



Synovial chondromatosis is an uncommon lesion characterized by cartilaginous metaplasia of the synovial layer with the usual formation of free osteocartilaginous bodies and typically involving large joints. Location in the ankle and foot is rare and, in turn, very rare in the synovial sheath of the foot tendons. The diagnosis of this little recognized entity is of great importance because it is a progressive condition that carries a substantial risk of local recurrence. Imaging tests such as CT or MRI help to identify the characteristic findings and the exact location to guide the orthopaedic surgeon in surgery. Its definitive treatment is surgical, through complete resection of the synovium (synovectomy).
La condromatosis sinovial es una lesión poco frecuente que se caracteriza por la metaplasia cartilaginosa de la membrana sinovial con la habitual formación de cuerpos libres osteocartilaginosos y que típicamente afecta grandes articulaciones. La localización en el tobillo y en el pie es poco frecuente y, a su vez, muy rara en la vaina sinovial de los tendones del pie. El diagnóstico de esta entidad poco reconocida es de gran importancia porque es una condición progresiva que conlleva un riesgo sustancial de la recidiva local. Las pruebas de imagen como la TC o la RM ayudan a identificar los hallazgos característicos y la localización exacta para así orientar al traumatólogo en la cirugía. Su tratamiento definitivo es quirúrgico, mediante resección completa de la sinovial (sinovectomía).
Synovial chondromatosis is an uncommon lesion of unknown etiology, characterized by cartilaginous metaplasia of the synovial membrane of small and large joints, with the usual formation of loose osteocartilaginous bodies and a variable degree of joint destruction.1
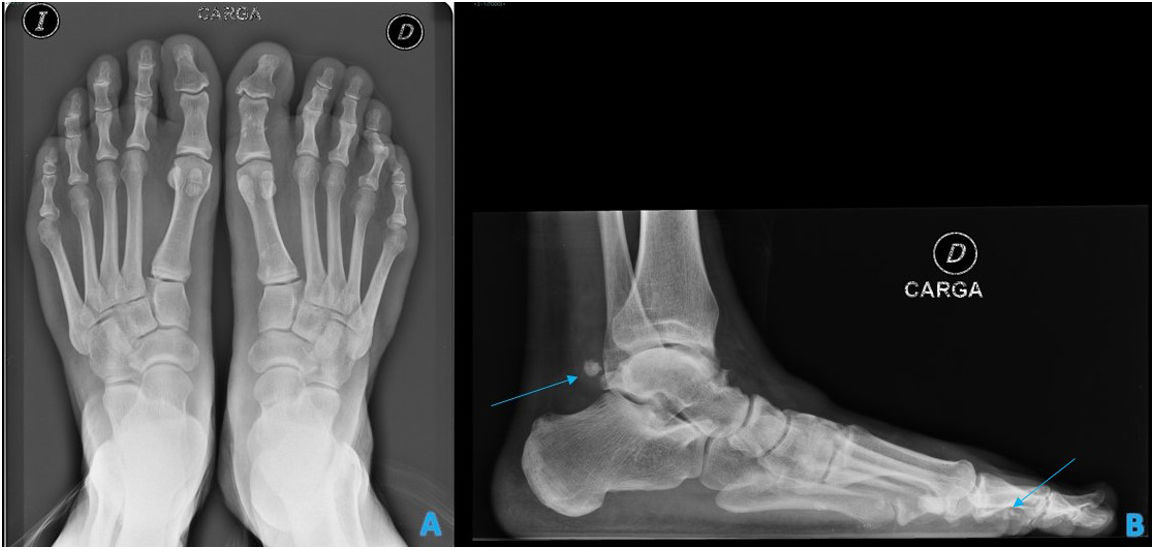
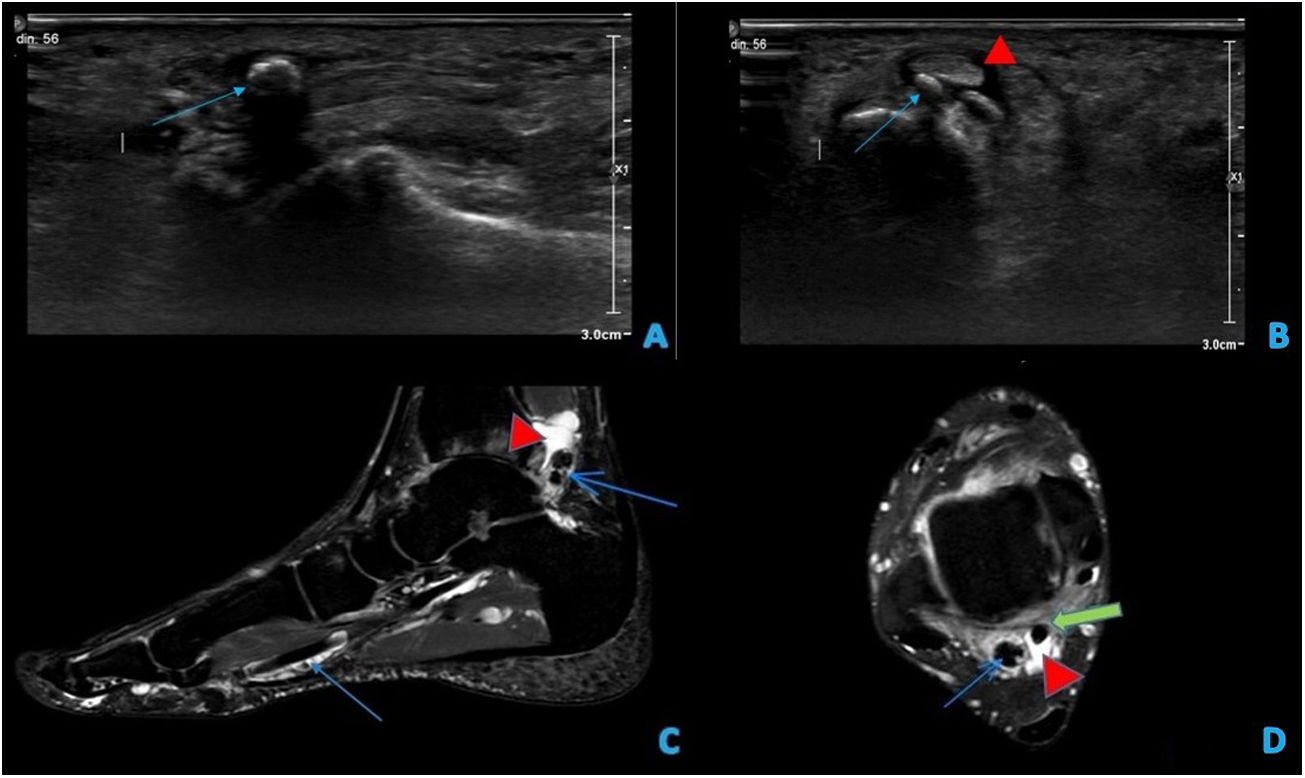
Case presentationWe present a 52year-old man who attended a traumatology consultation due to a tumor in the plantar area of the first toe of the right foot, without associated trauma, although he did have previous pain in the distal phalanx of the first toe of said foot, which was progressively relieved coinciding with the appearance of the tumor. On physical examination, a soft plantar lump was palpable in the region of the first intermetatarsal space. A weight-bearing radiograph was performed, which revealed “popcorn” calcifications in the soft tissues of the plantar aspect of the first phalanx of the big toe of the right foot and in the ankle (Fig. 1). It was decided to complete the study with ultrasound and magnetic resonance imaging (MRI) without contrast. In the first, fluid was visualized in the synovial sheath of the flexor hallucis longus, compatible with tenosynovitis, as well as multiple calcified images, without color Doppler signal, located inside the sheath of this tendon (Fig. 2A,B), along with marked subcutaneous edema in the sole of the foot. The MRI allowed to establish the definitive diagnosis, which confirmed the presence of numerous synovial calcifications in the sheath of the flexor hallucis longus, a finding related to synovial chondromatosis (Fig. 2C,D).
 and lateral projections (B). Several high-density images with rounded morphology suggestive of calcifications are visualized in the region of the tendons of the posterior compartment, as well as in the plantar fascia of the hallux (arrows).")
Simple weight-bearing standing X-ray of the right foot with anteroposterior (A) and lateral projections (B). Several high-density images with rounded morphology suggestive of calcifications are visualized in the region of the tendons of the posterior compartment, as well as in the plantar fascia of the hallux (arrows).
 Ultrasound images of the right foot showing anechoic fluid in the tendon sheath of the flexor propria of the big toe (flexor hallucis longus) in relation to tenosynovitis (red arrowhead), as well as hyperechoic foci within the sheath representing the calcified chondral foci (blue arrow). (C,D) MRI images of the right foot, T2 sequence with sagittal (C) and axial fat suppression located in the ankle (D). Fluid is observed in the sheath of the flexor tendon propria of the first finger (red arrowhead: liquid; green arrow: tendon) with numerous calcifications inside, both at its insertion and as it passes through the ankle, visualized as hypointense and rounded foci (blue arrows).")
(A,B) Ultrasound images of the right foot showing anechoic fluid in the tendon sheath of the flexor propria of the big toe (flexor hallucis longus) in relation to tenosynovitis (red arrowhead), as well as hyperechoic foci within the sheath representing the calcified chondral foci (blue arrow). (C,D) MRI images of the right foot, T2 sequence with sagittal (C) and axial fat suppression located in the ankle (D). Fluid is observed in the sheath of the flexor tendon propria of the first finger (red arrowhead: liquid; green arrow: tendon) with numerous calcifications inside, both at its insertion and as it passes through the ankle, visualized as hypointense and rounded foci (blue arrows).
Synovial chondromatosis originates from a metaplasia of the connective tissue of the synovial membrane, resulting in a multinodular cartilaginous proliferation. It was described for the first time in 1923 by Henderson and Jones.1 The involvement is usually monoarticular and it is most frequent in men between the third and fifth decades of life. Although the location in the ankle and in the foot is uncommon, several cases have been reported in the tibiotalar joint.1
The development of this pathology is classified into three phases: the first, active synovitis without the presence of articular cartilaginous bodies; the second, or transitional phase, shows nodular synovitis along with loss of chondral bodies in the joint; in the third, the chondral bodies persist but the synovitis is resolved.2
Clinical manifestations are variable and depend on the location and the stage of the disease; they range between episodes of joint inflammation and sensation of blockage, joint pain, palpable mass and paresthesia due to compression of neurovascular structures.3
Diagnosis is of great importance because of possible local recurrences. It is possible to detect it on X-rays if there are joint erosions and degenerative arthropathy secondary to the damage of the articular cartilage, a product of the joint loose bodies. However, it must be kept in mind that in 30% of the cases the chondral nodules are not seen when they are not calcified; likewise, X-rays are not sensitive to detect early changes in the synovial membrane, only a decrease in the joint space is observed.4 Computed tomography is also a valid diagnostic method and is more useful in stage 3 by the presence of calcium deposits on the cartilaginous metaplasia of the synovial membrane. Finally, MRI is also a recommended method that allows the detection of synovial alterations even in earlier stages, making it possible to visualize nodules or thickenings of the synovium that can guide the diagnosis.1 The nodules of hyaline cartilage show low signal intensity in T1-weighted sequences and high signal intensity in T2-weighted sequences due to their high aqueous content, but areas of calcification or ossification provide low signal in both sequences.4 However, the definitive diagnosis will be established by anatomopathological analysis of the synovial biopsy, visualizing the presence of nodules of mature hyaline cartilage on the subsynovial layer of the synovial membrane and of nodules of mature cartilage with a central ossification and an osteoblastic ring.1,3
Regarding treatment, although conservative therapy may be sufficient for non-weight bearing joints, such as the shoulders, surgical intervention should be considered to prevent degenerative joint changes. The proposed treatments range from an arthroscopic synovectomy in joints such as the knee and the hip, accompanied by resection of articular loose bodies, to a wide, open synovectomy, and eventually arthroplasty or arthrodesis in situations of advanced joint involvement.5 Total synovectomy is particularly important for the prevention of relapses. Compared with the open technique, the recovery time in arthroscopic procedures is shorter, and there is no need for postoperative inmobilization.6 Complete excision of the inflamed synovium is ideal in the case of tenosynovial chondromathosis.7
The prognosis is variable, and it has been reported a recurrence rate of 22% in the case of open synovectomy with resection of loose bodies in the hip joint.1,3 On the other hand, it is of great importance to consider the possibility of neoplastic transformation of this pathology, which has occurred in 5% of the cases described in the literature and with the type of low-grade chondrosarcoma.1,5
In conclusion, synovial chondromatosis is a rare pathology if we consider the ankle and foot joints, but the radiologist must be aware of this condition in order to establish an accurate diagnosis and guide the traumatologist in the treatment. Likewise, knowledge of its prognosis and its possibility of malignant transformation is of great relevance.
Protection of people and animalsThe authors state that no experiments have been conducted on humans or animals for this research.
Data confidentialityThe authors state that they have followed the protocols of their workplace regarding the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare they have no conflict of interest.
