


The objective of this study was to establish the role of the TLR-4 gene polymorphisms in individuals in risk of developing ACS.
MethodsThe study included 457 Mexican patients with ACS and 283 control individuals. The TLR-4 Asp299Gly and TLR-4 Thr399Ile single nucleotide polymorphisms were genotyped using 5′ exonuclease TaqMan genotyping assays on an 7900HT Fast real-time PCR system according to manufacturer's instructions (Applied Biosystems, Foster City, USA).
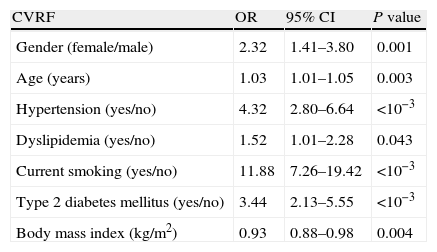
ResultsThe results obtained in this study showed that the frequency of the two polymorphisms (TLR-4 Asp299Gly and TLR-4 Thr399Ile) studied were similar between patients with ACS and healthy controls. Multiple logistic regression analysis showed that the largest risk factor for ACS development was given by smoking (11.88-fold increased risk), hypertension (4.32-fold increased risk), type II diabetes (3.44-fold increased risk), gender (2.32-fold increased risk), and dyslipidemia (1.52-fold increased risk).
ConclusionThe Asp299Gly and Thr399Ile polymorphisms were not associated with susceptibility to ACS in the Mexican population.
El objetivo de este estudio fue establecer el papel de los polimorfismos del gen TLR-4 en individuos en riesgo de desarrollar síndrome coronario agudo (SCA).
MétodosEl estudio incluyó a 457 pacientes mexicanos con SCA y 283 individuos como grupo control. Los polimorfismos de un solo nucleótido TLR-4 Asp299Gly y TLR-4 Thr399Ile fueron determinados usando ensayos TaqMan 5′ exonucleasa en un equipo tiempo real 7900HT (Fast real-time PCR system) de acuerdo con instrucciones del fabricante Applied Biosystems, Foster City, EE.UU.
ResultadosLos resultados obtenidos mostraron que las frecuencias de los 2 polimorfismos (TLR-4 Asp299Gly y TLR-4 Thr399Ile) estudiados fueron similares entre pacientes con SCA e individuos control. No obstante, el análisis de regresión logística mostró que los factores de mayor riesgo para desarrollar SCA se debieron a tabaquismo (incrementa 11.88 veces el riesgo), hipertensión (incrementa 4.32 veces el riesgo), diabetes tipo 2 (incrementa 3.44 veces el riesgo), género (incrementa 2.32 veces el riesgo), y la dislipidemia (incrementa 1.52 veces el riesgo).
ConclusiónDeterminamos que los polimorfismos Asp299Gly y Thr399Ile no se asocian con la susceptibilidad al SCA en la población mexicana.
Atherosclerosis is a multifactorial disorder that results from an excessive inflammatory response to various forms of injurious stimuli to the arterial wall.1–3 The inflammatory processes, genetic background, and various environmental factors, coupled to dyslipidemia, including hypertension, diabetes, obesity, and smoking play an important role in the progression of the atherosclerotic plaque.3–5 The transition of a stable coronary atherosclerotic lesion into a ruptured and eroded plaque results in the clinical manifestation of an acute coronary syndrome (ACS).5,6 The ACS includes unstable angina and myocardial infarction caused mainly by rupture or erosion of the atherosclerotic plaque, with subsequent thrombus formation.6–8 Mounting evidence suggests that specific agents enhance arterial inflammation during atherogenesis, based on their interaction with receptor signaling pathways of the innate immune systems.9,10 Toll-like receptor 4 (TLR-4) is part of the innate immunity response cascade. It has been associated as one of the factors contributing to the deleterious process of atherosclerosis.11–13TLR-4 is well known as a pattern-recognition receptor for exogenous lipopolysacharide (LPS) derived from gram-negative bacterial infection.14,15 However, several studies showed that TLR-4 interacts with other ligands, such as fibrinogen,16 fibronectin,17 heat-shock protein,18 hyaluronan oligosaccharide19 and modified low-density lipoproteins (LDL),20,21 playing an important role in the development of the atherosclerotic plaque. The TLR-4 gene is located in the 9q32 region.15TLR-4 presents two single nucleotide polymorphisms (SNP), both polymorphisms, rs4986790 (Asp299Gly) and rs4986791 (Thr399Ile), are located in the coding region. These (SNPs) affect TLR-4 extracellular domain and result in amino acid exchanges: an aspartic acid for a glycine at position 299 (Asp299Gly) and a threonine for a isoleucine at position 399 (Thr399Ile).22,23 Several studies associate these polymorphisms with several inflammatory diseases, such as ACS, gastric cancer, carotid artery elasticity, chronic obstructive pulmonary disease, and atherosclerosis.24–28 Considering the prominent role of the TLR-4 as initiator of the inflammatory response, this study was based on the assumption that the TLR-4 gene polymorphisms have a measurable influence in the development of the atherosclerotic plaque and contributes to or increases the occurrence of ACS. The objective of this study was to establish the possible role of the TLR-4 gene polymorphisms as a risk factor for ACS in a group of Mexicans patients.
MethodsStudy populationsThe study included 457 Mexican patients with ACS (368 males and 89 females, mean age 59.7±11.02) that were attended to our Institution. Three hundred forty-two presented myocardial infarction and 115 presented unstable angina. All subjects were diagnosed according to the World Health Organization and the American Heart Associated (AHA)/American College of Cardiology (ACC).29 Basis in clinical history, physical examination with electrocardiography, chest radiography, echocardiography, and coronary angiography. The group of patients was compared with a group of 283 healthy unrelated individuals (202 males and 81 females, mean age 55.39±7.23). This group was selected from people arriving with the purpose to donation at the blood bank at our institute. According to the medical records, none of these had diabetes, dyslipidemia, hypertension or other pathology. On the other hand, subclinical atherosclerosis was discarded through determined calcium score by multi-detector computed tomography. The values were zero in these individuals. All subjects included in the study (patients and controls) were ethnically matched, and we considered as Mexican Mestizos only those individuals who had been born in Mexico for three generations, including their own. A Mexican Mestizo is defined as someone born in Mexico, who is a descendant of the original autochthonous inhabitants of the region and of individuals, mainly Spaniards, of Caucasian and African origin, who came to the American continent during the sixteenth century. The Institutional Ethics and Research Committees approved the study, and all subjects provided written, informed consent.
DNA extractionGenomic DNA from whole blood containing EDTA was isolated with a standard technique.30
Determination of the TLR-4 genotypesThe TLR-4 Asp299Gly (rs4986790) and TLR-4 Thr399Ile (rs4986791) single nucleotide polymorphisms were genotyped using 5′ exonuclease TaqMan genotyping assays on an 7900HT Fast real-time PCR system according to manufacturer's instructions (Applied Biosystems, Foster City, USA).
Statistical analysisGene frequencies of TLR-4 polymorphisms in patients and controls were obtained by direct counting. Hardy–Weinberg equilibrium was evaluated by Chi2 test. Statistical analysis was carried out with the Stata 10.0 software for Windows. In the exploratory analysis, numerical data showed a different distribution from normal standard (Gaussian distribution) (Shapiro Wilk's test of normality, p>0.05), nominal and categorical variables were tabulated to estimate their proportions. Hypertension, altered lipid profile, smoking, and type 2 diabetes mellitus had two categories, yes or no, and all described the current condition of patients and healthy controls. Comparison of numerical variables, such as age and body mass index, between both groups was carried out with Mann–Whitney U test, data are presented as the 25th percentile, median, and 75th percentile. Categorical variables were analyzed with Chi2 tests and presented as absolute frequencies and proportions. Statistical significance was set at p≤0.05. Multiple logistic regression analysis was carried out to identify the variables that better explain the risk of developing ACS between patients and healthy controls. Models were constructed including one variable at a time to identify confounding bias; changes in estimated odds ratios (ORs) were less than 10%. When a main effect model was reached, effect modification was also tested, interaction terms were constructed between age and BMI, hypertension and type 2 diabetes mellitus, smoking and hypertension, and gender and BMI, no significant ORs (p ≤ 0.20) were identified and therefore these terms were not included in the final model. Hosmer–Lemeshow Goodness of fit test was performed for each multiple logistic model. Pairwise linkage disequilibrium (LD, D′) estimations between polymorphisms and haplotype reconstruction were performed with Haploview version 4.1 (Broad Institute of Massachusetts Institute of Technology and Harvard University, Cambridge, MA, USA).
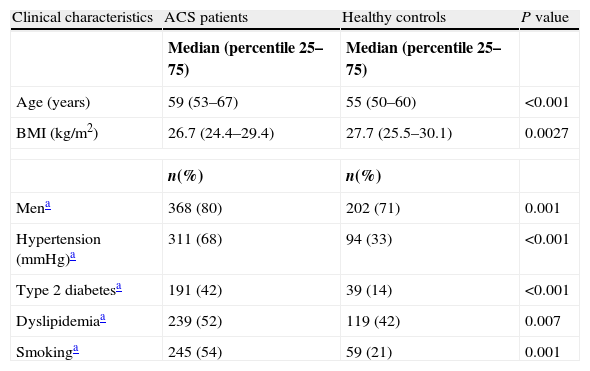
ResultsCharacteristic of the study sampleBaseline characteristic of the ACS patients and healthy controls included in the study are shown in Table 1.
Baseline clinical characteristics of the study group.
| Clinical characteristics | ACS patients | Healthy controls | P value |
| Median (percentile 25–75) | Median (percentile 25–75) | ||
| Age (years) | 59 (53–67) | 55 (50–60) | <0.001 |
| BMI (kg/m2) | 26.7 (24.4–29.4) | 27.7 (25.5–30.1) | 0.0027 |
| n(%) | n(%) | ||
| Mena | 368 (80) | 202 (71) | 0.001 |
| Hypertension (mmHg)a | 311 (68) | 94 (33) | <0.001 |
| Type 2 diabetesa | 191 (42) | 39 (14) | <0.001 |
| Dyslipidemiaa | 239 (52) | 119 (42) | 0.007 |
| Smokinga | 245 (54) | 59 (21) | 0.001 |
Abbreviations: ACS, acute coronary syndrome; BMI, body index mass.
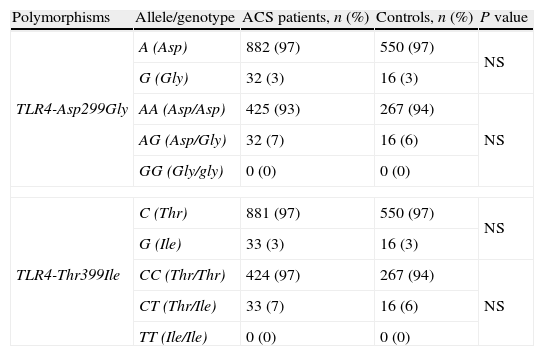
The observed and expected frequencies in the two polymorphic sites of the toll-like receptor (TLR-4) were in Hardy–Weinberg equilibrium. The allele and genotype frequencies of the two studied polymorphisms (positions +896 A>G (Asp299Gly) and +1196 C>T (Thr399Ile)) were similar between patients with ACS and healthy controls (Table 2). The multiple logistic regression analysis showed that the largest risk for ACS development was given by smoking (11.88-fold increased risk), hypertension (4.32-fold increased risk), type II diabetes (3.44-fold increased risk), gender (2.32-fold increased risk), and dyslipidemia (1.52-fold increased risk) (Table 3). The +896 A>G (Asp299Gly) and +1196 C>T (Thr399Ile) polymorphisms showed a strong linkage disequilibrium (D′=0.82) and were used to construct two haplotypes (AC and GT). The haplotype “AC” showed a similar distribution in ACS patients and healthy controls (95.7% and 96.8%, respectively). Moreover, the “GT” haplotype showed a similar decreased in patients and control (4.3%, and 3.2%, respectively).
Allele and genotype distribution between cases and controls.
| Polymorphisms | Allele/genotype | ACS patients, n (%) | Controls, n (%) | P value |
| TLR4-Asp299Gly | A (Asp) | 882 (97) | 550 (97) | NS |
| G (Gly) | 32 (3) | 16 (3) | ||
| AA (Asp/Asp) | 425 (93) | 267 (94) | NS | |
| AG (Asp/Gly) | 32 (7) | 16 (6) | ||
| GG (Gly/gly) | 0 (0) | 0 (0) | ||
| TLR4-Thr399Ile | C (Thr) | 881 (97) | 550 (97) | NS |
| G (Ile) | 33 (3) | 16 (3) | ||
| CC (Thr/Thr) | 424 (97) | 267 (94) | NS | |
| CT (Thr/Ile) | 33 (7) | 16 (6) | ||
| TT (Ile/Ile) | 0 (0) | 0 (0) | ||
Estimated risk of ACS between case and controls.
| CVRF | OR | 95% CI | P value |
| Gender (female/male) | 2.32 | 1.41–3.80 | 0.001 |
| Age (years) | 1.03 | 1.01–1.05 | 0.003 |
| Hypertension (yes/no) | 4.32 | 2.80–6.64 | <10−3 |
| Dyslipidemia (yes/no) | 1.52 | 1.01–2.28 | 0.043 |
| Current smoking (yes/no) | 11.88 | 7.26–19.42 | <10−3 |
| Type 2 diabetes mellitus (yes/no) | 3.44 | 2.13–5.55 | <10−3 |
| Body mass index (kg/m2) | 0.93 | 0.88–0.98 | 0.004 |
Abbreviation: CVRF, cardiovascular risk factor.
In the present work, we studied two polymorphisms (Asp299Gly and Thr399Ile) located in the TLR-4 gene in 457 patients with ACS and 283 healthy controls. In humans, both polymorphisms affect TLR-4 extracellular domain and individuals that possess these polymorphisms are hyporesponsive to several ligands.11–13 In this study, we observed that the distribution of the two polymorphisms were similar in patients with ACS and healthy controls. The association of the TLR-4 gene polymorphisms with several diseases in different populations is controversial with positive and negative results. For example, Koch et al. reported no association of the two TLR-4 gene polymorphisms with myocardial infarction in 3647 patients and 1211 individuals control with angiographic normal coronary and without signs or symptoms of myocardial infarction. In this work the authors showed that gender (women and men) did not sex-related associations and genotypes of polymorphisms in a Caucasian population,31 agreeing with our results. Similar data were obtained by Labrum et al. who studied the two TLR-4 gene polymorphisms in a cohort 3000 individuals obtained of carotid atherosclerosis progression study. In this study showed no association between carotid artery intima-media thickness and polymorphisms of the TLR4 gene in 1460 males and 1540 females. However, there was no association between polymorphisms of TLR4 gene and baseline intima-media thickness. In addition, is reported there was no interactions between polymorphisms and the cardiovascular risk factors (C-reactive protein, smoking, body mass index and diabetes) in Caucasian population.32 Moreover, Zee et al. reported that the Asp299Gly polymorphism is not associated with risk of incident myocardial infarction and stroke in 695 patients and 695 individuals control matched by age, smoking history, adjusted by body mass index, history of hypertension and presence or absence of diabetes, in a US population,33 in line with our data. In contrast with these results, Ameziane et al. reported that the 299Gly allele is associated with decreased risk of developing ACS in 183 patients and 216 controls (OR=0.41). In addition, in controls the individuals with heterozygous (299 Asp/Gly) genotype was also associated with a significantly decrease in plasma fibrinogen and soluble vascular cellular adhesion molecule-1 levels in a French population.24 On the other hand, Hernesniemi et al. reported an association of the 299Gly allele with increased carotid artery elasticity in a cohort of 2201 young adults. In addition, according to multivariate linear regression analysis adjusted with potential confounders, the 299Gly allele carriers had significantly higher carotid arterial compliance, measured in increase of luminal diameter percentage in response to blood pressure. This increase has beneficial effects, because it reduces the risk of future cardiovascular events.25 Santini et al. reported in a case–control study that the CT (Thr/Ile) genotype of the Thr388Ile polymorphism increases susceptibility to gastric cancer (OR=5.38). In addition, according with regression analysis determine that the Thr/Ile genotype adjusted for age, sex (male), alcohol intake and smoking status increases susceptibility to gastric cancer (OR=3.62).26 Similar data were reported by Speletas et al., who observed that the T (Ile) allele and CT (Thr/Ile) genotype (OR=2.4 and OR=2.0, respectively) are associated with risk of developing chronic obstructive pulmonary disease in a case–control study. Unfortunately, authors no determine differences between polymorphism and clinical and demographic data.27 Nonetheless, the results obtained of the multiple logistic regression analysis showed that smoking, hypertension, type II diabetes, and gender increased more the risk of developing ACS. These data confirm the previous results obtained by our group in a small group of patients.34 Moreover, this analysis showed no association between the TLR4 gene polymorphisms and clinical characteristics of the ACS in Mexican patients.
Limitations of the studyWe recognize that our study has limitations; one was the limited samples number in controls group. Another limitation was pairing by gender between patients group and control group. Some experts consider that a proper analysis would need a relation between controls and patients of 1:1. Unfortunately for this report we could not meet this criterion. Nonetheless, the results from the present study are concordant with data reported in the international literature.
ConclusionThe Asp299Gly and Thr399Ile gene polymorphisms were not associated with ACS in the present group of Mexican patients.
FundingThis work was supported in part by grants from the Consejo Nacional de Ciencia y Tecnología (project 156911) and Fundación Gonzalo Rio Arronte, Mexico City, Mexico.
DisclosureThe authors alone are responsible for the content and writing of the paper.
Conflicts of interestThe authors report no conflicts of interest.
The authors are grateful to the study participants.