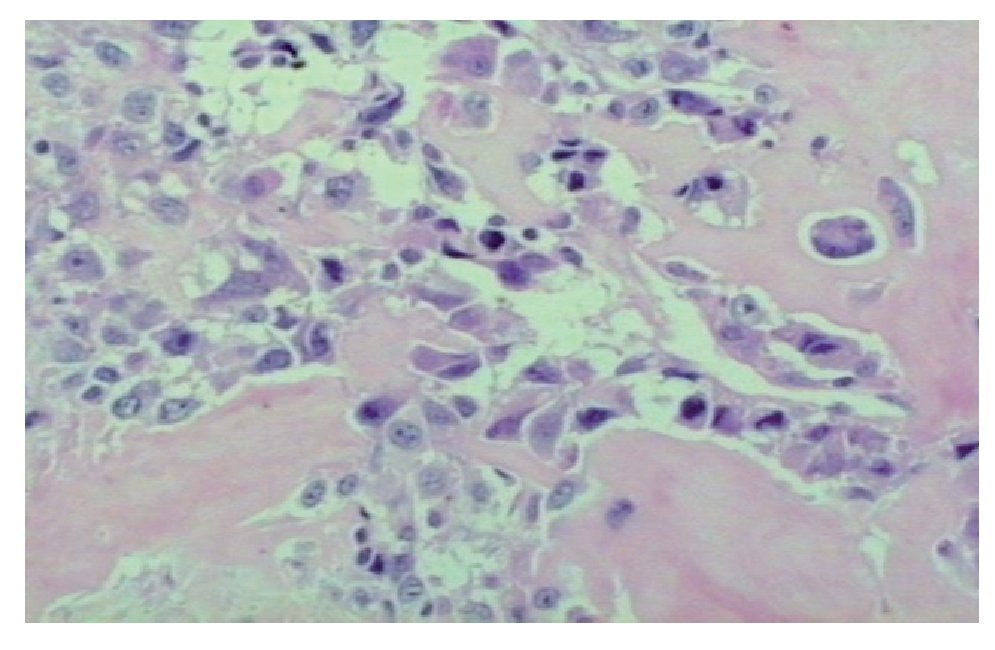
Figure 2A. Formation of osteoid by atypical pleomorphic osteoblast (Hematoxilin & heosin, X200).
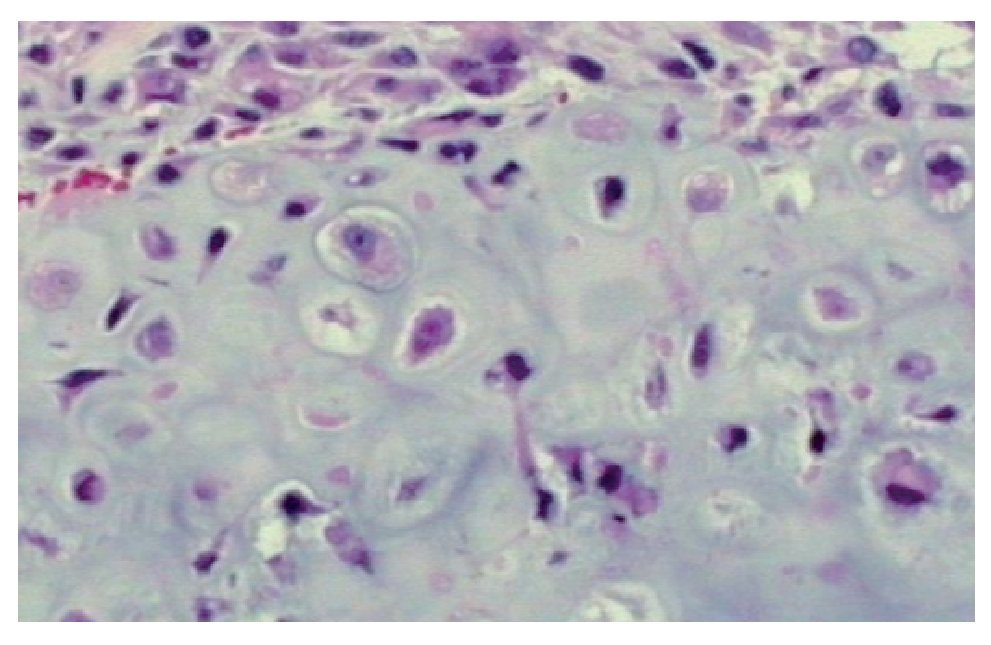
Figure 2B. Cellular anaplastic area with cartilage formation (Hematoxilin & heosin, X200).
The patient was treated with Ifosfamide+Mesna/ Etoposide and Cisplatinum.1-3 Doxorubicin could not be administered because of a prior myocardial infarction and a reduced baseline ejection fraction of 31%,4 Methotrexate could not be utilized due to technical problems in measuring blood levels. Six months after the diagnosis of the primary cardiac neoplasm she developed multiple brain metastases. She was at grade four on ECOG performance status, since she was completely disabled, without any condition of carry on any self-care and totally confined to bed.5 The treatment was supportive and four months later she died.
¿ DISCUSSION
The occurrence of primary cardiac tumors is much less common than metastatic lesions of the heart. Cardiac tumors are rare, difficult to diagnose and have particular clinical manifestations, location, morphology, size and radiological findings.6 The incidence ranges from 0.0017% to 0.35% in the general population.7 Based on a large autopsy series, approximately 72% of primary cardiac tumors are benign, while 28% are malignant.
Of the benign tumors, about 50% are myxomas. The benign tumors include rhabdomyomas, fibromas, papillary fibroelastomas, hemangiomas, pericardial cysts, lipomas, hamartomas, teratomas, mesotheliomas, and paragangliomas or pheochromocytomas. Of all malignant tumors, 33% are angiosarcomas, 20% rhabdomyosarcomas, and 15% mesotheliomas. Primary extra-skeletal osteosarcomas of heart account for approximately 1.1% of all cardiac tumors are mostly seen within the left atrium and can metastasize.8
No specific causes of cardiac sarcomas are known. Fine and Stout are of the opinion that visceral osteosarcomas result from the unilateral development of osseous component of a malignant mesenchymoma. 9 Primary sarcoma of the heart is rare with a dismal short-term prognosis. There is no particular age or sex predilection for this malignant cardiac neoplasm. The literature reports that the tumor has been detected from ages of three days to 79 years, with 75% of these tumors occurring between the ages 20 and 60 years.10 They can arise from any cardiac structure; most exhibit a predilection for a specific chamber. Angiosarcomas are more commonly found in the right atrium whereas myxomas, osteosarcomas, fibrosarcomas and undifferentiated sarcomas are found predominantly in the left atrium.11 The growth pattern of these malignancies is predominantly mural, although they may be polypoid, infiltrating or both.12 The location, size and mobility of tumors determine their clinical features. Most patients present with one or more features of the triad: embolism, intra-cardiac obstruction and constitutional symptoms. In the literature, approximately half of the embolic problems involve the central nervous system.13
The 2-D echocardiography remains the primary mode of diagnosis. Echocardiography provides important information on the size and shape, site of attachment, and also on the pattern of movement of the tumor. Malignant tumors often involve the right side of the heart and invade the myocardium, with extension into the pulmonary veins or pericardial effusion.14 Primary osteosarcomas are rare and most often involve and arise in the left atrium, their appearance and location may simulate a myxoma.7
Tumor calcification has been reported in several types of benign and malignant cardiac tumors, including rhabdomyomas, myxomas, fibromas, teratomas, hematomas, and angiomas. Calcification varies from a speckled pattern to a round clump of calcium mimicking mitral annular or valve calcification and may be visible on plain x-ray films, echocardiography or CT. The extent of calcification is generally minimal in benign tumors and dense calcification should raise suspicion for an extra-skeletal osteosarcoma.7
Primary cardiac malignancies are difficult to diagnose clinically and may be misdiagnosed at an initial stage. Fernandez reported that approximately 20% of the patients with primary neoplasm of the heart were asymptomatic at the initial assessment.15
Currently, doxorubicin, cisplatin, high-dose methotrexate with leucovorin rescue and ifosfamide are considered the most active agents against osteosarcoma.2 The treatment for osteosarcoma is at a stagnation point since most patients today are still receiving exactly the same drugs as they would have 25 or more years ago, namely doxorubicin, cisplatin, high-dose methotrexate, and sometimes ifosfamide, in varying combinations.16 -18 Questions about which of the 'standard' drugs combined at which dosages would result in an 'ideal' combination remain unanswered compromising, the poor prognosis of patients with these tumours.18
The prognosis for primary cardiac sarcoma remains dismal. The reasons for the dismal prognosis are the advanced tumor stage at presentation, non-specific symptomatology, insufficient awareness of these lesions, due to their rarity, delayed diagnosis and/or misdiagnosis, which leads to advanced tumor stage at presentation.19
Despite the bleak prognosis, a temporary benefit in quality of life and survival might be observed in patients with primary cardiac sarcoma. Wide surgical excision is the only treatment capable of improving outcome even with palliative resections. However, long-term survivors are still anecdotal. The optimization of chemotherapy regimens including anthracyclins and high-dose ifosfamide could improve quality of life and overall survival.21, 22
¿ CONCLUSION
There is extensive literature on cardiac osteosarcoma diagnosed post mortem, but this report shows an in vivo diagnosis and intends to call attention to the presentation of this patient with recurrent thromboembolic events leading to an echocardiograph investigation that resulted in the diagnosis of an underlying primary malignant neoplasm of the heart. The 2-D echocardiography is very helpful in the diagnosis of a number of cardiac diseases and might so diagnose cardiac neoplasm.
¿ ACKNOWLEDGMENT
The authors would like to express gratitude to Carlos Henrique Escosteguy Barrios for the proof-reading of the Case Report.
Corresponding Author: Dona Laura Street 226/202, ZP 90430-090, Porto Alegre, Rio Grande do Sul, Brazil. Oncology Department
Phone: (5551) 40096010. Fax: (5551) 4009 6000.
Email:julio@clinionco.com.br