

The study of the impact of psychological interventions to reduce stress at work is a focus of increasing attention for health professionals and employers. The objective of this study was to evaluate the effect of cognitive behavioral and psychoeducational intervention on coping strategies, burnout syndrome symptoms and symptoms associated with stress in public officials of the State Human Rights Commission of Veracruz, Mexico.
Material and methodsThirty one participants were randomly assigned to either an experimental group that received the treatment (n=15) or a waiting list control group (n=16), both responded to self-report measures before and after the intervention, which was performed on the job site in eight two-hour sessions. Student's t-test was used and the magnitude of the effect was analyzed with Cohen's d-test to analyze the data.
ResultsBoth groups were equivalent before the intervention in both the sociodemographic and psychological variables. After the intervention, compared to the control, the experimental group made a higher use of active coping strategies and showed a decrease in their levels of burnout, with large effect sizes in both cases.
ConclusionFindings suggest that a psychological intervention based on psychoeducation and problem solving is effective and viable to support public officials in managing work stress.
El estudio del impacto de las intervenciones psicológicas para reducir el estrés en el trabajo es un foco de atención cada vez mayor para los profesionales de la salud y los empleadores. El objetivo de este estudio fue evaluar el efecto de una intervención cognitivo conductual y psicoeducativa sobre las estrategias de afrontamiento, los índices del síndrome del burnout y de la sintomatología asociada al estrés en funcionarios públicos de la Comisión Estatal de Derechos Humanos de Veracruz, México.
Material y métodosTreinta y un participantes fueron asignados aleatoriamente al grupo experimental que recibió el tratamiento (n=15) o al grupo control en lista de espera (n=16). Ambos cumplimentaron medidas de autoinforme antes y después de la intervención, la cual se realizó en el sitio de trabajo en ocho sesiones de dos horas cada una. Se utilizó la prueba t de Student y se analizó la magnitud del efecto con la prueba d de Cohen para analizar los datos.
ResultadosAmbos grupos fueron equivalentes antes de la intervención tanto en las variables sociodemográficas como en las psicológicas. Tras la intervención, en comparación con el control, el grupo experimental aumentó en el uso de estrategias de afrontamiento activo y disminuyó en indicadores de síndrome del burnout; ambos casos con tamaño del efecto grande.
ConclusiónLos hallazgos sugieren que la intervención psicológica basada en psicoeducación y resolución de problemas es efectiva y viable para apoyar a funcionarios públicos en la gestión del estrés laboral.
According to Maslach, Schaufeli, and Leiter (2001), Burnout Syndrome (BS) is a prolonged response to chronic emotional and interpersonal workplace stressors comprising three dimensions: (a) emotional exhaustion (EE), characterized by a lack of energy and enthusiasm and a feeling that one is running out of resources; (b) depersonalization (DP), also called cynicism, characterized by treating people impersonally as objects; and (c) low personal fulfillment (PF) at work, characterized by a tendency to negatively self-evaluate him/herself. The cognitive and behavioral efforts an individual makes to handle the stressors of the working environment are known as coping strategies (Lazarus & Folkman, 1984), and play an important role in the modulation of BS levels and their side effects (Cox, Kuk, & Leiter, 1993). People with active coping (AC) skills who focus on solving work problems that cause them stress develop lower rates of BS compared to those who use passive coping strategies (PC), also called emotion-centered strategies, in which ignoring the problem or distracting oneself from it, is a means of coping with the discomfort (Shin et al., 2014).
Maintaining high BS rates for prolonged periods is associated with significant physical health effects such as hypercholesterolemia, type 2 diabetes, coronary heart disease, prolonged fatigue, and gastrointestinal and respiratory problems, including mortality under the age of 45. Moreover, the most frequent psychological effects are: insomnia, depressive symptoms and the use of psychotropic medication and antidepressants. In professional terms, effects include absenteeism and failure to meet work demands (Salvagioni et al., 2017). Work performance and quality also decline and the perception of occupational risks decreases (Salyers et al., 2017). At the same time, there are major family problems, work-family conflicts and a deterioration in the quality of life (Dyrbye, West, Satele, Sloan, & Shanafelt, 2011; Van der Heijden, Dillingh, Bakker, & Prins, 2008). All these negative repercussions have been studied for decades and are regarded as stress-related symptomatology (SRS).
Given that BS involves a psychosocial risk, several actions have been taken to prevent and treat it (Schaufeli & Taris, 2005). However, there is still no consensus on the most effective forms of intervention to achieve this (Ahola, Toppinen-Tanner, & Seppänen; 2017).
The intervention modalities most commonly used and studied fall into two main categories: (a) organizational, focused on strategies that include training for work, stress reduction, and management and collaborative labor relations and (b) individual, characterized by providing the worker with cognitive-behavioral and relaxation skills that enable them to effectively cope with work-related stress (West, Dyrbye, & Shanafelt, 2018), the latter being those that have shown a greater effect in comparison with the former in the reduction of BS levels and some of their consequences (Dreison et al., 2018).
Some studies on the effectiveness of individual interventions with a cognitive behavioral approach have been conducted with the aim of reducing the risk of developing BS in the teaching population (Bresó, Schaufeli, & Salanova, 2011), students (Ghannam, Afana, Ho, Al-Khal, & Bylund; 2019) and health personnel (Pflugeisen, Drummond, Ebersole, Mundell, & Chen, 2016) showing moderate effects, but little has been studied about their effect in other jobs that involve high demands and stress for workers. In this regard, Dreison et al. (2018) discuss the need to design, implement and evaluate the effect of interventions adapted to the unique needs of each organization and its staff.
In this respect, it is worth mentioning that those who perform functions assigned by the state in public service (known as civil servants) face working conditions that could encourage the development of burn-out, such as: interpersonal conflicts, overload of customer service cases, conflict and role ambiguity, perception of inequity in social exchanges, and lack of control over results Gil-Monte (2002).
In view of the above, and given the need to develop scientific evidence on the effect of psychosocial interventions to reduce BS (West, Dyrbye, Erwin, & Shanafelt, 2016), the objective of this study was to determine the effect of a Cognitive Behavioral Intervention (CBI) on coping rates and BS in a sample of public servants working at an autonomous public institution through an experimental study.
MethodParticipantsA convenience sample of 31 civil servants were randomly assigned to two groups: 15 in the experimental group and 16 in the control group who work in an autonomous public agency responsible for building a culture of respect and defense of human rights in the city of Xalapa, Veracruz, Mexico. All the participants had administrative functions that involved customer service, and the analysis and resolution of complaints filed by citizens to protest violations of their human rights by public servants.
The inclusion criteria were: agreeing to participate in the study, answering the questionnaires and signing an informed consent form. The exclusion criteria were: declaring they were undergoing a psychotherapeutic process and/or receiving psychopharmacological treatment. The main elimination criterion was failing to attend at least six of the eight sessions of the treatment or incorrectly filling in a questionnaire before or after the eight-week treatment.
InstrumentsA specially designed sociodemographic data questionnaire. The questionnaire included the following variables: age, sex, schooling, marital status, having children, seniority in work and religion.
Maslach Burnout Inventory - General Survey adapted to Spanish, comprising 16 items in the form of statements measuring the frequency with which the individual has experienced the characteristic emotions and thoughts of burnout on a scale from 0, never to 6, every day, that explore the degree of: low personal fulfillment at work, emotional exhaustion and depersonalization with Cronbach's alpha indexes of .85, .83 and .74 respectively (Gil-Monte, 2002).
The Scale Measuring Coping with Extreme Risks (López-Vázquez & Marván, 2004), a five-point Likert Scale ranging from 1 (never) to 5 (always). It includes 26 items that measure coping styles through two sub-scales: active coping (finding strategies to cope with situations and dealing with their consequences), and passive coping (strategies of denial, rejection and passive acceptance of the risks involved), with a total Cronbach's alpha of .79 and .76 respectively.
The Stress-Associated Symptoms Inventory created by Benavides, González, Moreno-Jiménez, and Garrosa (2002), consisting of 27 items in which a series of psychosomatic symptoms associated with stress (e.g. aches and pains, rashes, exhaustion, among others) are listed in a Likert format, in which individuals are asked to state the frequency with which these symptoms have been experienced in the past week, on a scale from 0 (never) to 4 (always). The total sum of the answers made it possible for the research to assess the consequences of burnout on the participant's health one-dimensionally, without this information constituting a specific medical diagnosis. The overall reliability of Cronbach's alpha scale was .89.
InterventionA Cognitive Behavioral Intervention (CBI) was designed with the aim of developing strategies in the staff to actively cope with problems based on Psychoeducation (PE) and Problem Solving Therapy (PST) techniques. This type of intervention boosts workers’ resistance and therefore increases the likelihood they will handle work stressors with better results (Schaufeli & Taris, 2005).
Specifically, PST can be defined as a process whereby individuals identify effective solutions for everyday problems, by creating and using a set of cognitive behavioral skills that are implemented flexibly in order to adapt to various stressful scenarios such as the workplace (Ruiz, Díaz, & Villalobos, 2012). The aim of the EP is to provide knowledge for people so that they understand the underlying mechanisms of chronic and acute stress so that they can use this information and handle stress effectively and preserve their health (Daele, Hermans, Van Audenhove, & Van den Bergh, 2012).
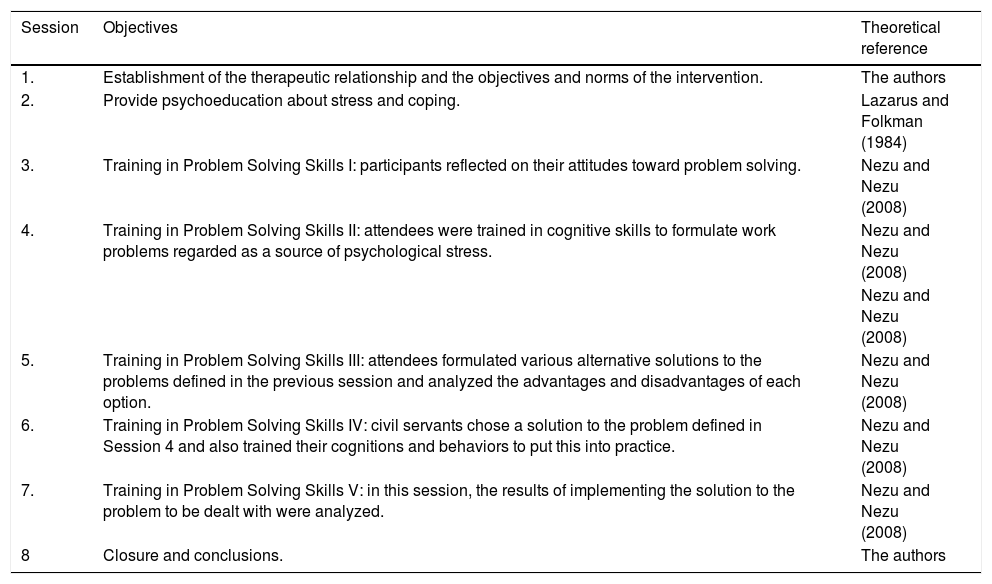
This was a group intervention, involving a two-hour session per week. The eight sessions were designed as in Table 1.
Contents of the cognitive behavioral intervention.
| Session | Objectives | Theoretical reference |
|---|---|---|
| 1. | Establishment of the therapeutic relationship and the objectives and norms of the intervention. | The authors |
| 2. | Provide psychoeducation about stress and coping. | Lazarus and Folkman (1984) |
| 3. | Training in Problem Solving Skills I: participants reflected on their attitudes toward problem solving. | Nezu and Nezu (2008) |
| 4. | Training in Problem Solving Skills II: attendees were trained in cognitive skills to formulate work problems regarded as a source of psychological stress. | Nezu and Nezu (2008) |
| Nezu and Nezu (2008) | ||
| 5. | Training in Problem Solving Skills III: attendees formulated various alternative solutions to the problems defined in the previous session and analyzed the advantages and disadvantages of each option. | Nezu and Nezu (2008) |
| 6. | Training in Problem Solving Skills IV: civil servants chose a solution to the problem defined in Session 4 and also trained their cognitions and behaviors to put this into practice. | Nezu and Nezu (2008) |
| 7. | Training in Problem Solving Skills V: in this session, the results of implementing the solution to the problem to be dealt with were analyzed. | Nezu and Nezu (2008) |
| 8 | Closure and conclusions. | The authors |
The study was carried out with the permission of the authorities responsible for the State Commission for Human Rights, an autonomous public agency located in the city of Xalapa, Veracruz, Mexico.
An orientation session was held to invite civil servants to participate in the research project, who were given information on the form and dates of enrollment in the study. The research was undertaken from November 2016 to May 2017.
Those who signed up for the research project signed an informed consent form and were randomly assigned to one of two groups (control or experimental), with every effort being made to have the same number of participants in each. Subsequently, both the group that would receive the intervention (experimental) and the waiting list group (control) were informed about the sites and the evaluation and intervention dates. The evaluation questionnaires were applied to both groups prior to the start of the intervention and eight weeks later, on completion of the intervention.
The evaluation and intervention sessions were held in a meeting room located in the work center facilities, and were conducted by a therapist with CBI training who knew the members of the control and experimental groups, since he was responsible for the research. Each participant was given a manual explaining the content of each work session and some examples and related exercises. At the end of each session, a randomly selected participant was given a form to evaluate the integrity of the treatment to confirm that the objectives of each session were being covered by the psychologist. The same intervention was given to the control group (which was on the waiting list) after the intervention had been given to the experimental group and the corresponding measurements were taken.
Data analysisThe sociodemographic characteristics of the participants of both groups were described using the mean and standard deviation for continuous variables, as well as frequencies for the categorical ones and the equivalence of all of them was reviewed using the X2 and Student t tests.
The normal distribution of all the variables studied was corroborated by the Kolmogorov–Smirnov test, and comparisons of pre- and post inter- and intra-group scores were made with the Student's t test (paired or independent versions). Moreover, an ANCOVA analysis was undertaken to determine whether the effect of the intervention expressed in the post-test measurement scores was influenced by the scores obtained in the measurement of all the psychological variables prior to the intervention. In addition, the intergroup effect of the intervention was analyzed using Cohen's d test (Cohen, 1969). In all cases, the preset alpha error was α=.05. Data were analyzed using IBM SPSS Statistics 23.0.
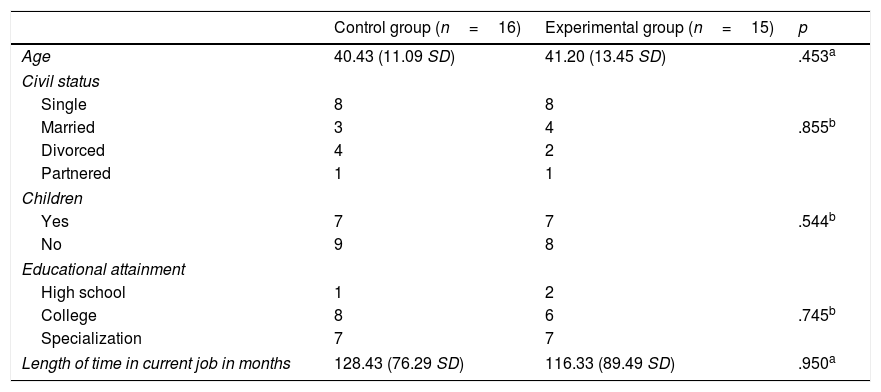
ResultsThe sociodemographic characteristics of the participants in both groups were statistically equivalent and are shown in Table 2.
Sociodemographic data of the groups studied.
| Control group (n=16) | Experimental group (n=15) | p | |
|---|---|---|---|
| Age | 40.43 (11.09 SD) | 41.20 (13.45 SD) | .453a |
| Civil status | |||
| Single | 8 | 8 | |
| Married | 3 | 4 | .855b |
| Divorced | 4 | 2 | |
| Partnered | 1 | 1 | |
| Children | |||
| Yes | 7 | 7 | .544b |
| No | 9 | 8 | |
| Educational attainment | |||
| High school | 1 | 2 | |
| College | 8 | 6 | .745b |
| Specialization | 7 | 7 | |
| Length of time in current job in months | 128.43 (76.29 SD) | 116.33 (89.49 SD) | .950a |
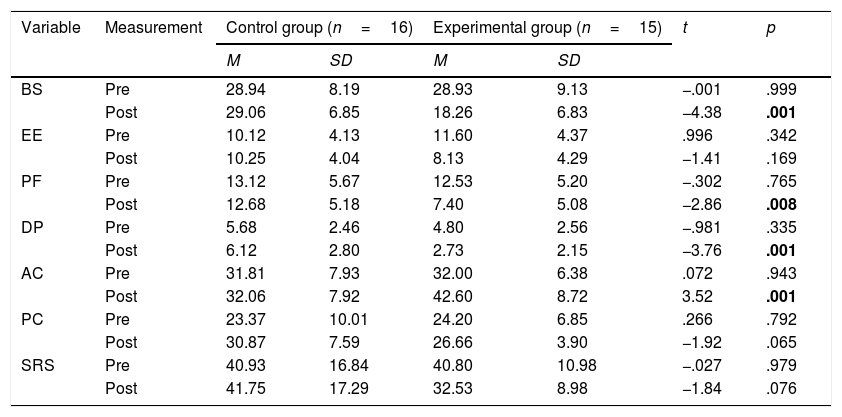
Equivalence was found in the scores of each variable and their respective dimensions before the intervention. After treatment, the control group significantly decreased its levels of BS, PF, DP and increased those of AC compared to the control group as shown in Table 3.
Intergroup comparison of means pre- and post-intervention in all the variables studied.
| Variable | Measurement | Control group (n=16) | Experimental group (n=15) | t | p | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| BS | Pre | 28.94 | 8.19 | 28.93 | 9.13 | −.001 | .999 |
| Post | 29.06 | 6.85 | 18.26 | 6.83 | −4.38 | .001 | |
| EE | Pre | 10.12 | 4.13 | 11.60 | 4.37 | .996 | .342 |
| Post | 10.25 | 4.04 | 8.13 | 4.29 | −1.41 | .169 | |
| PF | Pre | 13.12 | 5.67 | 12.53 | 5.20 | −.302 | .765 |
| Post | 12.68 | 5.18 | 7.40 | 5.08 | −2.86 | .008 | |
| DP | Pre | 5.68 | 2.46 | 4.80 | 2.56 | −.981 | .335 |
| Post | 6.12 | 2.80 | 2.73 | 2.15 | −3.76 | .001 | |
| AC | Pre | 31.81 | 7.93 | 32.00 | 6.38 | .072 | .943 |
| Post | 32.06 | 7.92 | 42.60 | 8.72 | 3.52 | .001 | |
| PC | Pre | 23.37 | 10.01 | 24.20 | 6.85 | .266 | .792 |
| Post | 30.87 | 7.59 | 26.66 | 3.90 | −1.92 | .065 | |
| SRS | Pre | 40.93 | 16.84 | 40.80 | 10.98 | −.027 | .979 |
| Post | 41.75 | 17.29 | 32.53 | 8.98 | −1.84 | .076 | |
BS, burnout syndrome; EE, emotional exhaustion; PF, personal fulfillment; DP, depersonalization; AC, active coping; PC, passive coping; SRS, stress-related symptomatology.
Statistically significant differences are highlighted in bold.
It should be mentioned that, regardless of the statistical differences found after the intervention between groups, when calculating the effect size, all the psychological variables showed changes with a large effect size (d≥.5). Specifically, it was found that in the experimental group, BS, EE, PF, DP, PC and SRS values decreased in comparison with the control group, and the AC variable increased. When the ANCOVA was performed using the pretest measures and the study group as covariates to determine its possible influence on the treatment effects, it was found that the only variable that explained the change was having received the intervention. It should be noted that in all cases, the corrected explained variance was at least .57.
Intragroup comparisonsControl groupA comparison of the pre- and post-intervention values showed that only the PC variable underwent a statistically significant increase (p=.001). In addition, when calculating the effect size, an increase was observed in the DP dimension (d=.16) of BS with a medium effect and on the PC subscale (d=.84) with a large effect.
Experimental groupThe BS variable and its EE, PF and DP dimensions decreased with statistical significance (p=.001); the same was true of the SRS variable (p=.001).
The AC and PC variables increased significantly (p≤.05). When the effect size was calculated, the values of the BS variable and their respective dimensions, as well as the SRS scores decreased with a large effect size in all cases (d≤−.5). AC values increased with large effect (d≥1.38) and PC values with medium effect (d=.44).
DiscussionBurnout and its negative effects on individuals and organizations require studies in various work scenarios on the effects of interventions for its prevention and treatment. This is particularly true since all interventions of this nature must be based on scientific evidence, in other words, with proven effects.
The purpose of this study was to study the effect of a CBI based on PST on BS, AC, PC and SRS indexes in civil servants at an autonomous public agency that defends human rights in a Mexican state. The results show that, compared to a control group on the waiting list, and when intra and intergroup results are combined, civil servants who received the CBI significantly decreased their BS and SRA indexes and increased both AC and PC. In other words, participants who received the CBI developed both cognitive and behavioral and emotion management skills to deal with workplace problems, which translated into a reduction of physical, psychological and social symptoms associated with stress, including an effective decrease in BS indexes.
Two issues must be considered in relation to the control group: (1) during the eight weeks the study lasted, members showed an increase in DP levels, in other words, they began to lose sensitivity and empathy in dealing with other people at work and (2) they began to make more use of PC, which can be understood as a coping mechanism based on emotion. Both conditions show that in the absence of a psychological intervention, members of this group coped with stressors using toxic strategies and therefore saw an increasing evolution of the negative effects of work stress, since they did not focus their cognitive behavioral efforts on the solution of the problems that created work stress, and tended to use emotional control strategies instead.
Kunkler and Whittick (1991) conducted a similar study to the present one, implementing an eight-session intervention using the problem-solving approach in nursing professionals, concluding that the program was effective in reducing burn-out by comparing the post-intervention results between the control and experimental groups. Likewise, a recent systematic review of research assessing the effectiveness of psychological and psychosocial interventions to reduce burnout syndrome in physicians reported that interventions with a behavioral cognitive approach have proved most effective (Clough et al., 2017), despite the methodological difficulties found in the studies reviewed. The main explanation for this is that people learn cognitive skills, which enable them to identify and modify disadaptative thought patterns that trigger unwanted emotions and behaviors in the work sphere and replace them with ones that are better adapted to coping with challenges at work. Nevertheless, further research is required to study the medium- and long-term effect of this type of interventions.
However, the research findings should be understood in the context of their limitations, such as the small sample size and the measurement instruments validated in populations other than the one used in this study. Moreover, future studies should consider the mediating impact certain environmental and relational variables could have on the long-term effect of this type of intervention. We believe it is necessary to assess the relevance of interventions that reinforce and maintain the cognitive-behavioral skills developed in the short term. In addition, it is essential to distinguish the effect of the techniques tested here from placebo effects (results due to a variety of influences related to the beliefs and expectations of the patient and those with whom they interact, as well as contextual signals that can promote change) (Carvalho et al., 2016; Kaptchuk & Miller, 2015).
It should be noted that the professional responsible for this research knew the results of the evaluations before the intervention, which he himself gave. This situation could have interfered with the results through the Pygmalion effect. It is recommended that in subsequent studies, a double blind assignation be included in which neither the therapists nor the participants know the group to which they have been assigned during the intervention nor the results of previous evaluations. Moreover, it is worth mentioning the support the authorities responsible for the administration of the institution where the research was carried out provided by facilitating the physical spaces and timetables for civil servants to attend the intervention, which may have optimized the results of the latter.
In order to find more solid, generalizable results, this study should be replicated at other institutions where civil servants with various functions and degrees of authority work, in order to determine their BS levels and the possible effects of the intervention studied in this research project.
This study suggests that, although there are different types of interventions to prevent or reduce BS, group interventions with a cognitive-behavioral approach designed for civil servants are effective in increasing coping skills and reducing BS rates and associated discomfort, as has been shown in various research projects. This form of intervention has the advantage that it can be carried out in situ, with a simple procedure and adapted to work circumstances. However, these interventions should be designed and implemented by qualified personnel with due methodological care, including, as in this study, a control group and measurements of the integrity of the treatment in order to obtain conclusive findings and with a greater power of generalization in future research.
It is important to consider that the data reported in this and other studies regarding the effect of psychological and psychosocial interventions for burnout treatment or reduction are as yet inconclusive and that more studies are required to achieve solid findings in this respect (Brattberg, 2006; De Vente, Kamphuis, Emmelkamp, & Blonk, 2008; Korczak, Wastian, & Schneider, 2012).
The development of knowledge in relation to psychosocial interventions at work to reduce work stress and its consequences should be a priority for governments and employers. It should also be a priority issue for the public agenda in Latin America, given the limited legislation on mental health at work that exists in the region. Experts and teachers in the field of occupational psychology should recommend the implementation of evidence-based interventions to their clients and students.
General conclusionCBI based on Problem Solving Therapy (Nezu & Nezu, 2008) and Psychoeducation based on the theory of Lazarus and Folkman (1984) undertaken by a trained therapist in the workplace proved effective in increasing AC and decreasing BS and SRS in civil servants.
Conflict of interestsThe authors declare no conflict of interest.