



Informed consent document (ICD) must be obtained in those cases defined by law. The development of ICD templates by experts in medical scientific societies would ensure the quality of the information procedure.
Method/resultsThis study tracked (October–December 2014) the website of 152 official scientific societies and identified ICD in just 25.66% of them (39 societies); 56.41% of them (22 societies) offered free access to ICD (462 documents), and the others, restricted public access. Among the 17 societies that offered ICD exclusively for members, access was achieved in 6 of them with a total of 52 ICDs obtained. A 19.04% of the specialties assembled the 94.94% above all the ICD founded.
DiscussionThe development and accessibility of ICD built by certain scientific societies is wide in certain specialties; however, despite its enormous potential, in the overall analysis it remains insufficient.
El consentimiento informado precisa ser recogido por escrito en los supuestos establecidos por ley. El desarrollo experto de modelos de documentos de consentimiento informado (DCI) por las sociedades científicas ofrecería garantías a pacientes y profesionales sobre la adecuación del procedimiento de información.
Metodología/resultadosEl presente estudio localizó, entre octubre y diciembre de 2014, las webs de sociedades científicas oficiales (152), identificando DCI en tan solo un 25,66% de ellas (39 sociedades), entre las cuales un 56,41% (22 sociedades) ofrecían los DCI en acceso libre (462 DCI), y las restantes, mediante acceso restringido. Se logró acceso a 6 de las 17 sociedades que ofrecían DCI exclusivos para socios, identificándose 52 DCI más. Un 19,04% de las especialidades agruparon el 94,94% de los DCI localizados.
DiscusiónEl desarrollo y la accesibilidad de DCI elaborados por las sociedades científicas es prolijo en determinadas especialidades, considerándose globalmente insuficiente en el conjunto de sociedades científicas, pese a su enorme potencialidad.
The respect for the patient's right to decide is a fundamental legal principal in health care, whose importance is acknowledged by health professionals.1 This right is exercised through informed consent, the procedure by which the patient, duly informed and competent, freely decides among the clinical options available.2
Both autonomous community3 and national legislation, by way of Law 41/2002, basic regulation on patient autonomy and the rights and obligations in terms of clinical information and documentation,2 establish that consent, as a general rule, will be verbal; however, written consent must be provided in certain cases which are generically described as: “surgical intervention, diagnostic procedures and invasive therapies and, in general, the application of procedures that involve risks and discomforts with a well-known and foreseeable negative impact on the patient's health”.2
Beyond the misguided myths existing regarding the informed consent document (ICD),4 appropriate patient information on the risks and possible alternatives is essential.5,6 It has been reported that the practice and the current standards for informed consent are often not useful for the patient and carry unnecessary risks in terms of medical professional responsibility for professionals.7,8 While patient information must be personalized, expert development of personalized ICD templates is recommended, increasing the guarantees for patients and professionals. This is being done by commissions designated for this purpose by autonomous communities9 or scientific societites,10 and they have been legally used as a standard of appropriate information.11,12 Access to and availability of those ICDs is basic, given that it guarantees patient autonomy and can serve to support professionals.
This study analyses the availability of such ICD templates through the official websites of the Spanish scientific societies.
MethodologyA list of 174 scientific societies was created based on the list of Scientific Societies of Health Professionals of the Ministry of Health, Social Services and Equality13 and the List of Spanish Medical Societies of MediRank.14 Between October and December 2014, we investigated whether the different societies had webpages, if reference was made to the ICDs in these, and if ICDs were available online, recording the access route to them (limited to members or open). Those societies which had a webpage but did not have an ICD on the webpage (whether open or with limited access) were contacted by email to ask whether they had developed an ICD, and if so, the way of accessing this.
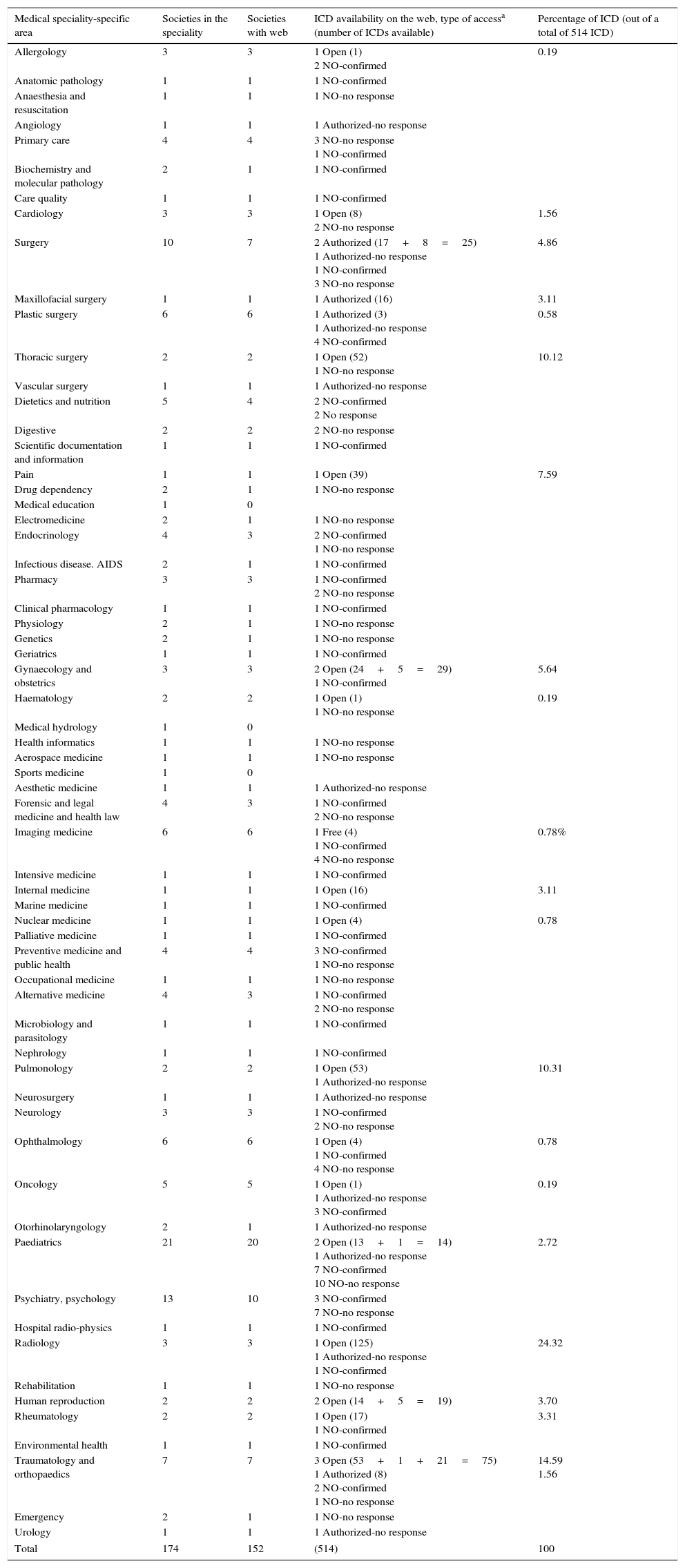
ResultsOf the 174 scientific societies, a total of 22 (12.64%) were excluded from the study as not having an official webpage. In the webpages of the remaining 152 (87.36%) societies, only 39 explicitly contain an ICD (25.66%), 22 of them through an open access section and the other 17 with restricted or authorized access. In the specific section of the 22 webpages with open access, a total of 462 ICDs were located. Contact was made with the 17 societies that requested authorized request, and we obtained a response in only 35.29% of cases (n=6). Among these we located another 52 ICDs, which, added to the 462 ICDs registered in open access, made a total of 514 registered ICDs. 113 scientific societies that did not contain ICDs in their webpage were contacted by email, obtaining responses from 53 of them (46.9%); all confirmed that they had not developed ICDs. No response was obtained from the remaining 60. The results are shown in Table 1. The table, for better understanding, groups the different societies together by each speciality, indicating in another column the number of societies which, within this group of specialities, have an official webpage. Finally, in another column, the type of access to ICDs registered for each of the groups of different specialities is shown, indicating in parentheses, in the event that the ICD was located, regardless of the type of access, the number of ICDs located.
Accessibility to informed consent documents from scientific societies grouped by medical speciality.
| Medical speciality-specific area | Societies in the speciality | Societies with web | ICD availability on the web, type of accessa (number of ICDs available) | Percentage of ICD (out of a total of 514 ICD) |
|---|---|---|---|---|
| Allergology | 3 | 3 | 1 Open (1) 2 NO-confirmed | 0.19 |
| Anatomic pathology | 1 | 1 | 1 NO-confirmed | |
| Anaesthesia and resuscitation | 1 | 1 | 1 NO-no response | |
| Angiology | 1 | 1 | 1 Authorized-no response | |
| Primary care | 4 | 4 | 3 NO-no response 1 NO-confirmed | |
| Biochemistry and molecular pathology | 2 | 1 | 1 NO-confirmed | |
| Care quality | 1 | 1 | 1 NO-confirmed | |
| Cardiology | 3 | 3 | 1 Open (8) 2 NO-no response | 1.56 |
| Surgery | 10 | 7 | 2 Authorized (17+8=25) 1 Authorized-no response 1 NO-confirmed 3 NO-no response | 4.86 |
| Maxillofacial surgery | 1 | 1 | 1 Authorized (16) | 3.11 |
| Plastic surgery | 6 | 6 | 1 Authorized (3) 1 Authorized-no response 4 NO-confirmed | 0.58 |
| Thoracic surgery | 2 | 2 | 1 Open (52) 1 NO-no response | 10.12 |
| Vascular surgery | 1 | 1 | 1 Authorized-no response | |
| Dietetics and nutrition | 5 | 4 | 2 NO-confirmed 2 No response | |
| Digestive | 2 | 2 | 2 NO-no response | |
| Scientific documentation and information | 1 | 1 | 1 NO-confirmed | |
| Pain | 1 | 1 | 1 Open (39) | 7.59 |
| Drug dependency | 2 | 1 | 1 NO-no response | |
| Medical education | 1 | 0 | ||
| Electromedicine | 2 | 1 | 1 NO-no response | |
| Endocrinology | 4 | 3 | 2 NO-confirmed 1 NO-no response | |
| Infectious disease. AIDS | 2 | 1 | 1 NO-confirmed | |
| Pharmacy | 3 | 3 | 1 NO-confirmed 2 NO-no response | |
| Clinical pharmacology | 1 | 1 | 1 NO-confirmed | |
| Physiology | 2 | 1 | 1 NO-no response | |
| Genetics | 2 | 1 | 1 NO-no response | |
| Geriatrics | 1 | 1 | 1 NO-confirmed | |
| Gynaecology and obstetrics | 3 | 3 | 2 Open (24+5=29) 1 NO-confirmed | 5.64 |
| Haematology | 2 | 2 | 1 Open (1) 1 NO-no response | 0.19 |
| Medical hydrology | 1 | 0 | ||
| Health informatics | 1 | 1 | 1 NO-no response | |
| Aerospace medicine | 1 | 1 | 1 NO-no response | |
| Sports medicine | 1 | 0 | ||
| Aesthetic medicine | 1 | 1 | 1 Authorized-no response | |
| Forensic and legal medicine and health law | 4 | 3 | 1 NO-confirmed 2 NO-no response | |
| Imaging medicine | 6 | 6 | 1 Free (4) 1 NO-confirmed 4 NO-no response | 0.78% |
| Intensive medicine | 1 | 1 | 1 NO-confirmed | |
| Internal medicine | 1 | 1 | 1 Open (16) | 3.11 |
| Marine medicine | 1 | 1 | 1 NO-confirmed | |
| Nuclear medicine | 1 | 1 | 1 Open (4) | 0.78 |
| Palliative medicine | 1 | 1 | 1 NO-confirmed | |
| Preventive medicine and public health | 4 | 4 | 3 NO-confirmed 1 NO-no response | |
| Occupational medicine | 1 | 1 | 1 NO-no response | |
| Alternative medicine | 4 | 3 | 1 NO-confirmed 2 NO-no response | |
| Microbiology and parasitology | 1 | 1 | 1 NO-confirmed | |
| Nephrology | 1 | 1 | 1 NO-confirmed | |
| Pulmonology | 2 | 2 | 1 Open (53) 1 Authorized-no response | 10.31 |
| Neurosurgery | 1 | 1 | 1 Authorized-no response | |
| Neurology | 3 | 3 | 1 NO-confirmed 2 NO-no response | |
| Ophthalmology | 6 | 6 | 1 Open (4) 1 NO-confirmed 4 NO-no response | 0.78 |
| Oncology | 5 | 5 | 1 Open (1) 1 Authorized-no response 3 NO-confirmed | 0.19 |
| Otorhinolaryngology | 2 | 1 | 1 Authorized-no response | |
| Paediatrics | 21 | 20 | 2 Open (13+1=14) 1 Authorized-no response 7 NO-confirmed 10 NO-no response | 2.72 |
| Psychiatry, psychology | 13 | 10 | 3 NO-confirmed 7 NO-no response | |
| Hospital radio-physics | 1 | 1 | 1 NO-confirmed | |
| Radiology | 3 | 3 | 1 Open (125) 1 Authorized-no response 1 NO-confirmed | 24.32 |
| Rehabilitation | 1 | 1 | 1 NO-no response | |
| Human reproduction | 2 | 2 | 2 Open (14+5=19) | 3.70 |
| Rheumatology | 2 | 2 | 1 Open (17) 1 NO-confirmed | 3.31 |
| Environmental health | 1 | 1 | 1 NO-confirmed | |
| Traumatology and orthopaedics | 7 | 7 | 3 Open (53+1+21=75) 1 Authorized (8) 2 NO-confirmed 1 NO-no response | 14.59 1.56 |
| Emergency | 2 | 1 | 1 NO-no response | |
| Urology | 1 | 1 | 1 Authorized-no response | |
| Total | 174 | 152 | (514) | 100 |
Open (ICD available with open access); Authorized (ICD available with restricted access); Authorized-no response (ICD presumably available with restricted access, unsuccessful attempt to contact by email); NO-confirmed (no availability of ICD confirmed); NO-no response (no ICD on line, unsuccessful attempt to contact by email.
Accessibility to ICDs by professionals is key. This study appropriately reflects, in our opinion, the accessibility that professionals from different specialities have to ICDs through the websites of their scientific societies, given that the available ICDs were located through 71.8% of the websites that had a dedicated space for these. No other studies have been found that analyze the ICDs available through scientific societies.
Although most of the scientific societies identified have an official webpage (87.35%), of those only 25.66% devote a space on their website to ICDs and therefore, it can be understood that the majority of the scientific societies have not specifically worked on the patient information process within their speciality nor have they prioritized the dissemination of the work in that respect. This is a striking result when the vast majority of specialities provide for the completion of procedures for written consent.
Furthermore, the mean of ICDs by speciality among those did have them was 18.35. 19.04% (12) of the 63 specialities identified registered 94.94% (488) of the 514 ICDs located: up to 24.32% of the total of ICDs in the specialities of Radiology (125), followed by Traumatology and Orthopaedics (83), Pulmonology (53), Thoracic Surgery (52), Pain Treatment (39), Gynaecology and Obstetrics (29), Surgery (25), Human Reproduction (19), Rheumatology (17), Maxillofacial Surgery (16), Internal Medicine (16) and Paediatrics (14). This may reflect the multiplicity of procedures that fall under these specialities requiring written consent and/or special sensitivity in these scientific societies towards patient autonomy and legal safety with regard to professionals (among them are specialities with a greater number of claims for presumed medical professional liability in our environment).15 This second option may be fundamental if we consider the existence of specialities that involve procedures requiring written consent and in which we confirmed the lack of development of an ICD by the corresponding scientific societies.
On the other hand, and maybe as a limitation to this study, there are specialities in which not all interventions require the development of an ICD.
Lastly, 56.41% of societies with ICDs and 89.88% of the ICDs located are provided with open access, which exemplifies the function of information dissemination of these documents and of the societies that create them.
Although patient information is a fundamental part of health care, there are currently few scientific societies that make efforts to establish standards in the information process in the area of their speciality and to optimize their dissemination through official websites. On the other hand, those that do so, create a considerable amount of ICDs as a sample of the potential of this work.
We consider that the development of ICD templates by the scientific societies would establish a framework of better guarantees for professionals and patients for the benefit of patient rights and the legal safety of professionals.
FundingThere is no funding.
Conflict of interestThere is no conflict of interest.
Please cite this article as: Gómez-Durán EL, Ferran-Ballús B, Torrent Jansà L, Martin-Fumadó C, Arimany-Manso J. Accesibilidad a documentos de consentimiento informado a través de las sociedades científicas. Rev Esp Med Legal. 2016;42:67–71.