



The incorporation of the provision of aid in dying to the common portfolio of services of the National Health System, after the approval of the Organic Law for the Regulation of Euthanasia (LORE), raises the need to investigate the knowledge of medical professionals about the processes of application of this procedure.
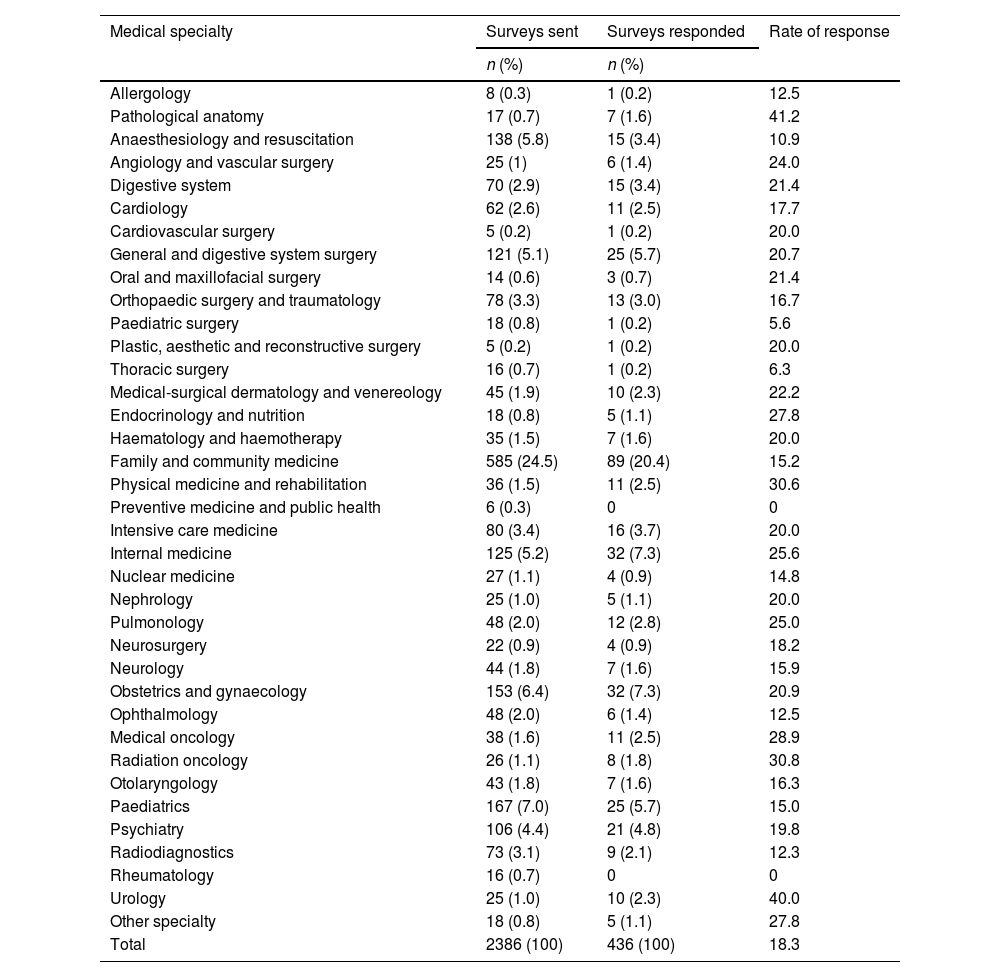
Material and methodsA self-administered online questionnaire of 25 questions was distributed among 2,386 medical practitioners involved in the clinical training of the students enrolled in the Degree in Medicine at the University of Granada.
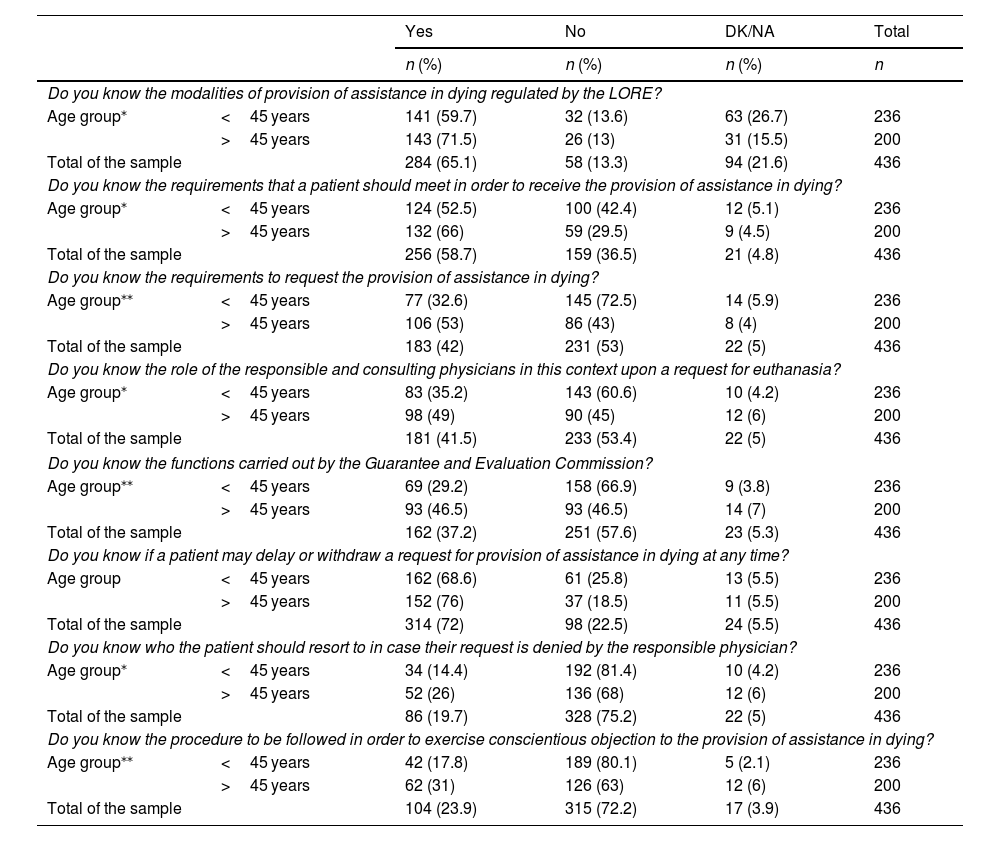
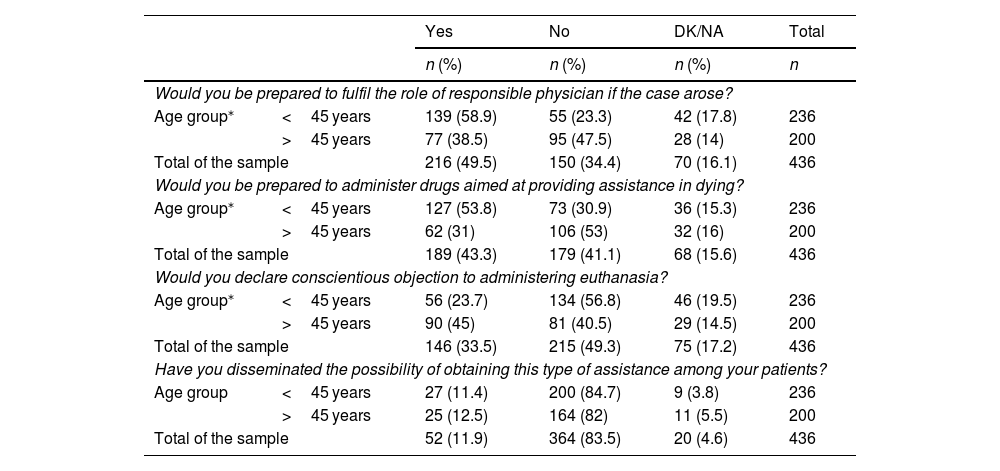
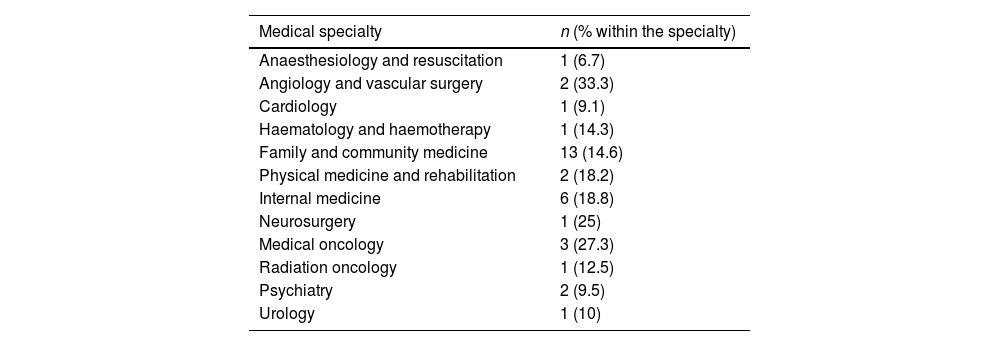
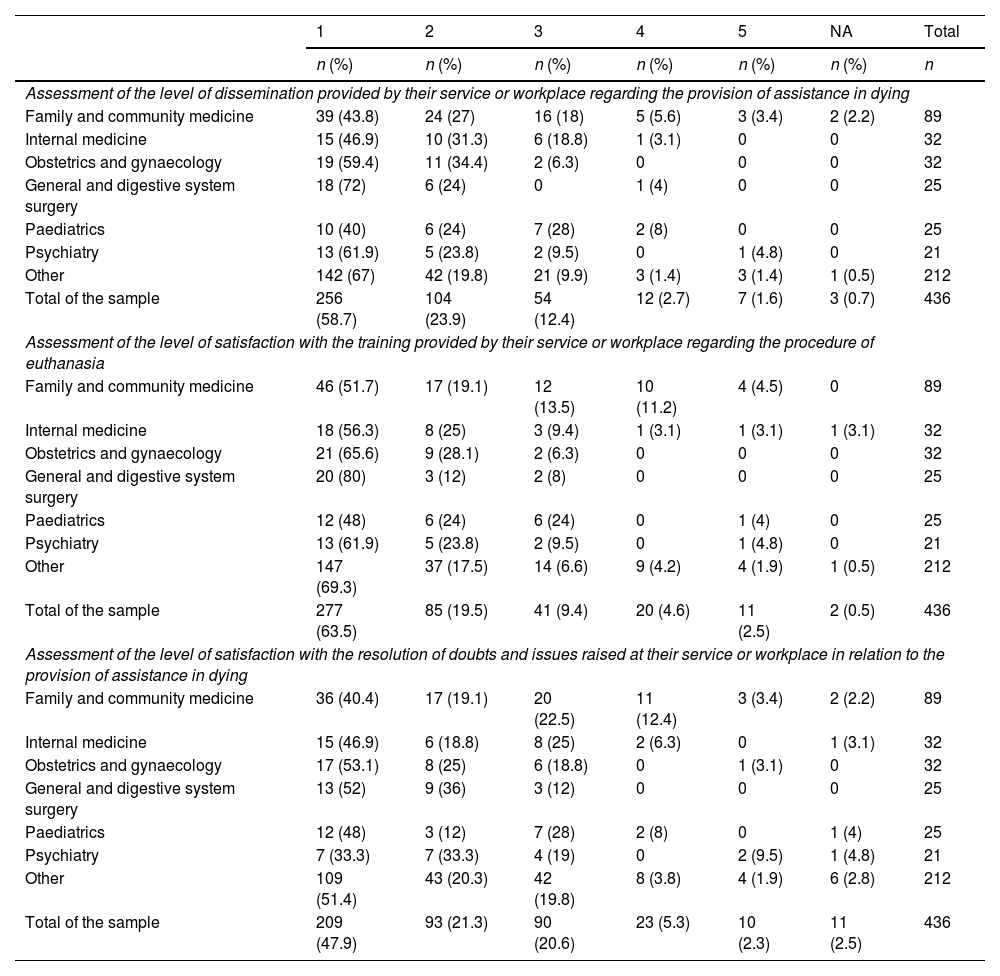
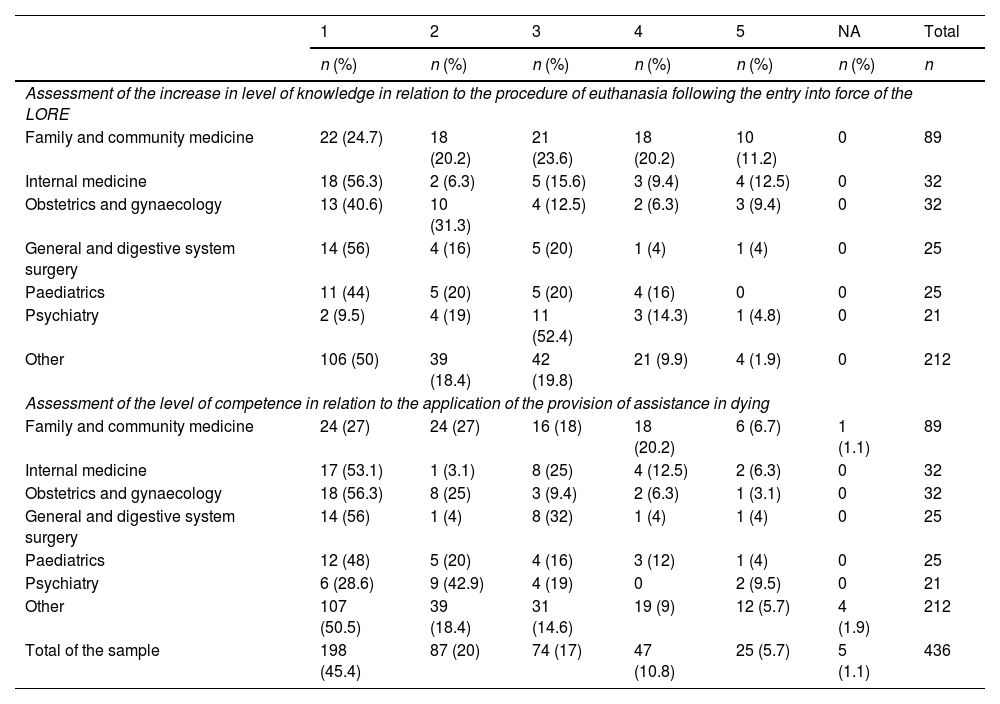
Results436 medical professionals (50.2% women) answered the survey. The specialty of Family and Community Medicine contributed the highest number of participants (20.4%). Around 60% of the physicians did not know the legal requirements that must be met by the patient requesting aid in dying or the role of the responsible physician and the consultant physician. 33.5% of the respondents declared that they would request conscientious objection if necessary and only 14.4% stated that they had received any specific training course in their workplace. More than 80% of the specialists did not consider themselves prepared to deal with this procedure.
ConclusionsThe results of this study indicate that the level of knowledge of the medical professionals surveyed about key aspects of LORE may still be insufficient, pointing out the need to reinforce their training to offer a better response to euthanasia contexts and ensure adequate access to this service for patients.
La incorporación de la prestación de ayuda para morir a la cartera común de servicios del Sistema Nacional de Salud, tras la entrada en vigor de la Ley orgánica de regulación de la eutanasia (LORE), plantea la necesidad de indagar sobre el conocimiento de los profesionales médicos acerca de los procesos de aplicación de este procedimiento.
Material y métodosSe distribuyó un cuestionario online autoadministrado de 25 preguntas entre 2.386 facultativos médicos vinculados con la formación clínica de los estudiantes del grado en Medicina de la Universidad de Granada.
ResultadosEl cuestionario fue respondido por 436 profesionales médicos (50,2% mujeres). La especialidad de Medicina Familiar y Comunitaria fue la que aportó un mayor número de participantes (20,4%). Alrededor del 60% de los encuestados desconocía los requisitos legales que debe cumplir el paciente que solicita la prestación de ayuda para morir o el papel del médico responsable y el médico consultor. El 33,5% de los participantes manifestó que solicitaría la objeción de conciencia llegado el caso. Solo el 14,4% afirmó haber recibido formación específica en su lugar de trabajo. Más del 80% de los especialistas aún no se consideraban preparados para abordar este procedimiento.
ConclusionesLos resultados de este estudio indican que el nivel de conocimiento de los profesionales médicos encuestados sobre aspectos clave de la LORE podría ser todavía insuficiente, señalando la necesidad de reforzar su formación para ofrecer una mejor respuesta ante contextos eutanásicos y asegurar el adecuado acceso de los pacientes a esta prestación.