




La sarcoidosis gastrointestinal es una forma infrecuente de la sarcoidosis. La sarcoidosis gástrica afecta aproximadamente al 10% de los pacientes con enfermedad sistémica y sólo rara vez se presenta con síntomas. Aquí presentamos el caso de una úlcera sangrante gástrica en una mujer de 66 años de edad con sarcoidosis pulmonar.
Las biopsias de la úlcera mostró granulomas no caseificantes y fueron positivos para Helicobacter pylori. La afección gástrica por la sarcoidosis suele ser asintomática, sin embargo, los médicos deben reconocer que se pueden presentar úlceras sintomáticas, aunque raramente.
Gastrointestinal (GI) tract sarcoidosis is an uncommon form of sarcoidosis. Gastric sarcoidosis affects approximately 10% of patients with systemic disease and only rarely presents with symptoms. Here we present the case of a bleeding gastric ulcer in a 66-year-old female with pulmonary sarcoidosis. Biopsies of the ulcer showed non-caseating granulomas and were positive for Helicobacter pylori. She received treatment with PPIs and H. pylori eradication therapy and recovered well. Gastric involvement in sarcoidosis is usually asymptomatic, however, clinicians should recognize that it can present with symptomatic ulcers, albeit rarely.
Introduction
Sarcoidosis is a systemic granulomatous disease of unknown etiology that is characterized by the formation of non-caseating granulomas. Sarcoidosis commonly involves the mediastinal and hilar lymph nodes, lungs, liver, eyes, skin, and nervous system.
Gastrointestinal (GI) tract involvement in sarcoidosis is rare. Gastric sarcoidosis affects approximately 10% of patients with systemic disease.1 GI sarcoidosis commonly occur subclinically, with clinical manifestations present in only 0.1 to 0.9% of patients with the disease.2 About 40% patients with sarcoidosis show subtle changes in their GI immune responses. The significance of these altered immune responses in the pathogenesis of GI tract sarcoidosis is unknown.3 Sporadic case reports and case series of symptomatic GI tract sarcoidosis have described the clinical and radiographic manifestation of this uncommon entity. The clinicopathologic features of GI tract sarcoidosis are non-specific, and other diseases should be excluded prior to making this diagnosis.
Case Report
A 66-year old woman with a history of colon cancer 14 years earlier, for which she received curative treatment with surgery and post operative radiotherapy and chemotherapy. While on surveillance multiple mediastinal, subcarinal and tracheal lymph nodes were found on a chest CT scan. Biopsy of these nodes revealed non-caseating granulomas, which were negative for acid-fast bacilli, fungi or other microorganisms; she had a negative tuberculin test and high levels of angiotensin converting enzyme (ACE). Spirometry was normal. Patient was discharged with a diagnosis of pulmonary sarcoidosis. She had been asymptomatic for eight years until she presented to the hospital with complaints of hematemesis and melena of 48 hours duration, her hemoglobin was 9 g/dL (previous was 13.6 g/dL), blood pressure was 80/60 mmHg with a pulse of 96. She was treated with intravenous fluids and underwent an upper endoscopy that revealed a 10 mm lesion with irregular and elevated borders, ulcerated with a fibrin plug, located on the posterior wall of the greater curvature. Biopsies of the lesion showed non-caseating granulomas and were positive for Helicobacter pylori (Figure 1). Tests using special stains for fungi, acid-fast bacilli gave negative results. She received treatment with PPIs and H. pylori eradication therapy. Patient recovered well and her last endoscopy shows the lesion without ulceration (Figure 2).
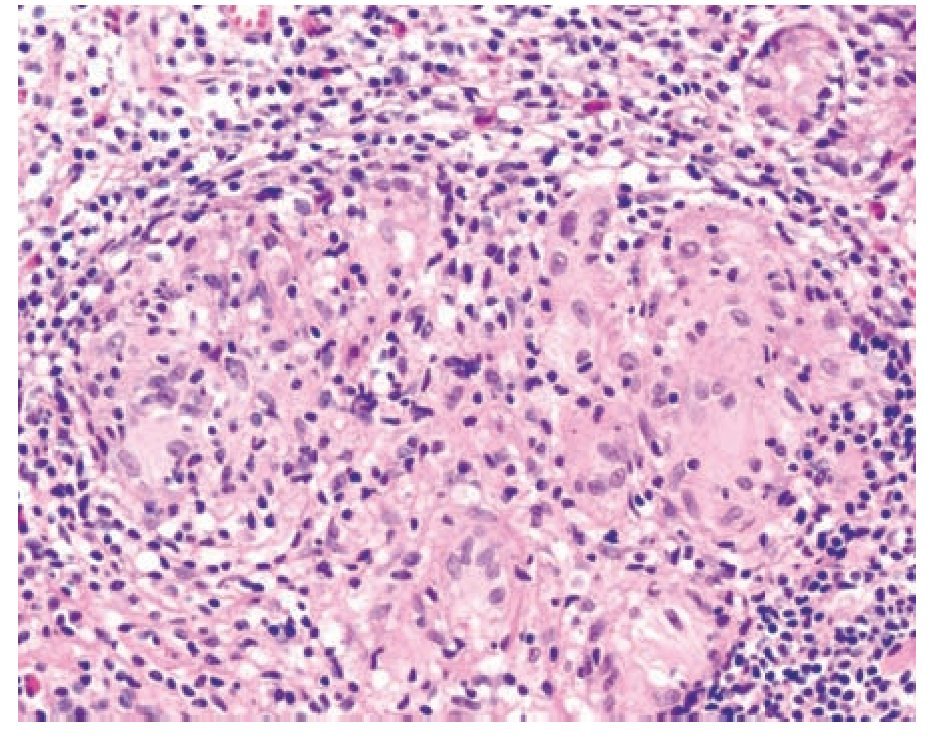
Figure 1. High magnification hematoxylin and eosin (H&E) stain of gastric mucosa, demonstrating non-caseating epithelioid-cell granuloma including giant cells.
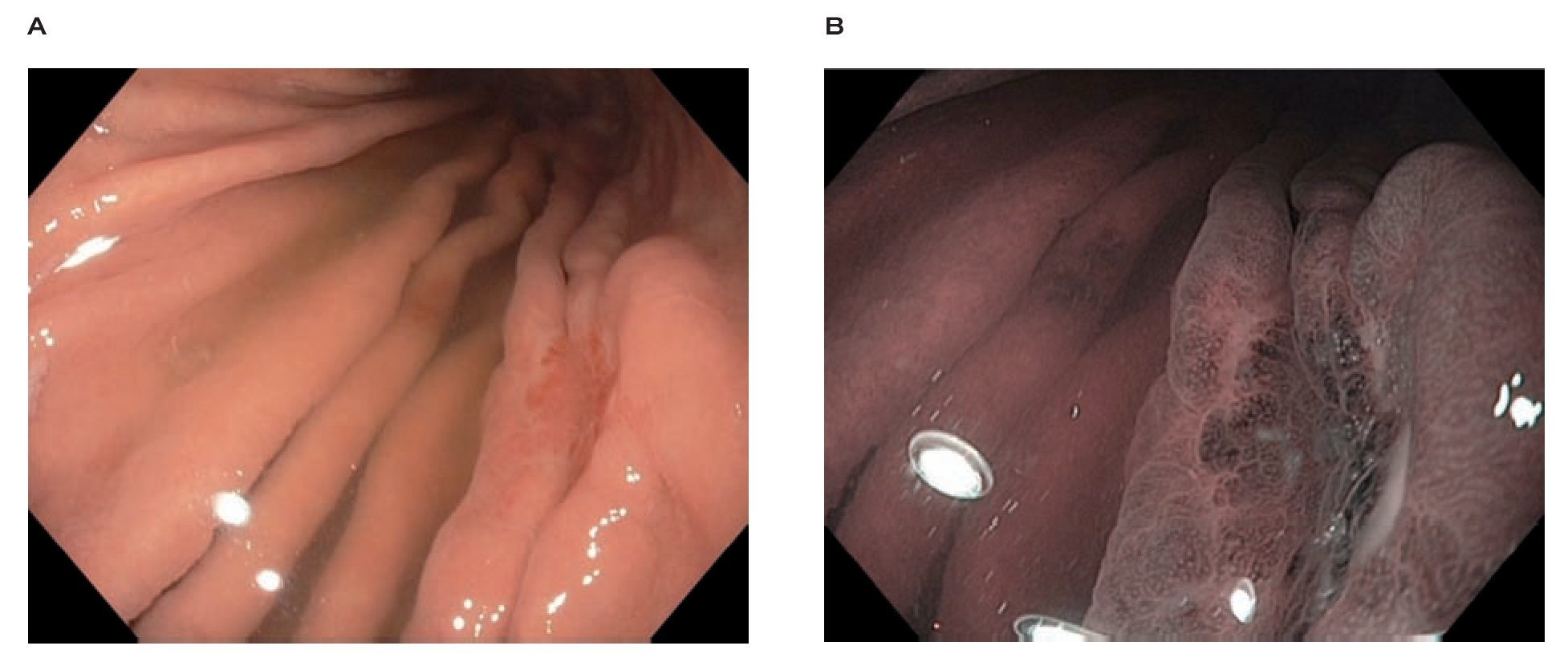
Figure 2. Lesion of the posterior wall of the greater curvature, upper endoscopy A), Narrow band imaging B).
Discussion
Schaumann first described gastric sarcoidosis in 1936.4 Although gastric sarcoidosis is rare, it is the most common form of GI tract sarcoidosis and may present in the context of generalized disease or as an isolated finding. It may mimic other gastric processes, including peptic ulcer disease, Menetrier's disease, localized hypertrophic gastritis, Crohn disease, and carcinoma.5 The diagnosis of gastric sarcoidosis is dependent on histological evidence of non-caseating granulomas on mucosal biopsies. Subclinical gastric sarcoidosis is the most common kind. Isolated cases have been described where known sarcoidosis patients have had gastric involvement.6 The outstanding characteristic of this case was that the patient was severely symptomatic with upper GI bleeding owing to a gastric ulcer, which was diagnosed at endoscopy. She also had H. pylori infection and this likely contributed.
The manifestations of gastric sarcoidosis are usually related to ulceration of involved mucosa or narrowing of gastric or pyloric lumen caused by granulomatous inflammation and scarring. The most common presenting symptom is epigastric pain; upper GI hemorrhage also has been reported. Other symptoms are nausea, vomiting, bloating, and early satiety. Although ulcerative gastric sarcoidosis can present throughout the stomach, it tends to occur more frequently in antral mucosa.7 The decision to provide treatment should reflect a weighing of the risks of using corticosteroids, the most common therapy, against the potential benefits. Treatment with corticosteroids results in symptomatic improvement in 66% of patients.8 Patients with gastric sarcoidosis may have a partial response to proton pump inhibitors and antacids.9 This case illustrates the importance of considering gastric sarcoidosis in patients with sarcoidosis and gastrointestinal symptoms.
Correspondence: Dra. Claudia Herrera de Guise.
Gastroenterology Department. Instituto Nacional de Ciencias Médicas y Nutrición "Salvador Zubirán". Vasco de Quiroga 15, Col. Sección XVI, Tlalpan. Mexico City, Mexico.
E-mail:cherrera@infomatrix.com.gt